Sweetness Without Sugar
Effectively counseling patients about low/noncalorie sweeteners.
This course was published in the July 2010 issue and expires July 2013. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the five Food and Drug Administration approved low/noncalorie sweeteners.
- Discuss the five “generally recognized as safe” low/noncalorie sweeteners.
- Understand why oral health care workers need to be knowledgeable about these sweeteners and how they may help patients.
Untreated dental caries exists in 16% to 42% of Americans and disproportionately affects individuals within the lower socioeconomic strata.1 In addition, the prevalence of overweight children and adults is becoming an epidemic.2,3 The importance of diet choices in the development of caries and as a contributor to weight gain is well-established.4-7 The caries process is multifactorial in nature but dietary sugars are a significant contributor to the disease.8 The retention of fermentable carbohydrates and frequency of exposure to the teeth are important considerations when evaluating the cariogenicity of food products.9 Fermentable carbohydrates include sugars or prepared starches that are used in acid production by the oral microflora.10-14 Consumption in developed countries is reported to be 40 kg to 60 kg/person/year.15 Sucrose, fructose, and maltose are commonly used sugars in beverages and processed food products. They each produce about 4 calories per gram. Natural and artificial alternatives to these carbohydrates are available as low/noncaloric sweeteners.
There are currently only five Food and Drug Administration (FDA) low/noncaloric sweeteners approved as additives. However, there are other low/noncaloric sweeteners that have FDA “generally recognized as safe” (GRAS) designation. In order to best counsel their patients, oral health care workers need to be knowledgeable about these agents.
THE IDEAL REPLACEMENT
Recognizing sucrose’s cariogenic potential and caloric burden, industry and researchers have searched for alternative sweeteners. The ideal product would provide sweetness but have no unpleasant after-taste, contain few or no calories, be noncarcinogenic or mutagenic, be economical to produce, and would not be heat degradable. The identification of such products has been challenging. Numerous non- nutritive sweetening agents that are not metabolized and contain little or no caloric value have been developed and marketed in the United States but none have possessed all of the ideal properties.
FDA-APPROVED SWEETENERS AS ADDITIVES
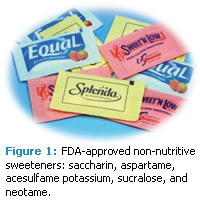 The FDA can approve or recognize a food substance by one of two means. To be approved by the FDA as a “food additive” submitted data are evaluated and the substance is determined to be safe under the conditions of proposed use. For approval under GRAS, a substance must be reviewed and accepted widely by qualified experts that the substance is safe under the conditions of its intended use. Currently there are five FDA-approved non-nutritive sweeteners as food additives: saccharin, aspartame, acesulfame potassium, sucralose, and neotame (Figure 1).
The FDA can approve or recognize a food substance by one of two means. To be approved by the FDA as a “food additive” submitted data are evaluated and the substance is determined to be safe under the conditions of proposed use. For approval under GRAS, a substance must be reviewed and accepted widely by qualified experts that the substance is safe under the conditions of its intended use. Currently there are five FDA-approved non-nutritive sweeteners as food additives: saccharin, aspartame, acesulfame potassium, sucralose, and neotame (Figure 1).
