 JANIFEST/ISTOCK/GETTY IMAGES PLUS
JANIFEST/ISTOCK/GETTY IMAGES PLUS
Caries Risk of E-Cigarette Use
While evidence is limited, vaping may contribute to increased caries experience and other negative health effects.
This course was published in the December 2020 issue and expires December 2023. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the risks associated with e-cigarette use, or vaping.
- Discuss the cariogenic properties of e-cigarettes.
- Explain the role of oral health professionals in addressing the risks associated with vaping.
Dental caries is a complex, multifactorial disease with many etiologic factors, including diet, composition of oral bacteria, level of salivary flow, immune system and host response, effectiveness of oral hygiene regimen, presence of community water fluoridation, fluoride exposure, and access to dental care.1 Electronic cigarette (e-cigarette) ingredients and properties may also create an oral environment more conducive to caries.
Caries is caused by an imbalance in the oral bacteria present, creating dental biofilm. The biofilm feeds off dietary fermentable carbohydrates, creating acids that eventually demineralize the tooth surface.1 E-cigarette flavors that are sweet or low pH can increase biofilm formation when exposed to caries-producing Streptococcus mutans.2 Nicotine also enhances S.mutans biofilm metabolic activity and formation.3 Additionally, e-cigarettes contain ingredients that resemble gelatinous candies and acidic drinks when interacting with hard tissues of the oral cavity,2 and their use can cause hyposalivation, which is proven to raise caries incidence.1,3–6 This article will look at the oral health effects of e-cigarette use, including caries risk, in addition to discussing evidence-based cessation strategies.
E-Cigarette Risks to Oral and Systemic Health
E-cigarettes were first introduced in the early 2000s to deliver nicotine without tobacco combustion.7–9 In 2014, the United States Food and Drug Administration (FDA) labeled e-cigarettes a tobacco product, as they contain nicotine derived from tobacco plants. In 2016, the FDA began regulating all tobacco products, including electronic nicotine delivery systems (ENDS).10 While the FDA regulates the manufacture, import, packaging, labeling, advertising, promotion, sale, and distribution of ENDS, there are no FDA-approved ENDS currently on the market.
ENDS are known by many names, including vapor pens, e-hookah, and vape pipes. The use of these devices is often referred to as “vaping.”7 While 44% of the general population believe that e-cigarettes are “safer” than traditional combustible cigarettes (CCs) because they do not contain as many chemical components, their use does expose users to nicotine and other toxic substances.11,12 E-cigarettes create an inhalable aerosol (commonly, though incorrectly, called vapor) via heating a liquid containing propylene glycol or glycerin along with nicotine, flavoring, and other additives.7–9,11 Marketing often states that e-cigarettes produce only “harmless water vapor,” when in reality they create an aerosol of ultrafine particles. While strong evidence suggests that frequent, low-level exposure to particles from CC smoke or air pollution can increase the risk of pulmonary inflammation and cardiovascular and respiratory diseases, it is not clear whether e-cigarette aerosols exert the same negative health effects.8 Only a few studies have explicitly researched the health effects of e-cigarette aerosol exposure, but some do show the ability of aerosols to cause biological effects. Some of the health effects noted are upper respiratory tract irritation, constricting of peripheral airways, cough, nausea, and vomiting.5,7,13,14 An observational study in 2011 reported mouth irritation, sore throat, dry mouth, and oral ulcers after 4 weeks of e-cigarette use.5 In another study of adolescents, e-cigarettes were associated with an increased risk of cracked or broken teeth, or tongue/oral mucosal pain.15 Additionally, periodontal diseases may be more common among users due to exposure to nicotine, oxidants, and particulates.5,7
Vaping products may increase the risk for SARS-CoV-2-related respiratory disease because their use can cause acute pulmonary toxicity. Aerosols generated by ENDS may also aid in the transmission of the novel coronavirus.16 Additionally, e-cigarette, or vaping, product use-associated lung injury has been found in users whose ENDS contained vitamin E acetate.
The flavoring chemicals used in ENDS, such as diacetyl and acetyl propionyl, can cause “popcorn lung” or bronchiolitis obliterans. In vitro research found that chocolate and cinnamon flavors in ENDS produced cytotoxic effects, oxidative stress, and inflammation.17 Many ENDS manufacturers note that the flavoring chemicals used are “food grade” and “generally recognized as safe” (GRAS). However, the GRAS certification provided by the Flavor Extracts Manufacturers Association pertains only to ingestion, not inhalation.18 Also, amid a drastic rise in ENDS use by adolescents who are often attracted by flavors, the FDA prohibited the manufacture and distribution of ENDS products with flavors, such as fruit and mint, that appeal to children in January 2020.19 However, this policy does not apply to the sale of flavors for tank-based systems.
