
Does Periodontal Disease Increase the Risk of Pancreatic Cancer?
A look at the current research.
This course was published in the July 2008 issue and expires July 31, 2011. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Understand the potential relationship between pancreatic cancer and periodontal disease.
- Discuss the lethality of pancreatic cancer and why it is so difficult to diagnose.
- Identify the risk factors for pancreatic cancer.
In January 2007, a group of Harvard investigators published some research suggesting that periodontal disease—as a marker of a susceptible immune system—may indicate an increased risk for pancreatic cancer.1
Investigation of this possible association is in its infancy but preliminarily it appears that periodontal disease and pancreatic cancer may be linked by an underlying mechanism that is inflammatory driven. An understanding of this potential relationship may help dental practitioners to better educate their patients on the potential ramifications of systemic inflammation in the oral cavity relative to diseases of the digestive tract. While many unknowns still exist related to the etiology, diagnosis, and treatment of pancreatic cancer, this challenging disease may be prevented through aggressive changes in behavior and lifestyle. Greater awareness among dental practitioners regarding the various risk factors associated with this lethal type of cancer and preventive measures may provide an additional, albeit nontraditional, opportunity for identifying those at risk for pancreatic cancer.
INFLAMMATION AS THE CULPRIT
In a questionnaire-based study of 51,529 predominately Caucasian male health professionals, Michaud and colleagues,1 reported that periodontal disease was associated with a 64% increase in the risk of pancreatic cancer, after adjusting for smoking and other risk factors. The researchers also found that within this study population, periodontal disease with recent tooth loss was associated with a 2.7-fold increase in the risk of pancreatic cancer. Furthermore, they found that the timing and severity of periodontal disease, as manifested by recent tooth loss, may have a joint effect.
Age, smoking, and obesity did not appear to influence the association between periodontal disease and pancreatic cancer. When men with a history of diabetes were excluded from the analysis, a statistically significant association between periodontal disease and pancreatic cancer was still observed. The investigators suggested that several mechanisms may explain the biological plausibility of the associations observed in this study.
The first hypothesis1 is that periodontal disease may promote pancreatic carcinogenesis through inflammation. The investigators cite earlier reports2,3 that plasma C-reactive protein (CRP) levels—an important biomarker of systemic inflammation—were consistently higher in subjects with a history of periodontal disease than those with no history.
An alternative hypothesis1,4 is that periodontal disease may influence pancreatic carcinogenesis through increased generation of carcinogens, specifically nitrosamines. Nitrosamines are known to induce pancreatic cancer in animals and are considered potential carcinogens in human pancreatic cancer.4,5 Approximately 45% to 75% of nitrosamine formation is endogenously formed by salivary and gastrointestinal bacteria.4,6 The formation of nitrosamines in the oral cavity of individuals with poor oral hygiene is eight times higher than in individuals with good oral hygiene.7 Also, periodontal disease and poor oral hygiene are associated with higher levels of oral bacteria and elevated nitrosamine levels within the oral cavity. As such, this relationship may place certain individuals at greater risk because nitrosamines and gastric acidity may play important roles in pancreatic cancer.
Individuals afflicted with chronic pancreatitis are at greater risk for developing pancreatic adenocarcinoma.7-10 Research published by Wheatley-Price and colleagues10 suggests that inflammation plays a role in the disease etiology of pancreatic cancer through the different forms of several inflammatory pathway genes. The same genotype is associated with an increased risk of coronary artery disease, raising the possibility that inflammatory processes may be important etiologically in pancreatic cancer.10 Accordingly, the chronic, low level inflammation associated with periodontitis may convey a greater risk of pancreatic cancer.10
Stolzenberg-Solomon and colleagues4 examined the association between dentition history and pancreatic cancer on a prospective group of 29,133 Finnish men who smoked. They found that tooth loss was significantly associated with pancreatic cancer and that this trend was consistent across all categories of tooth loss. The researchers also reported that compared with those with less tooth loss, the edentulous subjects were more likely to have ulcers, which is linked to Helicobacter pylori infection.