SACCHARIN
Saccharin, discovered in 1878, is 300 times as sweet as sucrose and is the oldest of the artificial sweeteners. It is noncariogenic; noncaloric; and is available in liquid, tablet, and powder form as a tabletop sweetener. However, saccharin has an unpleasant bitter or metallic aftertaste, especially at high concentrations. Saccharin, sold under the name Sweet’N Low™, has been approved for use in more than 100 countries. It is often combined with aspartame in diet soda. In 1972 saccharin at very high doses was found to cause an increased frequency of bladder cancer in a strain of male rats but a relationship between saccharin consumption and health risk in humans at normal consumption amounts has not been shown and is not believed to pose a concern.16
ASPARTAME
Aspartame, sold under the brand names NutraSweet™ and Equal™, is approximately 200 times sweeter than sucrose.17 It was initially approved by the FDA in 1981 for limited use as a sweetener, and extended to a larger market in 1983. Aspartame is the most widely used non- cariogenic artificial sweetener. Its primary use is in diet soft drinks, yogurt, puddings, gelatin, and snack foods. Aspartame is safe for use by people who have diabetes but should be avoided by people with phenylketonuria because they cannot metabolize phenylalanine, a component of aspartame. An interesting finding is that the oral ingestion of 6 mg of aspartame per kilogram of body weight reduced the number of sickled cells in the blood of patients with homozygous sickle cell anemia.18
The approval of aspartame by the FDA was not without dissenting opinions and there have been concerns raised relative to toxic effects of aspartame on growth, glucose homeostasis, and liver functions through longterm usage.19-23
ACESULFAME POTASSIUM (ACESLFAME K, ACE K)
Acesulfame potassium—a non-nutritive, calorie free, noncariogenic, artificial sweetener—was approved by the FDA in 1988 for use as a sweetener in specific food and beverage categories. It is 180 times to 200 times sweeter than sucrose. In 1994 yogurt, refrigerated desserts, syrups, and baked goods were added to the approved list and in 2002 it was accepted as a general-purpose sweetener. It is approved for use in foods, beverages, cosmetics, and pharmaceutical products in more than 30 countries and is marketed under the trade names Sunnett® and Sweet One®. Acesulfame potassium, like saccharin, has a slightly bitter aftertaste and is often blended with other sweeteners to give a more sugar-like taste. Unlike aspartame, acesulfame potassium is heat stable, which allows it to be used in baking. Although considered safe for consumption there have been some health issues raised relative to dose-dependent cellular toxicity.24,25
SUCROLOSE
Sucrolose, a non-nutritive, noncaloric trichlorinated derivative of sucrose, is branded as Splenda™. It was first accepted by the FDA as a tabletop sweetener in 1998 followed by acceptance as a general-purpose sweetener in 1999. It is 600 times sweeter than sucrose. Sucrolose is not metabolized by the body, is safe for people who have diabetes, and is noncariogenic. It is heat stable and is widely used throughout the world in many food products such as tea and coffee sweetener, carbonated and noncarbonated beverages, baked goods, chewing gum, and frozen desserts. No health concerns have been reported with sucrolose.26,27
NEOTAME
Neotame was approved by the FDA in 2002 as a sweetener and flavor enhancer for use in selected food products. It is a derivative of a dipeptide and although it has a similar chemical structure to aspartame, it is safe for people with phenylketonuria. Neotame is an intense noncariogenic sweetener with a clean taste and no unpleasant characteristics. It has a sweetness potency up to 13,000 times greater than sucrose, is heat stable in baking applications, and can be safely used by people who have diabetes. Similar to other sweeteners, the potency of neotame may vary depending on the food or how it is used.28,29 Neotame is functional and stable in carbonated soft drinks, powdered soft drinks, yellow cake, yogurt, and heat-sterilized noncarbonated drinks.30
OTHER SWEETENER AGENTS
 Recently the FDA has approved several additional noncaloric or reduced calorie sweeteners as GRAS (Figure 2).
Recently the FDA has approved several additional noncaloric or reduced calorie sweeteners as GRAS (Figure 2).