One of the purported benefits of ENDS is their role in helping traditional smokers quit. However, this premise is fraught with controversy.15 The American Dental Association does not recommend the use of e-cigarettes as a method to quit smoking or as an alternative, “less harmful” form of tobacco.20 The American Medical Association and the American Heart Association have similar views and prioritize the prevention of any type of tobacco use.20
Cariogenic Properties of E-Cigarettes
Research shows that nicotine exposure via traditional smoking increases caries risk.21–23 Nicotine enhances S.mutans biofilm metabolic activity and formation.3 When comparing current smokers to nonsmokers in Japan, Ojima et al22 found that smokers had significantly increased need for restorative treatment than nonsmokers. Another study of truck drivers discovered that the number of carious lesions present increased compared to how many cigarettes were smoked each day.23 However, similar research has yet to be conducted on the relationship between e-cigarette use. Exposure to nicotine may also cause swelling and inflammation of the palatal minor salivary glands; however, the clinical significance of this finding remains to be confirmed.17
E-cigarettes contain ingredients that, when interacting with the hard tissues of the oral cavity, resemble gelatinous candies and acidic drinks that adversely affect teeth.2 It is well-known that sucrose exposure increases caries risk, and, in some ENDS, sucrose has been found in samples of e-liquids, even though it is not listed as an ingredient on the product label.24 The source of sucrose in e-liquids is unknown, but it may come from sweet flavorings or from tobacco leaves.25
The aerosols generated by e-liquids are likely to adhere to any exposed hard or soft surface, including those of the oral cavity. This is due to the viscous nature of e-liquids and their glycerin base.2,26 As the ability of cariogenic bacteria to adhere to surfaces and form biofilm is influenced by surface roughness, the viscousness of e-cigarette aerosols may change surface characteristics, making the oral cavity more conducive to dental caries.2,17 Kim et al2 evaluated the impact of e-cigarette liquid ingredients—sucralose, ethyl butyrate, triacetin, and hexyl acetate—in the presence of Streptococcus mutans, and found they significantly increased biofilm formation, compared with an unflavored e-liquid control. Study authors suggest that esters, such as the ones in e-liquid flavors, provide a supplementary food source for S.mutans in oral biofilm. Additionally, they surmise that S.mutans attach to the aerosol-exposed surface and metabolize the base and flavors of the e-liquid to form a biofilm that demineralizes the enamel surface.2 As these data are preliminary, more research on the subject is necessary.
