Lasers in Orthodontics
As diode lasers become more common in orthodontic practice, dental hygienists need to understand their many uses.
Diode lasers are a new addition to the armamentarium of practicing orthodontists. Dental hygienists will most likely encounter patients with either completed or proposed laser treatment, and they may need to monitor procedural results and discuss laser therapies with patients.
The term laser is an acronym for light amplification by the stimulated emission of radiation. Laser light produced by a diode laser has a wavelength of 810 nanometers (nm) to 980 nm, which is at the high end of the infrared light portion of the electromagnetic radiation spectrum. This particular wavelength is not visible to the human eye, but it can be damaging to the retina; operators, assistants, and patients must always wear wavelength-specific safety glasses (provided by laser unit manufacturers) during use. The target molecules of this wavelength are melanin and hemoglobin, which are prevalent in gingival tissues, especially in inflamed tissue.
Laser light is monochromatic (on the same wavelength), unlike ordinary visible light, which possesses varying wavelengths—from red (650 nm) to violet (400 nm). It is also monophasic, meaning the wavelengths of light are all coincident (occurring simultaneously), and collimated, that is, travel in a straight line (Figure 1).1

Because the target molecules of the diode laser wavelengths are melanin and hemoglobin, both healthy and inflamed gingival and mucosal tissue can be cut. The cutting action is achieved by heating these molecules, which causes them to explode on a microscopic level. Table 1 lists the advantages of this technology in comparison to cutting tissue with a scalpel.2 Diode lasers will not interact with the dentition or metal, making them safe for use around restorations and orthodontic appliances.
Anesthesia
The use of diode lasers during orthodontic procedures requires some level of anesthesia. Depending on the scope and duration of a procedure, topical anesthetics, needleless anesthesia systems, and infiltration with a nonepinephrine-bearing local anesthetic can be used. Epinephrine is contraindicated because it restricts blood flow, and thus reduces the amount of hemoglobin in the target tissue, making the tissue more difficult to cut. Nerve blocks are not necessary for any orthodontic procedures.
Common Procedures
Diode laser units used in orthodontics are small and compact; some are the size of hand-held curing lights. The laser light is produced within the unit and delivered to the cutting tip via a fiber-optic cable. The tip itself is similar to a thick monofilament fishing line surrounded by a metal canula, and the metal portion of the tip can be curved with the fingers to assist in directing the laser light into difficult-to-access areas of the mouth. Diode laser tips are usually 300 microns or 400 microns in diameter.3
 Gingival recontouring/gingivoplasty/gingivectomy. Gingival surgery is often necessary in conjunction with orthodontic treatment. At the conclusion of orthodontic therapy, inflammation and hypertrophy of the gingival tissues are common due to lack of oral hygiene, space closure, and movement of teeth over a long distance. Diode lasers can surgically alter/remove tissues to address these problems, as well as provide esthetic gingival contouring prior to restoring individual teeth with composite, porcelain veneers, or full-coverage crowns.4
Gingival recontouring/gingivoplasty/gingivectomy. Gingival surgery is often necessary in conjunction with orthodontic treatment. At the conclusion of orthodontic therapy, inflammation and hypertrophy of the gingival tissues are common due to lack of oral hygiene, space closure, and movement of teeth over a long distance. Diode lasers can surgically alter/remove tissues to address these problems, as well as provide esthetic gingival contouring prior to restoring individual teeth with composite, porcelain veneers, or full-coverage crowns.4
Care must be taken not to impinge on the biologic width of the attached gingiva, or gingival recession may occur. Figure 2A through Figure 2C show a patient who presented with tissue encroaching on the archwire and was treated with a gingivoplasty/gingivectomy during orthodontic treatment.