 Stolzenberg-Solomon and colleagues4 discussed several mechanisms that may explain the increased risk associated with tooth loss and pancreatic cancer, including the contribution of poor oral hygiene to more deleterious gastrointestinal flora, and consequently, increased nitrosation. Another theory raised by these researchers is that tooth loss may be an indicator of a less healthy lifestyle or of health status in general. For instance, tooth loss reduces masticatory ability11-12 thereby leading to consuming a less healthy diet.11,13-14 Edentulous individuals in the study had greater intake of total and saturated fat and diminished intake of folate, both dietary factors that are associated with a greater risk of pancreatic cancer.4,15 The analysis of the data controlled for these dietary factors and the factors did not modify the association that Stolzenberg-Solomon and colleagues found between tooth loss and pancreatic cancer.
Stolzenberg-Solomon and colleagues4 discussed several mechanisms that may explain the increased risk associated with tooth loss and pancreatic cancer, including the contribution of poor oral hygiene to more deleterious gastrointestinal flora, and consequently, increased nitrosation. Another theory raised by these researchers is that tooth loss may be an indicator of a less healthy lifestyle or of health status in general. For instance, tooth loss reduces masticatory ability11-12 thereby leading to consuming a less healthy diet.11,13-14 Edentulous individuals in the study had greater intake of total and saturated fat and diminished intake of folate, both dietary factors that are associated with a greater risk of pancreatic cancer.4,15 The analysis of the data controlled for these dietary factors and the factors did not modify the association that Stolzenberg-Solomon and colleagues found between tooth loss and pancreatic cancer.
THE LETHALITY
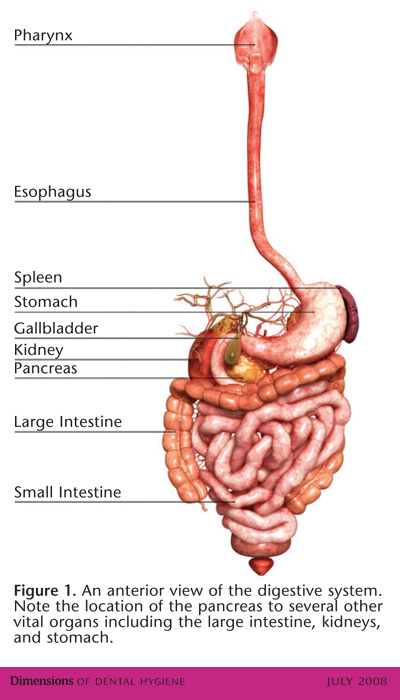
Pancreatic cancer is the fourth leading cause (after lung, breast, and colo-rectum8) of cancer death in the United States,1 (approximately 30,000 new cases are diagnosed each year), and it ranks eighth in incidence in the world.4 Pancreatic cancer is a relatively uncommon malignancy.4 However, the mortality rate is very high and its lethality near universal,16 mostly due to the location of the pancreas, which makes it very difficult to access, and its proximity to other vital organs.17 Figure 1 illustrates the placement of the pancreas in the body. The overall 5-year survival rate is less than 4%.18 One of the reasons the survival rate is so low is that pancreatic cancer is difficult to diagnose at an early, resectable stage and less than 15% of cases are candidates for surgery.19 The current lack of a screening technique to accurately and cost-effectively detect pancreatic cancer in the general population before the onset of symptoms also impacts the ability to intervene in the early stages of the disease.16
In the United States, the incidence of pancreatic cancer is 40% higher in men than women.8 Predominately a disease of older people, only about 13% of all patients are diagnosed with pancreatic cancer before 60.8 Nearly 50% of patients are 75 years or older at the time of diagnosis.8 As longevity increases, the incidence of pancreatic cancer will become more frequent; a measurable age-related increase in the global burden of pancreatic cancer is expected as the number of people aged 65 and older increases throughout the world.8
RISK FACTORS
Risk factors related to pancreatic cancer are classified as demographic, host-related, or environmental.16,20 With 80% of pancreatic cancer occurring between the ages of 60 and 80,21 the most important demographic factor is advancing age. Jewish descent, black ethnicity, and male gender are associated with a slight (less than two-fold) increased risk.21