E-cigarette use may increase the risk for xerostomia, which undoubtedly raises caries risk.1,4–6,27 In a survey of United States adults who used e-cigarettes, 31% reported experiencing dry mouth or throat.28 A 2011 observational study found that after 4 weeks of vaping, e-cigarette users reported experiencing dry mouth, in addition to mouth irritation, sore throat, and oral ulcers.5 As saliva aids in the development of the dental pellicle, the film that forms on the tooth and protects it against mineral loss, its absence or reduction can leave tooth structure open to a cariogenic attack. Saliva also replenishes the tooth surface with minerals such as calcium and phosphate, and provides antibacterial and buffering activity, keeping the oral pH neutral. Lastly, it aids in the mechanical removal of residual food particles from the teeth. A lack of saliva exposes the teeth to acidic challenges from food and beverages and bacteria-produced acid. Demineralization occurs when the acids dissolve the calcium and phosphate ions from the enamel. With the loss of saliva buffering capacity, the oral pH drops and demineralization occurs, leading to carious lesions.27,29
Caries Risk Assessment
Caries risk assessment is essential for all patients, including e-cigarette users. Updated “caries management by risk assessment,” or CAMBRA tools should be implemented to develop an individualized risk-based treatment plan combining minimally invasive treatment strategies and restorative therapy, if necessary.1,4 Patients’ risk levels are determined by evaluating disease indicators, risk factors, and preventive factors via a caries risk assessment form.30 After determining whether a patient is low, moderate, or high risk, lifestyle is discussed and minimally invasive therapies, such as fluoride, antimicrobials, and calcium phosphate products, are recommended.29
If a patient indicates on the health history that they are using e-cigarettes, especially those with sweet flavors, clinicians should inform him or her that this is a potential risk factor for caries and suggest caries-mitigating strategies.4

Tobacco Cessation
While the use of CCs has been declining in the US for decades, the popularity of vaping continues to grow. Since 2014, e-cigarettes have been the most common form of tobacco product used by US middle and high school students.7,8,20 As such, dental hygienists need to provide comprehensive tobacco prevention planning for patients that addresses all tobacco products, not just CCs.8,20
All patients should be asked about tobacco use, including e-cigarette use, during the medical history, and those who disclose use should be provided with cessation strategies.20,31 Patients who express interest in using vaping to quit traditional smoking should be advised on potential health effects. No form of tobacco or nicotine exposure is safe and the long-term health risks of e-cigarettes are unknown.20
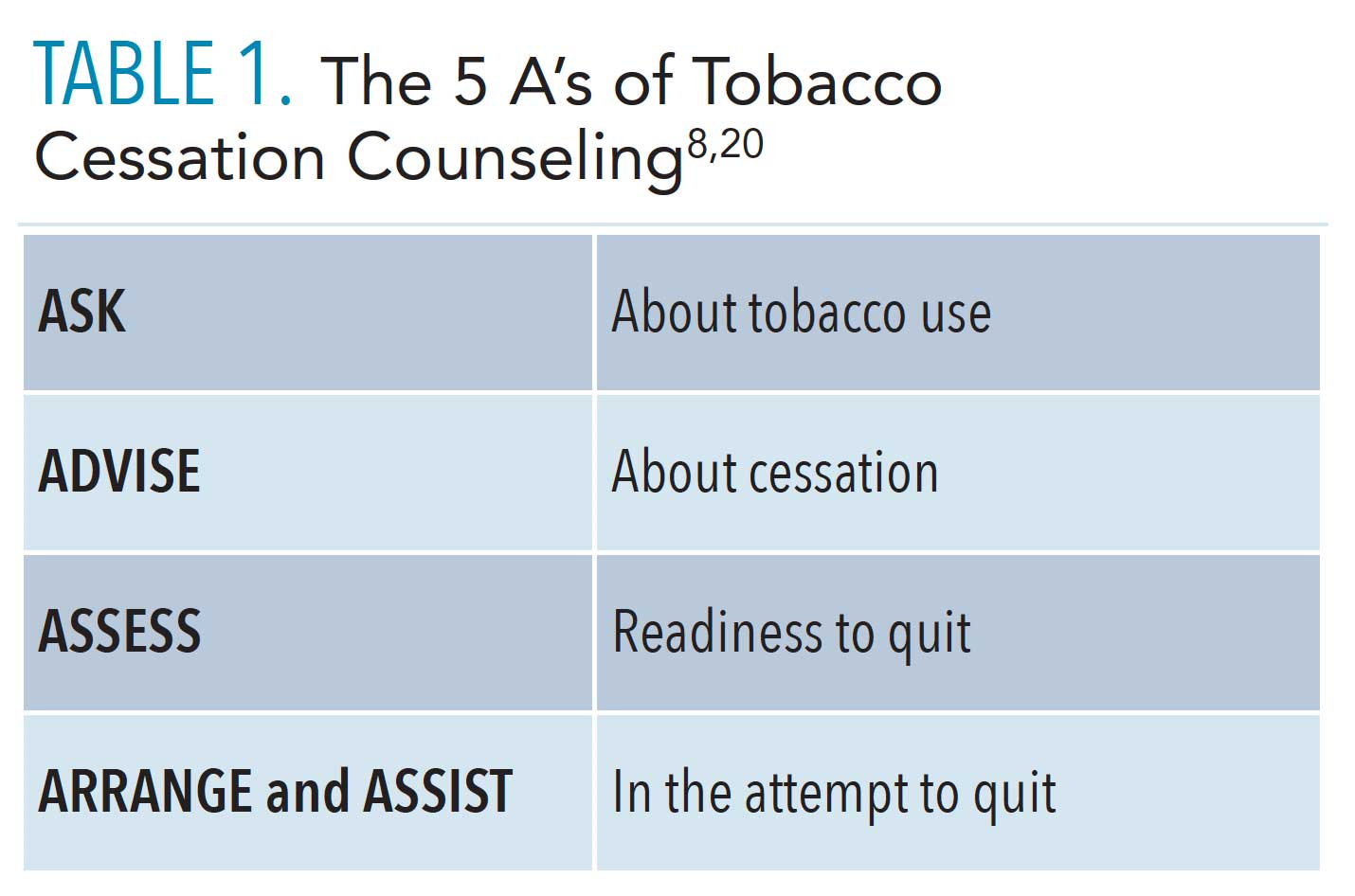
Dental hygienists can use the 5 A’s of tobacco cessation to help patients quit (Table 1, page 37).8,20 Even if only employed for a few minutes, the 5 A’ can increase the likelihood of long-term cessation.
