Update on Anesthesia
Gwen Essex, RDH, MS, EdD, discusses pain control options for the dental hygienist.
Q. When are topical anesthetics most effective in the provision of pain relief?
A. It depends on which topical is used. Most topical anesthetics used to numb the tissue before local injection offer up to 4 mm of penetration of the mucosal tissue within 2 minutes to 3 minutes. However, the use of topical anesthetics is not effective on keratinized tissue, such as the palate, unless the topical is left on for 3 minutes to 5 minutes. For palatal use, pressure anesthesia— the creation of ischemia in the tissues through the application of pressure in the area receiving the injection for 1 minute to 2 minutes—is most effective in reducing patient discomfort.
In terms of topical anesthetics for injections, the most commonly used are the benzocaines, which are esters. Some patients may experience an allergic reaction when given esters systemically, but there is little systemic absorption of these compounds in the mouth. Generally, the only signs of sensitivity are minor, such as microbleeding at the site of application. Benzocaines are most commonly used because they have a 2 minute to 3 minute window of efficacy whereas amides take 10 minutes to 15 minutes to become effective. Thus, amides are not traditionally used as topical agents.
Unfortunately, not all dental hygienists can administer a local anesthetic injection. Additionally, in some states hygienists are allowed to administer infiltrations but not blocks. Regardless of the rationale of regulations, dental hygienists must work within the limits of the governing laws and regulations.
In areas where dental hygienists are prohibited from giving local anesthetic injections, there is a tendency to overapply topical anesthetic if a patient has gingival sensitivity. This is not the best-recommended practice because there is a risk of overdose when using topical anesthetics and alternative needle-free options are available. One option is Oraqix®*, a lidocaine/ prilocaine combination.
Oraqix is a 5% solution of 2.5% lidocaine and 2.5% prilocaine. It begins working within 30 seconds with the most profound anesthesia occurring within 5 minutes and lasting approximately 20 minutes. Oraqix is applied into the gingival crevice or periodontal pocket and can provide significant pain relief during scaling and root planing.1
Q. Do you have any tips for success in using topical anesthetics?
A. I find that drying the gingiva with gauze before applying a topical anesthetic helps me more accurately see where I am applying it. Anecdotally, I believe that dry tissue is better able to accept whatever I’m placing on it, so I typically blot the tissue dry with cotton gauze before placement.
Q. Are there any other topical anesthetic solutions for dental hygienists who cannot give injections?
A I have had great success with dyclonine hydrochloride or Dyclone**.2 Dyclone is a liquid 5% solution that takes 10 minutes to become effective. However, when I place it on the tongue, it works much more quickly, most likely because of the placebo effect of the patient feeling his or her tongue go numb. I add Dyclone to a bit of mouthrinse, have the patient rinse for 30 seconds to a minute, and spit it out. I’ve found that patients with generalized gingival sensitivity respond very well to this. Dyclone was unavailable for a period of time due to a manufacturing problem but is now back on the market. Although it was commercially unavailable temporarily, many dentists continued using it because compounding pharmacies were able to create it for them.
A combination topical anesthetic designed to provide long-lasting topical anesthesia is available in Cetacaine®***. A combination of 14% benzocaine, a quickonset, short-acting topical; 2% butamben, an intermediate-onset, intermediateacting drug; and 2% tetracaine hydrochloride, a slow-onset and longlasting topical, Cetacaine is designed to offer a potentially more extensive topical effect.3 In liquid form Cetacaine can also be applied subgingivally with a blunt tip needle.
If dental hygienists can’t have a syringe in their armamentarium due to dental practice acts, I would definitely recommend they have these other options available. We shouldn’t be scaling patients who are in pain so it’s important to use all available tools to ensure that we’re offering adequate pain relief.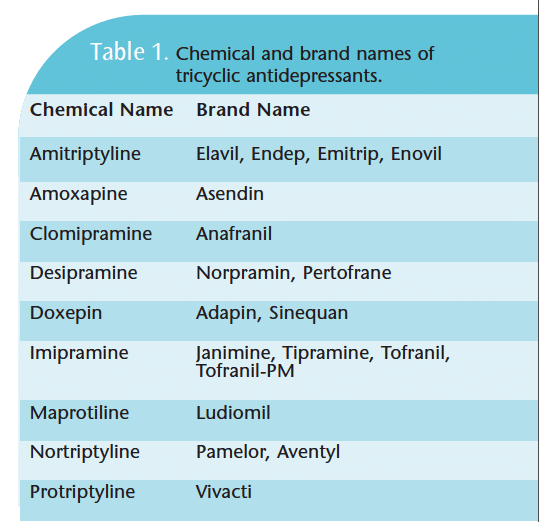
