The Heart of the Matter
To better understand the association between cardiovascular disease and oral health and its effect on the provision of dental care, Dimensions of Dental Hygiene spoke to renowned heart surgeon and innovator in the field of endovascular surgery Jacob DeLaRosa, MD, and risk assessment expert JoAnn R. Gurenlian, RDH, PhD
Q When dental hygienists are treating patients with heart problems, what do they need to be aware of?
DeLaRosa: Dental professionals need to know if a patient has valvular heart disease. When these patients receive oral health care, dental hygienists need to “stop, prophylac, and then act.” Valvular heart disease patients must receive antibiotics before dental treatment because bacteria in the gingiva can enter the bloodstream, infecting the heart valve and causing endocarditis.1
Q What separates valvular disease from the greater umbrella of cardiovascular disease?
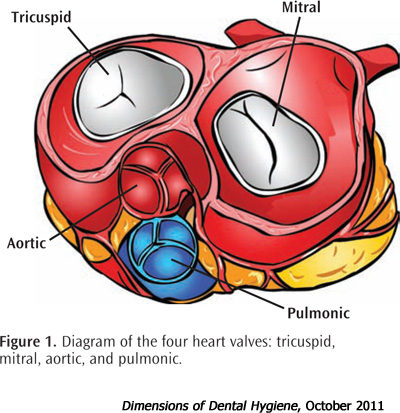
DeLaRosa: Valvular heart disease is characterized by a defect in one of the four heart valves: tricuspid, mitral, aortic, and pulmonic (Figure 1). Most people with valvular disease have lesions on the left side in the aortic valve or the mitral valve. It’s important to ask patients if they have heart disease and, if so, which type. There are many kinds of cardiovascular problems, but valvular disease is the most important in regards to dental treatment (see sidebar).2
Q Do dental hygienists need to be concerned about heart patients experiencing acute episodes of cardiac distress?
DeLaRosa: I have not had this experience in my practice. Patients with heart disease can have a heart attack while they are walking down the street. I don’t think an episode is any more likely to occur while they are in the dental chair.
Q Are there symptoms that dental hygienists should watch for that would indicate treatment should be postponed?
DeLaRosa: If a patient becomes short of breath during a procedure, then there is a problem. People with heart disease should not experience shortness of breath during routine dental procedures. Increased anxiety is also a potentially dangerous symptom.
Q What can dental hygienists do specifically to screen their patients for possible signs of cardiovascular problems?

Gurenlian: Functional capacity is a way to measure cardiac risk that focuses on a patient’s ability to complete various physical activities. Functional capacity is defined as the ability to perform activities that meet a four metabolic level of endurance or metabolic equivalents (METs). METs include: eating and dressing, walking around the house, light housework, and climbing a flight of stairs (Table 1).5,6
This assessment can help determine cardiac risk and the need for further cardiovascular evaluation. Dental hygienists can ask patients questions related to METs, such as:
- Can you climb a flight of stairs with groceries?
- Can you walk on level ground at 4 mph or run a short distance?
- Can you perform heavy housework, such as scrubbing and vacuuming floors?
- Can you perform recreational activities, such as golfing, bowling, playing tennis, dancing, throwing a softball or football, etc?
If the patient answers “yes” to these questions, he or she meets the minimum four METs level of endurance and is at low risk of cardiac emergency during the scheduled dental hygiene appointment. If the patient reports, however, that he or she cannot walk up a flight of stairs or perform light housework—such as dusting or washing dishes—without shortness of breath, fatigue, or chest pain, the patient is at increased risk of cardiac problems.
As preventive specialists, dental hygienists have an opportunity to use this cardiac risk assessment to possibly prevent a medical emergency, as well as determine whether a patient requires further medical evaluation and intervention with a cardiologist (see Case Study).
Q Are there instances when you would advise against patients with cardiovascular disease receiving dental care?
DeLaRosa: No, but I strongly encourage patients to make their dental care providers aware of their disease. I often ask patients to have their dental care provider call me before treatment, and I am happy to report that I receive many calls from dental hygienists and dentists about effectively and safely treating patients with heart disease.
