 SDI PRODUCTIONS/E+/GETTY IMAGES PLUS
SDI PRODUCTIONS/E+/GETTY IMAGES PLUS
What Every Oral Health Professional Needs To Know About the AAP Classification System
The American Academy of Periodontology’s 2017 classification system presents a step forward in the quest for more accurate and timely periodontal assessment, care, and referral.
This course was published in the April 2021 issue and expires April 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the legal and ethical considerations involved in changing the periodontal classification system.
- Differentiate between the 1999 and 2017 periodontal classification guidelines.
- Identify how oral health professionals can integrate the updated periodontal guidelines in their professional practices.
The 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions made significant changes to the periodontal classification system, which has improved diagnostics and treatment. Oral health professionals are responsible for identifying and assisting in the maintenance of patients’ periodontal status. Clinicians should be aware of the changes to the periodontal classification guidelines and be able to apply them in professional practice. Close adherence to the updated guidelines is paramount to legal and ethical practice.
The American Dental Association states that dental providers are responsible for diagnosing and treating disease, infection, deficiency, and any conditions in or around the oral cavity.1 In order to determine the correct periodontal diagnosis, a comprehensive evaluation of the patient’s current oral and overall health is necessary. The American Academy of Periodontology (AAP) suggests that every patient receive an annual comprehensive dental exam, which includes a complete periodontal assessment, including the recording of probing depths, width of keratinized tissue, gingival recession, evaluation of radiographs, and clinical attachment level. Evaluation of bleeding on probing, purulence, furcation involvement, and mobility is necessary to reach an accurate diagnosis. A biofilm index, amount of calculus, and gingival description should be part of the differential diagnosis. Pre-existing systemic conditions and patient risk factors should also be considered.2
Incorrect diagnosis and/or treatment can result in complex legal ramifications. Malpractice is a broad term that encompasses a wide range—from infliction of trauma to neglect. Often, malpractice cases are due to incorrect diagnosis, delay in treatment, and improper management of patient care.3 Oral health professionals must diagnose patients correctly so the appropriate treatment can be rendered. If the diagnosis is wrong, the treatment may also be incorrect.
In the context of oral healthcare, malpractice cases have included improper diagnosis, inadequate treatment, and dental neglect.4 The most common malpractice filing, however, remains failure to diagnose periodontal diseases.3 A variety of consequences result from malpractice suits, including fines, suspension, and/or revocation of licensure. In many of these cases, the plaintiffs were typically long-standing, established patients who were treated without a diagnosis of periodontal disease. Patients with periodontal diseases were seen on a recare interval, but not receiving the proper treatment.4–6 For example, patients with periodontal disease were often treated with prophylaxis instead of nonsurgical periodontal therapy and/or periodontal maintenance therapy.5
Other cases of dental neglect include failure to treat and/or refer the patient to a specialist.4–6 For example, established patients received multiple extractions because the extent of periodontal disease became too advanced but they were not referred by the general practitioner. In many instances, the patient’s pain and suffering could have been avoided if practitioners provided accurate diagnosis and treatment as well as timely referral.5,6 As such, the proceedings from the World Workshop should be at the forefront of every clinician’s mind when diagnosing and treating periodontal diseases.
At the World Workshop, practitioners created the classification guidelines with a systematic process for diagnosing, treating, and referring patients for specialist care when needed. A printable checklist is available on the AAP website to ensure all factors in the annual comprehensive exam are evaluated.2 Adherence to the guidelines may result in improved patient outcomes and reduce clinicians’ risk for malpractice litigation.
Oral health professionals need to understand the etiology of periodontal diseases, benefits of providing valid and reliable therapy, and consequences of not providing appropriate treatment.7 Interprofessional variability in the standard of periodontal care within dental practices may result in undesired outcomes, such as poor periodontal health. Failure to refer in a timely manner can also lead to undesired outcomes.8 The intent of the new periodontal classification guidelines is to provide a more comprehensive approach to diagnosing and managing periodontal status. Evidence suggests that the previous periodontal classification system did not provide enough information for accurate diagnosis and treatment of patients with periodontal diseases.8 The system needed to be updated and adjusted to focus on each patient’s specific condition and overall risk.