LOCAL ANESTHETICS
Q. Please review the guidelines re garding blood pressure and vasoconstrictors.
A. I believe that it’s always best to include a vasoconstrictor if it can be done safely. Clinicians need to remember that if a patient has a pain reaction, his or her own adrenaline response will be much greater than any reaction from the epinephrine.
Clinicians will often automatically rule out a vasoconstrictor if a patient checks hypertension on his or her medical history. I strongly believe that clinicians need to take patients’ blood pressure before every injection because even if they checked hypertensive on the medical history form, they may not be hypertensive today. If they are hypertensive but it’s under control, then they’re not actually hypertensive during the appointment. Rather than just looking at the medical history and making a decision about which anesthetic to use, clinicians should review a patient’s vital signs taken the day of the appointment and then make a decision. Stress should not be placed on the heart unnecessarily but treating a patient who is in pain is not a positive outcome either and can be potentially dangerous.
A larger issue relating to safety is that clinicians need to be very conscientious about their aspiration technique. They need to aspirate in multiple planes when they are in areas where there are a lot of vessels, such as the posterior superior alveolar or inferior alveolar. Aspiration in multiple planes helps ensure that tissue isn’t blocking the bevel of the needle, which will give a false negative aspiration result. By being conscious of aspiration and taking blood pressure the day of treatment, a vasoconstrictor can be included more frequently. Vasoconstrictors provide a reduction in overall dose and an increase in the amount of time that the drug is absorbed. It’s more slowly metabolized so the addition of a vasoconstrictor reduces the risk for overdose. Vasoconstrictors also provide longer lasting and more profound anesthesia.
Vasoconstrictors should not be included when patients have diastolic pressure above 100. If a patient has that high of a reading and is not being treated for hypertension, he or she needs a referral to a physician for assessment. Local anesthetics without vasoconstrictors are potent vasodilators so there will be more bleeding at the site. Other contraindications for vasoconstrictor use are uncontrolled hypertension, hyperthyroidism (vasoconstrictors can potentiate the problems of hyperthyroid), uncontrolled angina, and recent heart attacks.
 There are two categories of drugs that warrant care when using vasoconstrictors: tricyclic antidepressants and nonselective beta blockers (see Tables 1 and 2 for a list of chemical and brand names). In a patient taking a tricyclic antidepressant, the vasoconstrictor use should be reduced to 1:100,000. An excellent choice is prilocaine, which includes a vasoconstrictor at 1:200,000—effectively reducing the normal dose by half. Mepivacaine, which is used without a vasoconstrictor but does some vasoconstriction of its own, is another option. Also prilocaine used as a block with no vasoconstrictor is just as effective as 2% lidocaine in terms of working time and profound anesthesia because of its affinity for lipids. So if prilocaine is given at a nerve trunk where there are a lot of lipids, an effective block occurs but if used as an infiltration without a vasoconstrictor, it’s only going to last 20 minutes. Typically with patients taking tricyclic antidepressants, delivering more than two or three carpules is contraindicated; the amount administered should not be more than 1:100,000.
There are two categories of drugs that warrant care when using vasoconstrictors: tricyclic antidepressants and nonselective beta blockers (see Tables 1 and 2 for a list of chemical and brand names). In a patient taking a tricyclic antidepressant, the vasoconstrictor use should be reduced to 1:100,000. An excellent choice is prilocaine, which includes a vasoconstrictor at 1:200,000—effectively reducing the normal dose by half. Mepivacaine, which is used without a vasoconstrictor but does some vasoconstriction of its own, is another option. Also prilocaine used as a block with no vasoconstrictor is just as effective as 2% lidocaine in terms of working time and profound anesthesia because of its affinity for lipids. So if prilocaine is given at a nerve trunk where there are a lot of lipids, an effective block occurs but if used as an infiltration without a vasoconstrictor, it’s only going to last 20 minutes. Typically with patients taking tricyclic antidepressants, delivering more than two or three carpules is contraindicated; the amount administered should not be more than 1:100,000.