Cigarette smoking is the most significant and reproducible environmental risk factor for pancreatic cancer,1,16,20 accounting for 25%-30% of all cases.8 Exposure to tobacco products conveys about a two-fold increased risk for pancreatic cancer, compared to nonsmokers.8,16,20 Some studies have found a dose response relationship between smoking and increased risk, with heavy smoking having a substantially higher risk of pancreatic cancer than light smoking.8,22,23 In countries where smoking has increased, for example in Japan from the 1950s to the 1990s, the frequency of pancreatic cancer increased.8 In populations where smoking rates decreased, such as in the American male population, the incidence of pancreatic cancer is declining.8 In estimating the impact of complete smoking cessation on the frequency of pancreatic cancer in the European Union, Mulder and colleagues24 determined that the incidence of pancreatic cancer could be reduced by 15%. Aggressive public health measures to control smoking may substantially reduce the incidence of pancreatic cancer.8
Candidates for referral to medical care providers for further evaluation for the risk of pancreatic cancer include patients between ages 60-80 and
- History of pancreatic cancer in first or second-degree relatives
- Chronic pancreatitis
- Smoking
- Diabetes of recent onset
- Obesity
- Insulin resistance
- Diet high in calories and in fat content from red and processed meats
- BMI >25 kg/m2 and sedentary life style
- Male gender
- Black ethnicity
- Jewish descent
- Helicobacter pylori infection
- Cystic fibrosis
- History of any cancer in a first-degree relative
- Colo-rectal cancer
- Gallstone disease
- Peptic ulcer disease
Mounting evidence suggests that diabetes, obesity, and insulin resistance are also associated with risk for pancreatic cancer.1,16,25-27 Diet may also play a role. Fat content, which contributes to total caloric intake, seems to be the dietary factor most consistently associated with pancreatic cancer.8,28-30 The intake of total and saturated fat from red and processed meat, but not dairy products, appears to increase the risk for pancreatic cancer.31 Increased consumption of fruits and vegetables reduces the risk of pancreatic cancer.28,29,32 Exercise, to help maintain healthy weight, is also associated with decreased risk for pancreatic cancer.30 However, not all studies agree with these findings.
Meta-analyses25,33 of the association between diabetes and pancreatic cancer suggest that individuals with diabetes have about a two-fold increased risk of pancreatic cancer. A significant amount of data suggests that diabetes may be a marker for pancreatic cancer (or a complication of pancreatic cancer) in some individuals, and a predisposing risk factor in others.34 In a large case-control study of pancreatic cancer in San Francisco, Wang and colleagues34 found that recent-onset diabetes (but not diabetes of 10 years and longer) may be a complication or an early marker of pancreatic cancer. Further, the investigators reported that people who had diabetes for a shorter time and used insulin may have a substantially elevated risk for pancreatic cancer, which could mean that insulin resistance is elicited by pancreatic cancer.
Pre-existing chronic pancreatitis is associated with a 10- to 20-fold increased risk of pancreatic cancer.8,9,16 A cohort study35 of more than 2,000 patients from six different countries found a 14-fold increased risk for pancreatic cancer of patients with chronic pancreatitis after a follow-up period of 5 years. Alcohol is a major risk factor for chronic pancreatitis, however, it is not known whether its use plays a role as a risk factor in pancreatic cancer.36
The greatest risk factor for the development of pancreatic cancer is genetic predisposition.16 Individuals with the highest risk have multiple family members who have been diagnosed with pancreatic cancer.16 Approximately 10% of individuals with pancreatic cancer have more than one first-degree or second-degree relatives with pancreatic cancer.16,37
For patients with an early onset of pancreatic cancer, a positive family history for pancreatic cancer or a genetic defect is often present.35,38 Some studies evaluating the risk for pancreatic cancer in families with known genetic mutations have reported risks ranging from 13- to 39-fold.37,39,40 Other gene mutations (polymorphisms) have protective properties such as the potential to detoxify tobacco or food-related carcinogens.8 This may explain why individuals who are exposed to known risk factors do not develop pancreatic cancer.8 Individuals with hereditary pancreatitis have a 30%-40% higher cumulative risk for pancreatic cancer.8 Within this high risk group, individuals who smoke tend to develop pancreatic cancer about 10 years earlier than nonsmokers.