DIFFERENCES BETWEEN THE 1999 AND 2017 GUIDELINES
Up until 2017, the periodontal classification guidelines had not been updated since 1999.2,9–12 The 2017 modifications include evaluation of periodontal health and systemic health.2,9,13,14 Clinicians can now classify whether the patient is healthy or has gingivitis or periodontitis, and specifically identify current status of periodontal disease.9,11,12 At the World Workshop, oral health professionals concluded that three forms of periodontitis exist: necrotizing periodontitis, periodontitis as a manifestation of systemic disease, and periodontitis. With the modifications to the classification guidelines, the categories of “chronic” and “aggressive” periodontitis were eliminated.9,10,11,13 While “chronic” and “aggressive” forms of periodontitis are characterized by different presentations of disease, limited clinical evidence demonstrates a practical distinction between them.9,10,13
Periodontal health is the absence of detectable inflammation.12 There are two separate forms of periodontal health: clinical health on an intact periodontium and clinical gingival health on a reduced periodontium. In other words, health of the periodontium can exist before the disease process begins and after the disease has been maintained.15 Prophylactic treatments prevent disease and are appropriate for patients with healthy gingiva and those with gingivitis. When a patient is diagnosed with periodontitis, prophylactic treatment is no longer appropriate. After periodontal diseases are treated with nonsurgical periodontal therapy, the goal is to maintain the patient’s periodontal status. This is achieved by periodontal maintenance therapy. Improper coding of periodontal treatment may lead to insurance fraud litigation. Ensuring the entire dental staff is calibrated to the new periodontal guidelines may safeguard practices against these legal ramifications.
The World Workshop uses a two-factor approach in diagnosing extent of periodontitis.2,7,9,13 The first step is staging, in which clinicians evaluate severity, complexity, and extent/distribution of disease. When evaluating severity, clinicians should assess interdental clinical attachment loss (CAL) at the site of greatest loss, percent of radiographic bone loss (RBL), and quantity of tooth loss due to periodontitis. When evaluating complexity, clinicians should assess probing depths, extent of horizontal and/or vertical bone loss, furcation involvement, ridge defects, and need for complex dental rehabilitation. When evaluating for extent and distribution, clinicians should assess if periodontal diseases present as localized, generalized, or follow a molar/incisor pattern.2,7,9,13
The second step is grading, which indicates the rate of disease progression, responsiveness to therapy, and impact on overall health.10, 11,16 Clinicians should use direct or indirect evidence to determine the progression of disease.10,11,14,16 An example of direct evidence includes evaluating extent of RBL or CAL over 5 years. Clinicians are encouraged to assess a patient’s oral health over time, rather than at one point in time.10,11,16 Clinicians also use indirect evidence to determine extent of disease progression, such as percentage of bone loss based on patient age, and case phenotype, which refers to the extent of biofilm accumulation and periodontal destruction.10,11,14,16 Because there is a normal progression of disease associated with age, the World Workshop’s charts provides a simple calculation to assist clinicians with determining if the rate of progression is within normal limits or not.17 The World Workshop guidelines recommend that clinicians use direct evidence to diagnose disease, wherever possible.10,11,16
A second aspect to the grading component is the notion of grade modifiers, which include systemic risk factors that impact the patient’s periodontal condition.11,14 The World Workshop guidelines recognize that smoking and diabetes impact periodontal health. As such, the classification now acknowledges that the presence and extent of either systemic condition can potentially accelerate the rate of periodontal destruction.11 The systemic risk of periodontal disease, however, is not limited to smoking and diabetes alone.14
The World Workshop also requires that peri-implant health be assessed and considered.2,9,11 None of the previous classification systems discussed implant-related concerns.7 As the popularity of dental implants continues to grow, the number of patients affected by peri-implant diseases is also on the rise.18,19 The gingiva, peri-mucosa, and tissue surrounding an implant are constantly challenged by the oral environment. This includes the constant exposure to biofilm present on adjacent teeth and implant surfaces.18 Implant success depends on thorough examination of the hard and soft tissues to determine if health or disease affects periodontal support.7,11 The tissue surrounding the implant can now be categorized as healthy or having peri-implant mucositis or peri-implantitis.8,9 In order for the peri-implant tissue to be classified as healthy, the tissue must not exhibit any signs of clinical inflammation. Bleeding on probing is a key clinical sign that distinguishes between peri-implant health and disease.18,19 The health of a patient’s implant should be evaluated as it is another sign of oral health. By incorporating implant health into the classification system, clinicians can better document and detect changes in implant health.11
IMPLEMENTATION
The correct adoption of the revised periodontal classification system will require significant recalibration of the workforce, particularly because practitioners have been adhering to the preceding classification for nearly two decades. In 2019, Miyamoto et al20 demonstrated the application of the new system in the case of a 17-year-old woman who presented with slight gingival inflammation. This case integrates the staging and grading system, with emphasis on familial history as a risk factor. Although the patient’s initial diagnosis was gingivitis, when the clinicians looked further into her overall risk, her mother’s history of advanced periodontal disease was included in her evaluation. Familial genetic predisposition to periodontal diseases led to the diagnosis of Periodontitis, Stage I Grade C, which called for early intervention. In this case, efforts to alleviate the potential for rapid disease progression due to the evidence of family history of aggressive periodontitis were implemented. Without this detailed new system, the patient may not have received the proper treatment to maintain her condition and prevent progression. The staging and grading sections of the new classification system add an element of personalization that is integral to the diagnosis and treatment of periodontal diseases.