Clinicians must have a good drug reference on hand. Most medical emergencies in the dental office can be avoided by looking up a drug, taking a new vital sign, and not just reflexively using 2% lidocaine for every patient. Often clinicians continue to administer 2% lidocaine if a block fails. Dental hygienists need to believe in their technique, recognizing that patients may or may not be receptive to a particular drug. If an injection has been given and the dental hygienist feels that it was successful but the patient has no response, a new drug should be administered. I think that many dental hygienists feel that anesthesia failure is a technique failure on their part. Some patients may not react to a drug the way that most patients do. A better result may be gained by using a drug with a different molecular structure.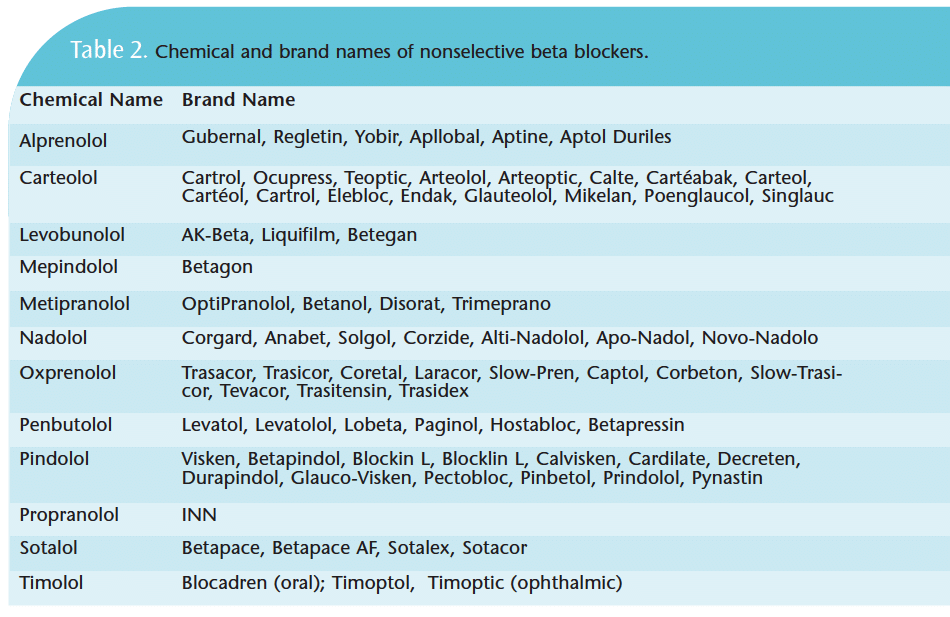
Dental hygienists are very concerned about patient safety and comfort. What I love about the dental hygiene community is that we’re very holistic in the treatment of our patients. I don’t know many hygienists who ask their patients to just “grin and bear it.” Providing comfortable local anesthesia is possible and dental hygienists should not to be afraid to administer it if it’s in their license category. There are just a few techniques to becoming proficient in the delivery of anesthesia: use a topical, leaving it on for 1 minute to 2 minutes on dry tissue, and inject slowly (60 seconds to 120 seconds for one cartridge). If you’re restricted by your state’s dental practice act, then the use of other topical anesthetic agents can help significantly.
The views expressed in this interview are the author’s.
REFERENCES
- DiMatteo A. Efficacy of an intrapocket anesthetic for scaling and root planing procedures: a review of three multicenter studies. Compend Contin Educ Dent. 2005;26(2 Suppl 1):6-10.
- Roghani S, Duperon DF, Barcohana N. Evaluating the efficacy of commonly used topical anesthetics. Pediatr Dent. 1999;21:197-200.
- Bassett K, DiMarco AC. Safety first. Dimensions of Dental Hygiene. 2007;5(10): 20-25.
From Dimensions of Dental Hygiene. October 2009; 7(10): 24-26, 28, 30.

{kind=link}