Other digestive tract diseases, including gallstone disease41,42 and peptic ulcer disease,43,44 may be pre-existing diseases that increase the risk for pancreatic cancer. Cystic fibrosis is associated with a moderately increased risk of pancreatic cancer.16,45 Infection of Helicobacter pylori may convey a modest increased risk for pancreatic cancer.4,46
The interaction of various risk factors for pancreatic cancer is important to consider. The cumulative risk imposed by multiple risk factors in a cohort with an already high baseline risk of developing pancreatic cancer is more significant than any individual risk factor within the general population in which the incidence of pancreatic cancer is relatively low. For example, smoking in patients with hereditary pancreatitis increases the risk for pancreatic cancer by 54- to 154-fold.47 The inter-relationship between obesity and physical activity appears to affect the risk for pancreatic cancer. Based on two large cohort studies,48 the highest risk for developing pancreatic cancer may be associated with higher body mass index (?25 kg/m2) and low total physical activity; greater physical activity appears to decrease the risk of pancreatic cancer in overweight individuals.
TARGETING THOSE AT RISK
The survival rate of pancreatic cancer many be enhanced if the disease can be diagnosed in its earlier stages;34 a substantial body of data suggests that the detection of the very early stages of the disease allows for a better prognosis.16 As a result, the search for effective early detection tools has taken on a new urgency.34
Experts at a 2002 conference49 concluded that screening patients with a history of hereditary pancreatitis at age 40 and older is helpful in better identifying those who are at high risk of pancreatic cancer.
According to another consensus opinion,16 pancreatic cancer screening for those at high risk is recommended. For individuals in these high risk pools, diagnostic tools such as endoscopic ultrasound and endoscopic retrograde cholangiopancreatography may offer hope in earlier identification of at risk patients,16 as well as genetic testing and counseling to educate high risk patients.16
To date, the benefit of chemoradiotherapy in treating pancreatic cancer has been limited.50 However, a number of emerging molecular therapies, still under development, hold promise in effective treatment, including gene therapy, antiangiogenic agents, immunotherapy, and inhibitors of cell signaling.34 Chemoprevention, with drugs such as COX inhibitors8,51 and aspirin52,53 have shown some promise in reducing the risk of pancreatic cancer.
PRACTICAL APPLICATIONS
Because there is no agent proven to prevent pancreatic cancer, risk factor reduction lies at the heart of preventive strategies.16 This includes the ability of health care providers to identify individuals at high risk for pancreatic cancer, in addition to recognizing modifiable risk factors and strategies aimed at their elimination.34
Identify patients at risk for pancreatic cancer who should then be referred to medical care providers for further evaluation. More than a dozen germline mutations increase the risk of pancreatic cancer.8 Identifying patients with a strong familial history of pancreatic cancer may provide for earlier interventions.8 Evidence also suggests that certain individuals with diabetes, especially new onset diabetes, may be at higher risk for pancreatic cancer.34 Another population at risk for pancreatic cancer are individuals aged 60-80 who have other risk factors such as smoking, history of chronic pancreatitis, other digestive tract diseases, obesity, and high fat consumption. Targeted surveillance of people in these risk pools could help in the identification of early-stage, resectable pancreatic cancer and the potential for improved survival rate.
Help patients eliminate or modify risk for pancreatic cancer. Pancreatic cancer ‘should be emerging as a form of cancer that might be preventable, at least in part through modification of lifestyle habits’.6 Recommendations for these kinds of lifestyle modifications for patients include the following:
- Smoking cessation, especially for individuals with a familial history of pancreatic cancer, is critical. For patients with chronic pancreatitis or a familial history of pancreatic cancer, provide referral services for smoking cessation.