The prevalence of periodontal diseases is a major public health issue. Periodontal diseases can lead to tooth loss and negatively impact chewing function and esthetics, while also reducing quality of life and adversely affecting systemic health.13 Oral health professionals should use the new classification system to evaluate their patients and to ensure accurate diagnosis and treatment. Treatment should portray a balance between the patient’s chief complaint, diagnosis, goal of therapy, and the treatment plan.7
Currently, there is no cure for periodontal diseases.2 Once a patient is classified as having periodontal disease, he or she will remain in that classification. Patients with periodontal diseases cannot return to periodontal health even with effective treatment, their level of disease can only be maintained.9 However, there is one exception to this rule. If a case is classified as a Stage III due to a vertical periodontal defects and the rest of the interdental CAL throughout the mouth were congruent with Stage II, the problem sites could be regenerated by bone graft treatment. In this case, the patient could be reclassified as Stage II Periodontitis.2
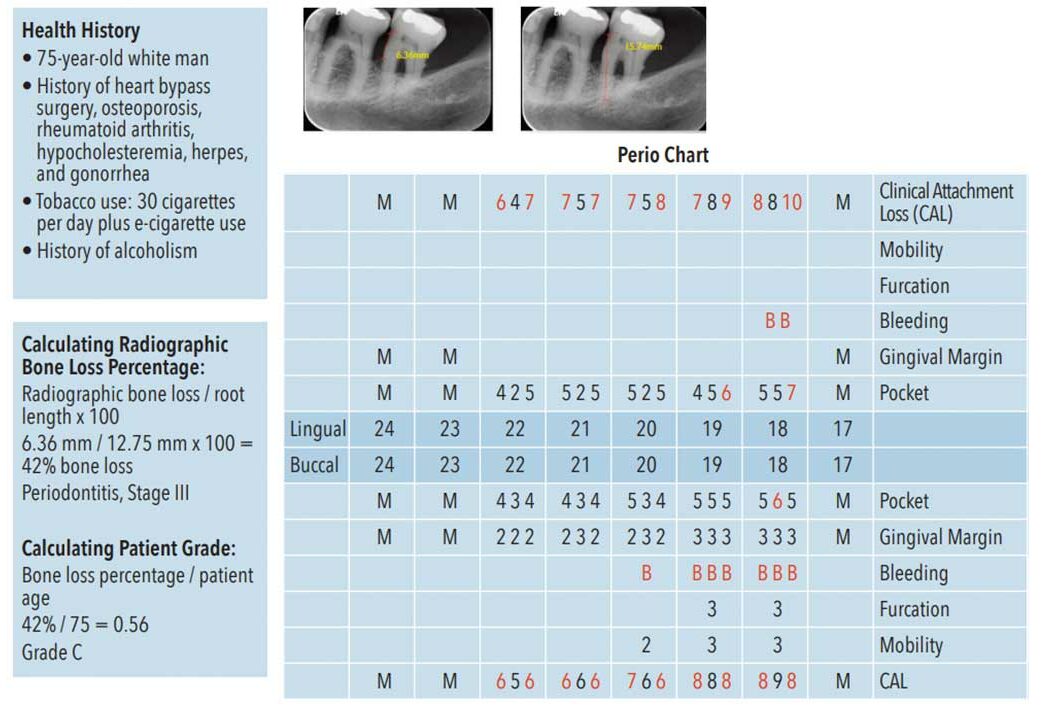
Figure 1 demonstrates how to apply the staging and grading system. The radiographs show how to accurately measure the length of the tooth’s root along with RBL, remembering to begin the measurement 2 mm below the cementoenamel junction. When the amount of RBL is divided by the length of the root and multiplied by 100, this gives the percentage of RBL present. In this instance, approximately 42% RBL exists. Given this percentage, the AAP chart (available at perio.org) can be used to determine this patient’s periodontal condition.
To the determine the grade, previously taken radiographs from at least 5 years ago should be used to compare the percent of RBL to current radiographs. This provides a good indication as to how rapidly the disease is progressing over time. However, if previously taken radiographs are not available, practitioners should use indirect evidence to determine grading. Simply take the percentage of RBL, and divide that number by the patient’s age. For example, the patient in Figure 1 has a RBL percentage of 42%. If that number is divided by his age (75), 0.56 is the result. This number compared to the AAP’s chart (available at perio.org) shows the patient could be classified as Grade B. At this point, practitioners should consider the influence of established grade modifiers. For example, the fact that the patient smokes up to 30 cigarettes a day is a relevant grade modifier in this context. This advances his periodontal grading to Grade C. Thus, the patient’s final periodontal diagnosis should be Periodontitis, Stage III, Grade C.