Q Are you familiar with the science showing an association between cardiovascular disease and periodontal diseases?
DeLaRosa: Data show that people with poor oral health are more likely to have heart disease, and there are many theories about why this is true.3,4 The hypothesis that seems most likely is that patients who don’t take care of their teeth also do not take care of their heart.
Q As more research is conducted on this relationship, would the assertion of a more direct relationship change the way you treat your patients?

DeLaRosa: Every patient I see who needs open heart surgery for a valve replacement must have his or her teeth professionally cared for. This is mandatory. Patients are often surprised that I am looking in their mouth when they came in to have their heart problems treated. I explain that their heart health and overall health are dependent on maintaining a healthy dentition. I ask all of my patients if they receive regular dental care. If not, I ask them to take care of this first before beginning cardiac treatment. Before I initiate invasive treatment on patients, I want to make sure they do not have an abscess, active infection, or extremely poor oral health—because an infection in the oral cavity can enter the bloodstream and eventually attack the lining of the new heart valve. I have my patients’ dental providers fax me a report, so I am aware of their oral health status.
Gurenlian: Unfortunately, dental hygienists are all too familiar with patients and health care providers who do not recognize that the mouth is connected to the body. Many patients don’t know why we ask medical questions as part of the health history. This is the perfect moment to discuss health practices, and how improved oral health translates to better general or overall health.
There are several changes I would like to see in oral health care. First, I would ensure that cardiac risk assessment was part of every dental practice. Second, I would encourage practices to create a plan for managing cardiac-related medical emergencies, including hypotension; severe hypertension; arrhythmias; and episodes of congestive heart failure, myocardial infarction, and stroke. While many dental practices have not experienced medical emergencies, I personally have seen three patients present with signs of active myocardial infarction in the past few years. For each case, treatment was deferred, 911 was used, and the patients were transported to a local hospital for further cardiovascular care. Staff members were prepared to administer CPR if needed. Fortunately, each person survived and was able to resume regular oral health care appointments without further incident. However, there is no substitute for knowing how to manage these types of medical emergencies. Regular practice of medical emergency situations helped us remain calm and effective.
I would also consider altering the appointment schedule for patients with a significant cardiac history. They may not be able to tolerate long appointments, recline in a supine position, or manage the physical stress of dental and dental hygiene appointments. Customizing the appointment experience to address these issues is helpful for both patients and practitioners. Assessing the patient’s oral health and providing education that is both relevant and practical for the patient’s needs. Some patients simply do not relate a chronic inflammatory periodontal condition to their general health. Helping these individuals realize that long-standing compromised oral health is not in their best interest, and that it can be significantly improved by working together, is as important as removing calculus and stain.
QDo you foresee greater collaboration between dentistry and medicine?
DeLaRosa: I would like to see it. I hope that dental professionals encourage patients with inadequate oral health who do not list cardiovascular disease on their health histories to get a heart check-up. People who have been smokers should also be referred for cardiac evaluation. As a heart surgeon, the earlier I see patients, the better their prognoses.
The dental office often provides the first opportunity for health screening. People will visit a dental office before they will schedule a medical check-up. If we can get those at risk of cardiovascular disease to see a physician through a referral from the dental office, we can greatly improve patient outcomes. Heart disease is the number one killer in the United States. Early referral and treatment can improve this statistic. There aren’t enough family practice physicians to serve as gatekeepers for the health of all Americans. Dental hygienists and dentists can fill this gatekeeping role by referring at-risk patients for care. This could be a significant transition in how medicine is practiced in this country.
Gurenlian: I see opportunities for dental hygienists and dentists to broaden their vision of health care and to partner with other clinicians to improve the health of the public. In addition to cardiovascular disease, cancer is a leading causes of death in the US. Diabetes is a worldwide epidemic. All of these conditions have oral health implications. We cannot work in a vacuum with “open wide” as our starting point. We can create target goals for our practice settings that include addressing these health concerns for our patients.