Canine exposure. Permanent canines may be impacted in the hard and soft tissues or only in the soft tissue. Often canines can be exposed through a diode laser procedure, and an attachment can be bonded to the tooth to facilitate eruption (Figure 3A–Figure 3C). Especially on facially positioned teeth, soft tissue anatomy must be taken into consideration prior to performing a surgical exposure.5
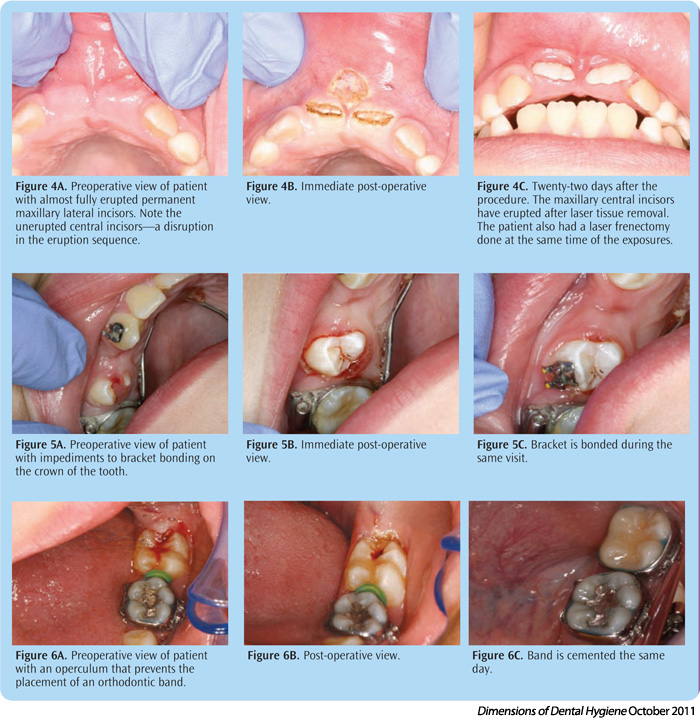
Exposure to facilitate eruption of teeth other than canines. In the event of the premature loss of primary teeth due to trauma or caries, the eruption of the succedaneous teeth may be delayed due to the hyperkeratinization of the tissue in the extraction or avulsion site. Laser incision into the tissue can expedite the eruption of the permanent teeth because the tissue becomes less problematic after laser uncovering (Figure 4A–Figure 4C).6,7
Tissue removal for proper orthodontic bracket placement. It is often difficult, especially in newly erupted teeth among early adolescent patients, to position an orthodontic bracket in the proper position on the crown of a tooth. Excessive tissue, sulcular fluid leakage, or hemorrhage can all impede the bonding of brackets. With diode lasers, tissue can be removed to facilitate bracket placement (Figure 5A–Figure 5C). Due to its ability to coagulate hemorrhage, the bracket can often be bonded to the tooth immediately after tissue removal.8
Operculectomy. The presence of an operculum, especially over the disto-occlusal surface of a mandibular second molar, can impede or prevent the placement of an orthodontic band. Taking into consideration the soft tissue anatomy of the area, the operculum can be removed using a laser so a band can be immediately placed (Figure 6A–Figure 6C). This situation often requires infiltration with a local anesthetic due to the thickness of the tissue.9
 Frenectomy. Diode lasers can be used for both lingual and labial frenectomies. Often the maxillary labial frenum is a factor in both the presence of a midline diastema and its re-opening after orthodontic treatment is completed and retention is discontinued. The typical protocol is to close the midline space with appliances, eliminate occlusal factors that may contribute to the spacing, perform a labial frenectomy, and hold the space closed with appliances for at least 6 weeks to 8 weeks after the frenectomy is completed. Traditional frenectomy is performed with an incision by a scalpel, the tissue is removed, and the wound is sutured. With the diode laser, a horizontal incision across the frenum is performed, fibrous tissue is removed, and the tissue is ablated—all without the need for suturing (Figure 7A–Figure 7E). The patient is instructed to move the upper lip several times a day to keep the opposing sides of the wound from healing together. As uncomfortable as the wound may appear, very little discomfort is experienced by the patient.1
Frenectomy. Diode lasers can be used for both lingual and labial frenectomies. Often the maxillary labial frenum is a factor in both the presence of a midline diastema and its re-opening after orthodontic treatment is completed and retention is discontinued. The typical protocol is to close the midline space with appliances, eliminate occlusal factors that may contribute to the spacing, perform a labial frenectomy, and hold the space closed with appliances for at least 6 weeks to 8 weeks after the frenectomy is completed. Traditional frenectomy is performed with an incision by a scalpel, the tissue is removed, and the wound is sutured. With the diode laser, a horizontal incision across the frenum is performed, fibrous tissue is removed, and the tissue is ablated—all without the need for suturing (Figure 7A–Figure 7E). The patient is instructed to move the upper lip several times a day to keep the opposing sides of the wound from healing together. As uncomfortable as the wound may appear, very little discomfort is experienced by the patient.1