Application of the World Workshop guidelines is more complex and comprehensive than the previous guidelines, and they remain a work in progress. Changes will continue to be made as the knowledge base surrounding periodontitis expands.10,13
CONCLUSION
The 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions provides the necessary information for clinicians to accurately diagnose, treat, refer, and maintain periodontal diseases in their patients. Improvements to the periodontal classification system will ultimately result in a higher standard of care. When dental offices incorporate the updated guidelines, oral health professionals will be able to closely monitor their patients’ periodontal status. They will be more effective in managing the progression of periodontal disease and referring more complex conditions to specialists. The World Workshop is a strong step forward for more accurate and timely periodontal assessment, care, and referral.
ACKNOWLEDGEMENT
The authors would like to thank Taylor Cornuaud, RDH, BSDH; Regan Gopffarth, RDH, BSDH; and Deborah Foyle, DDS, MS, MSC, for their assistance with this manuscript.
REFERENCES
- American Dental Association. Dentists: Doctors of Oral Health. Available at: ada.org/en/about-the-ada/dentists-doctors-of-oral-health. Accessed March 15, 2021.
- American Academy of Periodontology. Proceedings from the 2017 World Workshop on the Classification of Periodontal and Peri-Available at: perio.org/2017wwdc. Accessed March 15, 2021.
- Vasquez R. 4 prominent things you should know about dental malpractice. Available at: centerforhealthjournalism.org/2016/02/10/4-prominent-things-you-should-know-about-dental-malpractice. Accessed March 16, 2021.
- Misra SR, Mishra L, Kumar M, et al. Dental malpractice, the odds in dental treatment. Indian J Public Health. 2018;9:2430.
- Case: pain from untreated periodontal disease. Clinical Risk. 2007;13(4):159.
- Dental malpractice: elderly female, age not given: failure to diagnose and treat or refer out severe periodontal disease over aperiod of years: loose, shifting teeth: $85,000 settlement. CINAHL Nursing Guide. April 2007.
- Mittal V, Bhullar R, Bansaal R, et al. A Practical approach for periodontal classification. Dent Res J (Isfahan). 2013;10:697–703.
- Sweeting LA, Davis K, Cobb CM. Periodontal Treatment Protocol (PTP) for the general dental practice. J Dent Hyg. 2008;82 Suppl 3:16–26.
- Caton J, Armintage G, Berglundh T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions—introduction and key changes from the 1999 classification. J Clin Periodontol. 2018;45(Suppl 20): S1–S8.
- Tonetti M, Greenwell H, Kornman K. Staging and grading of periodontitis: Framework and proposal of a new classication and case definition. J Clin Periodontol. 2018;89:1475.
- Babay N, Alshehri F, and AlRowis R. Major highlights of the new 2017 classification of periodontal and peri-implant disease and conditions. Saudi Dent J. 2019;3:303–305.
- Chapple I, Mealey B, Van Dyke T, et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri‐Implant Diseases and Conditions. J Clin Periodontol. 2018;47:S68–S77.
- Papapanou P, Sanz M, Buduneli N, et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018;45(S20):S1–S291.
- Albandar J, Susin C, Hughes F. Manifestations of systemic diseases and conditions that affectthe periodontal attachment apparatus: Case definitionsand diagnostic considerations. J Clin Periodontol. 2017;89(Suppl 1):S183–S203.
- Lang N, BartoldM. Peridontal Health. J Clin Periodontol. 2017;89:S1.
- Graetz C, Mann L, Krois J, et al. Comparison of periodontitis patients’ classification in the 2018 versus 1999 classification. J Clin Periodontol. 2019;46:908–917.
- Billings M, Holtfreter B, Papapanou P, et al. Age–dependent distribution of periodontitis in two countries: Findings from NHANES 2009 to 2014 and SHIP‐TREND 2008 to 2012. J Clin Periodontol. 2018;89:S1.
- Araujo M, Lindhe J. Peri-implant health. J Periodontol. 2018;89:S249–S256.
- Jepsen S, Berglundh T, Genco R, et al. Primary prevention of peri-implantitis: managing peri-implant mucositis. J Clin Periodontol. 2015;42:S152–S157.
- Miyamoto T, Kumagai T, Khan S, et al. Application of 2017 new classification of periodontal diseases and conditions to localized aggressive periodontitis: case series. J Clin Periodontol. 2019;9:185–191.
From Dimensions of Dental Hygiene. April 2021;19(4):40–43.