A graduate student in the Department of Dental Hygiene at Idaho State University is working on a program with a state oral health coalition to bring physicians and oral health professionals together to address the issue of greater collaboration. With health care reform on the horizon, and ever increasing concerns about access to quality oral health care, we have wonderful opportunities to embrace and utilize the best of each discipline’s expertise.
 A 78-year-old woman arrived for her biannual dental appointment. She appeared short of breath while walking from the reception area to the operatory. Further questioning revealed that this patient had been experiencing chest tightness and shortness of breath while walking around her home and performing simple household chores. The patient reported that bringing groceries from the car into her home was problematic. Her vital signs were within normal limits, but the chest tightness and shortness of breath were red flags. She was referred for a cardiac evaluation, and the patient underwent an electrocardiogram and stress test.
A 78-year-old woman arrived for her biannual dental appointment. She appeared short of breath while walking from the reception area to the operatory. Further questioning revealed that this patient had been experiencing chest tightness and shortness of breath while walking around her home and performing simple household chores. The patient reported that bringing groceries from the car into her home was problematic. Her vital signs were within normal limits, but the chest tightness and shortness of breath were red flags. She was referred for a cardiac evaluation, and the patient underwent an electrocardiogram and stress test.
The cardiologist sent a follow-up letter to the practice indicating that the results of testing were within normal limits; however, the patient was somewhat overweight and had been self-limiting with physical activities. The patient was advised to lose a modest amount of weight and begin a suitable home-exercise program.
When the patient returned for additional oral health care several months later, she had been exercising more regularly, was able to walk 20 minutes per day without difficulty, and had lost 7 pounds. She was pleased to report that her shortness of breath and chest tightness appeared to be resolving. This intervention in the dental office led to a positive outcome for the patient and the avoidance of a possible crisis during dental treatment.
Case Study
A 78-year-old woman arrived for her biannual dental appointment. She appeared short of breath while walking from the reception area to the operatory. Further questioning revealed that this patient had been experiencing chest tightness and shortness of breath while walking around her home and performing simple household chores. The patient reported that bringing groceries from the car into her home was problematic. Her vital signs were within normal limits, but the chest tightness and shortness of breath were red flags. She was referred for a cardiac evaluation, and the patient underwent an electrocardiogram and stress test.
The cardiologist sent a follow-up letter to the practice indicating that the results of testing were within normal limits; however, the patient was somewhat overweight and had been self-limiting with physical activities. The patient was advised to lose a modest amount of weight and begin a suitable home-exercise program.
When the patient returned for additional oral health care several months later, she had been exercising more regularly, was able to walk 20 minutes per day without difficulty, and had lost 7 pounds. She was pleased to report that her shortness of breath and chest tightness appeared to be resolving. This intervention in the dental office led to a positive outcome for the patient and the avoidance of a possible crisis during dental treatment.
The views expressed in this interview are those of Jacob DeLaRosa, MD, and JoAnn R. Gurenlian, RDH, PhD.
REFERENCES
- Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care andOutcomes Research Interdisciplinary Working Group. J Am Dent Assoc. 2008;139(Suppl):3S–24S.
- Mackay J, Menash GA. The Atlas of Heart Disease and Stroke. Geneva, Switzerland: World Health Organization; 2004:19.
- Beck J, Garcia R, Heiss G, Vokonas PS, Offenbacher S. Periodontal disease and cardiovascular disease. J Periodontol. 1996;67(10 Suppl):1123–1137.
- Beck JD, Offenbacher S, Williams R, Gibbs P, Garcia R. Periodontitis: a risk factor for coronary heart disease? Ann Periodontol. 1998;3:127–141.
- Ainsworth BE, Haskell WL, Leon AS, et al. Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc. 1993;25:71–80.
- Ainsworth BE, Haskell WL, Whitt MC, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32(9 Suppl):S498–S504.
From Dimensions of Dental Hygiene. October 2011; 9(10): 36-38, 40.

{kind=link}