- Evaluate patients’ diets. Counsel patients on the importance of a diet with adequate quantities of fruits and vegetables, low in fat from red and processed meats, and other dietary measures aimed at calorie reduction that may help to prevent pancreatic cancer.8
- Evaluate patients’ intake of vitamin D. Intakes of vitamin D higher than 600 IU are associated with a lower risk of pancreatic cancer.54
- Counsel overweight patients (BMI ?25 kg/m2) that greater physical activity appears to decrease the risk of pancreatic cancer and the other health benefits of regular exercise and weight control.55
- For patients who are at greater risk for any form of cancer, discuss current research related to how inflammation, in response to certain trigger factors such as infection from oral origin, may influence cancer growth.
REFERENCES
- Michaud DS, Joshipura K, Giovannucci E, Fuchs CS. A prospective study of periodontal disease and pancreatic cancer in US male health professionals. J Natl Cancer Inst. 2007;99:171-175.
- Loos BG. Systemic markers of inflammation in periodontitis. J Periodontol. 2005;76(Suppl):2106-2115.
- Joshipura KJ, Wand HC, Merchant AT, Rimm EB. Periodontal disease and biomarkers related to cardiovascular disease. J Dent Res. 2004;83:151-155.
- Stolzenberg-Soloman RZ, Blaser MJ, Limburg PJ, et al. Helicobacter pylori seropositivity as a risk factor for pancreatic cancer. J Natl Cancer Inst. 2001;93:937-941.
- Hujoel PP, Drangsholt M, Spiekerman C, Weiss NS. An exploration of the periodontitis-cancer association. Ann Epidemiol. 2003;13:312-316.
- Ziebarth D, Spiegelhalder B, Bartsch H. N-nitrosation of medicinal drugs catalysed by bacteria from human saliva and gatstrointestinal tract, including Helicobacter pylori. Carcinogenesis. 1997;18:383-389.
- Nair J, Ohshima H, Nair UJ, Bartsch H. Endogeneous formation of nitrosamines and oxidative DNA-damaging agents in tobacco users. Crit Rev Toxicol. 1996;26:149-161.
- Lowenfels AB, Maisonneuve P. Epidemeology and prevention of pancreatic cancer. Jpn J Clin Oncol. 2004;34:238-244.
- Malka D, Hammel P, Maire F, et al. Risk of pancreatic adenocarcinoma in chronic pancreatitis. Gut. 2002;51: 849-852.
- Wheatley-Price P, Asomaning K, Reid A, et al. Myeloperoxidae and superoxide dismutase polymorphisms are associated with an increased risk of developing pancreatic adenocarcinoma. Cancer. 2008;112:1037-1042.
- Wayler AH, Chauncey HH. Impact of complete dentures and impaired natural dentition on masticatory performance and food choice in healthy aging men. J Prosthet Dent. 1983;49:427-433.
- Chauncey HH, Muench ME, Kapur KK, Wayler AH. The effect of the loss of teeth on diet and nutrition. Int Dent J. 1984;34:98-104.
- Papas AS, Joshi A, Giunta JL, Palmer CA. Relationship among education, dentate status, and diet in adults. Spec Care Dentist. 1998;18:26-32.
- Papas AS, Palmer CA, Rounds MC, Russell RM. The effects of denture status on nutrition. Spec Care Dentist. 1998;18:17-25.
- Stolzenberg-Solomon RZ, Albanes D, Nieto FJ, et al. Pancreatic cancer and nutrition-related methyl-group availability indicators in male smokers. J Natl Cancer Inst. 1999;91:535-541.
- Brand RE, Lerch MM, Rubinstein WS, et al. Advances in counselling and surveilance of patients at risk for pancreatic cancer. Gut. 2007;56:1460-1469.