In December 2018, the US Surgeon General Jerome Adams, MD, MPH, issued an advisory on youth e-cigarette use, sounding the alarm that vaping among American children was skyrocketing, and highlighting the need to prevent nicotine dependence among the nation’s young people.32 In response, the US-based nonprofit organization dedicated to eradicating tobacco use, Truth Initiative, added an e-cigarette quit program.14 Personalized for teens and young adults, the “This Is Quitting” program is a free, digital program designed to help users quit vaping.14 It can be accessed by teens and young adults by texting “DITCHJUUL” to 88709. Parents and adults who would like to help young people quit can text “QUIT” to (202) 899-7550. Youth trying to quit vaping will receive supportive messages tailored to their age and e-cigarette use. Participants who are not yet ready to quit receive messages supporting their ability to quit in the future for 4 weeks.
In 2018, the American Dental Hygienists’ Association (ADHA) partnered with the US Centers for Disease Control and Prevention (CDC) to promote the first federal national tobacco education campaign—Tips From Former Smokers. The campaign features real people who are living with serious long-term health effects from smoking in addition to family members who have been impacted by their loved one’s illnesses.33 In its first year, the program motivated 1.64 million people to try to quit smoking. The Tips From Former Smokers campaign offers multiple resources to help oral health professionals assist their patients in tobacco cessation (Table 2).34
Conclusion
Oral health professionals should be aware of the potential cariogenicity of e-cigarettes and prepared to educate ENDS users about this elevated caries risk, in addition to other health risks associated with ENDS use. Using updated CAMBRA approaches to develop an individualized plan combining chemical therapy and conservative restorative treatment to reduce caries risk or arrest caries lesions is integral to an overall approach to support oral health.4 Additionally, dental hygienists play a key role in tobacco cessation. As such, they should be ready to support patients who are interested in quitting e-cigarette use.
References
- Pitts NB, Zero DT, Marsh PD, et al. Dental caries. Nat Rev Dis Primers. 2017;3:17030.
- Kim SA, Smith S, Beauchamp C, et al. Cariogenic potential of sweet flavors in electronic-cigarette liquids. Plos One. 2018;13:e0203717–e0203717.
- Huang R, Li M, Gregory RL. Effect of nicotine on growth and metabolism of Streptococcus mutans. Eur J Oral Sci. 2012;120:319–325.
- California Dental Association Foundation. CAMBRA Caries Management by Risk Assessment: a Comprehensive Caries Management Guide for Dental Professionals. Available at: cdafoundation.org/Portals/0/pdfs/cambra_handbook.pdf. Accessed November 23, 2020.
- Ghazali AF, Ismail AF, Daud A. Caries experience among cigarette and e-cigarette users: a 6-month prospective study. J Pharm Sci. 2019;11:4.
- Savant S, Shetty D, Phansopkar S, Jamkhande A. Electronic cigarettes: ambiguity and controversies of usage. J Coll Physicians Surg Pak. 2014;24:3.
- Chaffee BW. Electronic cigarettes: trends, health effects and advising patients amid uncertainty. J Calif Dent Assoc. 2019;47:85–92.
- Grana R, Benowitz N, Glantz SA. E-Cigarettes: a scientific review. Circulation. 2014;129:1972–1986.
- Cuadra GA, Smith MT, Nelson JM, Loh EK, Palazzolo DL. A comparison of flavorless electronic cigarette-generated aerosol and conventional cigarette smoke on the survival and growth of common oral commensal Streptococci. Int J Environ Res Public Health. 2019;16:1669.
- United States Food and Drug Administration. Vaporizers, E-Cigarettes, and other Electronic Nicotine Delivery Systems (ENDS). Available at: fda.gov/tobacco-products/products-ingredients-components/vaporizers-e-cigarettes-and-other-electronic-nicotine-delivery-systems-ends. Accessed November 23, 2020.
- Stratton KR, Kwan LY, Eaton DL, National Academies of Sciences, Engineering, and Medicine, eds. Public Health Consequences of E-Cigarettes. Washington, DC: National Academies Press; 2018.
- Kim JJ, Sabatelli N, Tutak W, et al. Universal electronic-cigarette test: physiochemical characterization of reference e-liquid. Tob Induced Dis. 2017;15:14.
- Ghazali AF, Ismali AF, Faisal G, Muhamad Halil MH, Daud A. Oral health of smokers and e-cigarette users: a case-control study. Available at: researchgate.net/publication/328006246_Oral_Health_of_Smokers_and_E-Cigarette_Users_A_Case-Control_Study. Accessed November 23, 2020.