Wound Healing
One of the most appealing aspects of using diode lasers for minor surgical procedures is that inflammation is drastically reduced, and healing usually occurs quickly and without complication.10 Cellular damage adjacent to a laser-induced surgical wound is minimal and usually leads to a comfortable post-operative recovery for the patient. Many patients report they do not need over-the-counter pain medications while others use analgesics for less than 2 days. The presence of pain is relative to the extent of the procedure performed and the patient’s tolerance level. Periodontal dressings are not necessary, the patient is not packed with gauze, and sutures are not used to close the wounds, which further reduces inflammation.
More than 150 procedures have been performed with the diode laser in the dental school clinic at the University of Colorado Denver, School of Dental Medicine. Only one complication has occurred that required an immediate post-operative visit. In this case, the patient disturbed the surgical site with his fingernail several hours after the surgery, hemorrhage occurred, and a liver clot formed. It was removed via suction, the source of the bleeding was identified, and the wound was cauterized with the laser, using only a topical anesthetic.
Summary
The use of diode lasers in dentistry is relatively new and their efficacy in a variety of applications is still being investigated.11 Their effectiveness in soft tissue procedures, however, is well documented and diode lasers offer significant benefits, including: improved overall oral health, expedited orthodontic treatment, and improved outcomes. Dental hygienists will likely encounter orthodontic patients who have undergone soft tissue procedures and should be knowledgeable about their indications.
REFERENCES
- Kravitz ND, Kusnoto B. Soft-tissue lasers in orthodontics: an overview. Am J Orthod Dentofacial Orthop. 2008;133:110–114.
- Christensen G. Soft-tissue cutting with laser vs. electrosurgery. J Am Dent Assoc. 2008;139:981–984.
- Hilgers JJ, Tracey SG. Clinical uses of diode lasers in orthodontics. J Clin Orthod. 2004;38:266–273.
- Gracco A, Tracey S, Lombardo L, Siciliani G. Soft tissue laser in orthodontics. Prog Orthod. 2011;12:66–72.
- Genovese MD, Olivi G. Use of laser technology in orthodontics: hard and soft tissue laser treatments. Eur J Paediatr Dent. 2010;11:44–48.
- Sarver DM, Yanosky M. Principles of cosmetic dentistry in orthodontics: Part 3. Laser treatments for tooth eruption and soft tissue problems. Am J Orthod Dentofacial Orthop. 2005;127:262–264.
- Sousa MV, Scanavini MA, Sannomiya EK, Velasco LG, Angelieri F. Influence of low-level laser on the speed of orthodontic movement. Photomed Laser Surg. 2011;29:191–196.
- Jarjoura K. Soft tissue lasers. Am J Orthod Dentofacial Orthop. 2005;127:527–528.
- Pick RM, Colvard MD. Current status of lasers in soft tissue dental surgery. J Periodontol. 1993;64:589–602.
- Ozcelik O, Cenk Haytac M, Kunin A, Seydaoglu G. Improved wound healing by low-level laser irradiation after gingivectomy operations: a controlled clinical pilot study. J Clin Periodontol. 2008;35:250–254.
- Cobb CM. Lasers in periodontics: a review of the literature. J Periodontol. 2006;77:545–564.
From Dimensions of Dental Hygiene. October 2011; 9(10): 30-32, 34.

{kind=link}