- Gapstur SM, Gann P. Is pancreatic cancer a prevetable disease? JAMA. 2001;286:967-968.
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006;56:106-130.
- Niederhuber JE, Brennan MF, Menck HR.. The national cancer data base report on pancreatic cancer. Cancer. 1995;76:1671-1677.
- Gold EB, Goldin SB. Epidemeology of and risk factors for pancreatic cancer. Surg Oncol Clin N Am. 1998;7:67-91.
- Lillemoe KD, Yeo CJ, Cameron JL. Pancreatic cancer: state-of-the-art care. CA Cancer J Clin. 2000;50:241-268.
- Lin Y, Tamakoshi A, Kawamura T, et al. A prospective chort study of cigarette smoking and pancreatic cancer in Japan. Cancer Causes Control. 2002;13:249-254.
- Akiba S, Hirayama T. Cigarette smoking and cancer motality risk in Japanese mean and women-results from reanalysis of the six-prefecture cohort study data. Environ Health Perspect. 1990;87:19-26.
- Mulder I, Hoogenveen RT, van Genugten ML, et al. Smoking cessation would substantially reduce the future incidence of pancreatic cancer in the European Union. Eur J Gastroenterol Hepatol. 2002;14:1343-1353.
- Everhart J, Wright D. Diabetes mellitus as a risk factor for pancreatic cancer. A meta-analysis. JAMA. 1995;273:1605-1609.
- Stolzenberg-Solomon RZ, Graubard BI, Chari S, et al. Insulin, glucose, insulin resistance, and pancreatic cancer in male smokers. JAMA. 2005;294:2872-2878.
- Rapp K, Schroeder J, Klenk J, et al. Obesity and the incidence of cancer: a large cohort study of over 145,000 adults in Austria. Br J Cancer. 2005;93:1062-1067.
- Baghurst PA, McMichael AJ, Slavotinek AH, Baghurst KI, Boyle P, Walker AM. A case-control study of diet and cancer of the pancreas. Am J Epidemiol. 1991;134:167-179.
- Ghadirian P, Thouez JP, PetitClerc C. International comparisons of nutrition and mortality from pancreatic cancer. Cancer Detect Prev. 1991;15:357-362.
- Stolzenberg-Solomon RZ, Pietinen P, Taylor PR, Virtamo J, Albanes D. Prospective study of diet and pancreatic cancer in male smokers. Am J Epidemiol. 2002;155: 783-792.
- Nöthlings U, Wilkens LR, Murphy SP, Hankin JH, Henderson BE, Kolonel LN. Meat and fat intake as risk factors for pancreatic cancer: the multiethnic cohort study. J Natl Cancer Inst. 2005;97:1458-1465.
- Zatonski W, Przewozniak K, Howe GR, Maisonneuve P, Walker AM, Boyle P. Nutritional factors and pancreatic cancer: a case control study from south-west Poland. Int J Cancer 1991;48:390-394.
- Huxley R, Ansary-Moghaddam A, Berrington de González A, Barzi F, Woodward M. Type II diabetes and pancreatic cancer: a meta-analysis of 36 studies. Br J Cancer. 2005;92:2076-2083.
- Wang F, Gupta S, Holly EA. Diabetes mellitus and pancreatic cancer in a population-based case-control study in the San Francisco Bay area, California. Cancer Epidemiol Biomarkers Prev. 2006;15:1458-1463.
- Lowenfels AB, Maisonneuve P, Cavallini G, et al. Pancreatitis and the risk of pancreatic cancer. International Pancreatitis Study Group. N Engl J Med. 1993;328:1433-1437.
- Klein AP, Brune KA, Petersen GM, et al. Prospective risk of pancreatic cancer in familial pancreatic cancer kindreds. Cancer Res. 2004;64:2634-2638.
- Brand RW, Lynch HT. Hereditary pancreatic adenocarcinoma: a clinical perspective. In: Whitcomb DC, Cohn JA, Ulrich CD, eds. The Medical Clinics of North America: Inherited Diseases of the Pancreas. Philadelphia: W.B. Saunders Co; 2000:665-675.