- Truth Initiative. Quitting E-Cigarettes. Truth Initiative. Available at: truthinitiative.org/research-resources/quitting-smoking-vaping/quitting-e-cigarettes. Accessed November 23, 2020.
- Goniewicz ML, Knysak J, Gawron M, et al. Levels of selected carcinogens and toxicants in vapour from electronic cigarettes. Tob Control. 2014;23:133–139.
- Javelle E. Electronic cigarette and vaping should be discouraged during the new coronavirus SARS-CoV-2 pandemic. Arch Toxicol. 2020;94:2261–2262.
- Ebersole J, Samburova V, Son Y, et al. Harmful chemicals emitted from electronic cigarettes and potential deleterious effects in the oral cavity. Tob Induc Dis. 2020;18:41.
- Tierney PA, Karpinski CD, Brown JE, Luo W, Pankow JF. Flavour chemicals in electronic cigarette fluids. Tob Control. 2016;25:e10—e15.
- United States Food and Drug Administration. FDA Finalizes Enforcement Policy on Unauthorized Flavored Cartridge-Based E-Cigarettes That Appeal to Children, Including Fruit And Mint. Available at: fda.gov/news-events/press-announcements/fda-finalizes-enforcement-policy-unauthorized-flavored-cartridge-based-e-cigarettes-appeal-children. Accessed November 23, 2020.
- Singh T. Tobacco use among middle and high school students—United States, 2011–2015. MMWR Morb Mortal Wkly Rep. 2016;65:361–367.
- Beshay YS, Gregory RL. The role of nicotine in caries risk and development. Dimensions of Dental Hygiene. 2017;15(7):22–26.
- Ojima M, Hanioka T, Shimada K, Haresaku S, Yamamoto M, Tanaka K. The role of tobacco use on dental care and oral disease severity within community dental clinics in Japan. Tob Induc Dis. 2013;11:13.
- Aguilar-zinser V, Irigoyen ME, Rivera G, Maupomé G, Sánchez-pérez L, Velázquez C. Cigarette smoking and dental caries among professional truck drivers in Mexico. Caries Res. 2008;42:255–262.
- Kubica P, Wasik A, Kot-Wasik A, Namieśnik J. An evaluation of sucrose as a possible contaminant in e-liquids for electronic cigarettes by hydrophilic interaction liquid chromatography–tandem mass spectrometry. Anal Bioanal Chem. 2014;406:3013–3018.
- Kubica P, Wasik A, Kot-Wasik A, Namieśnik J. An evaluation of sucrose as a possible contaminant in e-liquids for electronic cigarettes by hydrophilic interaction liquid chromatography–tandem mass spectrometry. Anal Bioanal Chem. 2014;406:3013–3018.
- Tedjo C, Neoh KG, Kang ET, Fang N, Chan V. Bacteria–surface interaction in the presence of proteins and surface attached poly(ethylene glycol) methacrylate chains. J Biomed Mater Res A. 2007;82:479–491.
- Su N, Marek CL, Ching V, Grushka M, Abom D. Caries prevention for patients with dry mouth. J Can Dent Assoc. 2011;77:b85.
- King JL, Reboussin BA, Wiseman KD, et al. Adverse symptoms users attribute to e-cigarettes: results from a national survey of US adults. Drug Alcohol Depend. 2019;196:9–13.
- Rechmann P, Chaffee BW, Rechmann BMT, Featherstone JDB. Caries management by risk assessment: results from a practice-based research network study. J Calif Dent Assoc. 2019;47:15–24.
- American Academy of Pediatric Dentistry. Caries-risk Assessment and Management for Infants, Children, and Adolescents. Available at: aapd.org/media/Policies_Guidelines/BP_CariesRiskAssessment.pdf. Accessed November 23, 2020.
- American Heart Association. E-Cigarettes and Public Health. Available at: heart.org/idc/groups/heart-public/@wcm/@adv/documents/downloadable/ucm_472463.pdf. Accessed November 23, 2020.
- United States Department of Health & Human Services. Surgeon General releases advisory on E-cigarette epidemic among youth. Available at: hhs.gov/about/news/2018/12/18/surgeon-general-releases-advisory-e-cigarette-epidemic-among-youth.html. Accessed November 23, 2020.
- American Dental Hygienists’ Association. Help Them Stop So They Can Start. Available at; adhaquittobacco.org. Accessed November 23, 2020.
- United States Centers for Disease Control and Prevention. Health Care Providers: How You Can Help Patients Quit. Available at; cdc.gov/tobacco/campaign/tips/partners/health/index.html. Accessed November 23, 2020.
From Dimensions of Dental Hygiene. December 2020;18(11):36-39.