- Lowenfels AB, Maisonneuve P, DiMagno EP, et al. Hereditary pancreatitis and the risk of pancreatic cancer. International Hereditary Pancreatitis Study Group. J Natl Cancer Inst. 1997;89:442-446.
- Vasen HF, Gruis NA, Frants RR, van Der Velden PA, Hille ET, Bergman W. Risk of developing panceatic cancer in families with familial atypical multiple mole melanoma associated with a specific 19 deletion of p16(p16-Leiden). Int J Cancer. 2000;87:809-811.
- Borg A, Sandberg T, Nilsson K, et al. High frequency of multiple melanomas and breast and pancreas carcinomas in CDKN2A mutation-positive melanoma families. J Natl Cancer Inst. 2000;92:1260-1266.
- Chow WH, Johansen C, Gridley G, Mellemkjaer L, Olsen JH, Fraumeni JF Jr. Gallstones, cholecystectomy and risk of cancers of the liver, biliary tract and pancreas. Br J Cancer. 1999;79:640-644.
- Coughlin SS, Calle EE, Patel AV, Thun MJ. Predictors of pancreatic cancer mortality among a large cohort of United States adults. Cancer Causes Control. 2000;11: 915-923.
- Silverman DT, Schiffman M, Everhart J, et al. Diabetes mellitus, other medical conditions and familial history of cancer as risk factors for pancreatic cancer. Br J Cancer. 1999;80:1830-1837.
- Tascilar M, van Rees BP, Sturm PD, et al. Pancreatic cancer after remote peptic ulcer surgery. J Clin Pathol. 2002;55:340-345.
- Maisonneuve P, FitzSimmons SC, Neglia JP, Campbell PW 3rd, Lowenfels AB. Cancer risk in nontransplanted and transplanted cystic fibrosis patients: a 10- year study. J Natl Cancer Inst. 2003;95:381-387.
- Stolzenberg-Solomon RZ, Dodd KW, Blaser MJ, Virtamo J, Taylor PR, Albanes D. Tooth loss, pancreatic cancer, and Helicobacter pylori. Am J Clin Nutr. 2003;78: 176-181.
- Lowenfels AB, Maisonneuve P, Whitcomb DC, Lerch MM, DiMagno EP. Cigarette smoking as a risk factor for pancreatic cancer in patients with hereditary pancreatitis. JAMA. 2001;286:169-70.
- Giovannucci E, Michaud DS, Willet WC et al. Physical activity, obesity, height, and the risk of pancreatic cancer. JAMA. 2001;286:921-929.
- Durie P, Lerch MM, Lowenfels AB, et al. Genetic Disorders of the Exocrine Pancreas. An Overview and Update. Basel: Karger; 2002.
- Tsai JY, Iannitti DA, Safran H. Combined modality therapy for pancreatic cancer. Semin Oncol. 2003;30:71-79.
- Kokawa A, Kondo H, Gotda T, et al. Increased expression of cyclooxygenase-2 in human pancreatic neoplasms and potential for chemoprevention by cyclooxygenase inhibitors.” Cancer. 2001;91:333-338.
- Lowenfels AB, Maisonneuve P, Lankisch PG. Chronic pancreatitis and other risk factors for pancreatic cancer. Gastroenterol Clin North Am. 1999;28:673-685.
- Anderson KE, Johnson TW, Lazovich D, Folsom AR. Association between nonsteroidal anti-inflammatory drug use and he incidence of pancreatic cancer. J Natl Cancer Inst. 2002;94:1168-1171.
- Skinner HG, Michaud DS, Giovannucci E, et al. “Vitamin D intake and the risk for pancreatic cancer in two cohort studies.” Cancer Epidemiol Biomarkers Prev. 2006;15:1688-1695.
- Kelly P. Focus on oncology. The cancer critical care paradox.” Curr Anaesth Crit Care. 2008;19:96-104.
From Dimensions of Dental Hygiene. July;6(7): 32-35.