SORBITOL
Sorbitol is a 6-carbon sugar alcohol that occurs naturally in many fruits and berries. It is produced commercially from glucose but is expensive to manufacture. Sorbitol is often used as a bulk sweetener in a variety of food substances such as chewing gums, chocolates and confectioneries, toothpastes, and mouthwashes. It is only half as sweet as sucrose and is generally considered noncariogenic. However, it has been shown to be mildly cariogenic with prolonged use by patients who have reduced salivary gland function.31 Some concern exists relative to whether people who have diabetes should consume sorbitol. It is not easily metabolized or absorbed from the gastrointestinal tract and can cause diarrhea if ingested in large quantities.32
XYLITOL
Xylitol is a 5-carbon naturally occurring sugar alcohol (polyol). In 1890, it was discovered in birch and other hardwood chips and in wheat and oat straw in 1891.33,34 It is nonfermentable and pleasant tasting but is relatively expensive to manufacture.35 Xylitol is as sweet as sucrose but has 40% fewer calories. It was approved by the FDA in 1986. It possesses approximately the same sweetness potency as sucrose and is used primarily in chewing gum, mints, and toothpaste. It is also available for table use under the market name of Ideal™. Studies suggest that the regular use of xylitol-containing chewing gum reduces the amount of dental plaque and increases saliva flow. A significant reduction in caries incidence has been reported in cariesactive age groups when xylitol-containing gum was regularly chewed.35-39 Xylitol has also been credited for reducing the transmission of cariogenic bacteria from mother to infant and has been shown to have bacteriocidal qualities.40,41 An additional reported benefit of chewing gum that contains xylitol is a reduction in the incidence of ear infections among young children at day care centers.42 However, xylitol can aggravate symptoms of irritable bowel syndrome.43,44
ERYTHRITOL
Erythritol is a 4-carbon sugar alcohol that is manufactured by fermenting glucose. It is only about 60% to 80% as sweet as sucrose and has fewer calories (0.2 calories per gram) but does not dissolve as well in water. Erythritol has been used in Japan since 1990 as a component of candies, soft drinks, chewing gum, jams, and yogurts. It was given GRAS recognition by the FDA in 1997. Erythritol is heat stable and can be used in baking and as a general sweetener in low carbohydrate diets. It is safe for use by people who have diabetes and is noncariogenic. Erythritol is sold in North America under the names Zerose™ and Organic Zero™. One undesirable side effect of consuming large amounts of erythritol is that it may have a laxative effect in both children and adults.45
TAGATOSE
Tagatose, a low-calorie natural sugar, has all the good qualities of erythritol plus it has about the same sweetness as sucrose. It performs better in cooking, and actually improves blood sugar control in people who have diabetes.46 Tagatose has about one-third the number of calories as sucrose. It was granted GRAS status in 2001 and is used in a variety of drugs, foods, beverages, and dietary supplements. To date there have been no adverse health effects associated with the ingestion of this product when consumed in reasonable amounts. Excessive consumption can lead to mild intestinal discomfort.47
STEVIA
Stevia rebaudiana (Bertoni) is an herb in the Chrysanthemum family. An extract, stevia, is a naturally occurring, heat stable sweetener.48 The extracted active ingredient is a white crystalline material that contains three glucose molecules and steviol, a ditepenic carboxylic alcohol. Its sweetness potency is 200 times to 300 times greater than sucrose. Stevia is calorie-free, noncariogenic, and has been used by the indigenous peoples of Paraguay for centuries as a sweetener.49 It has been commercially used in China, Brazil, and Japan, and to a lesser extent in Germany, Malaysia, and Israel, for more than 25 years as a sweetener in many food categories.50 In 1995, the FDA approved the importation and use of stevia as a dietary supplement but not as a sweetener. The argument to include stevia as a food additive was a highly charged issue and it was approved only as a food supplement for many years. However, in December 2008, the FDA responded favorably to two GRAS notices for the chemically refined extract rebaudioside A (rebiana) to be used as a general- purpose sweetener.51It is available under the brand names of Truvia™ and Pure- Via™. Rebiana is also available in combination with dextrose under the name of Stevia in the Raw™ and as an extract from stevia leaves under the name of SweetLeaf™. Two companies have marketed soft drinks (Sprite Green™ and SoBe Lightwater) using rebiana.
Stevia is safe for use by people who have diabetes and it has a mild antihypertensive quality.52 It does not cause any genetic changes.53
Oral health care workers are often called on to provide knowledgeable advice regarding the importance of diet and the role of sugars in caries formation and weight control. As such, they must be familiar with alternatives to sugar and the types of food products that are available with substitute non/low caloric, noncariogenic sweetening agents.
It is difficult to totally avoid sugar in the diet as it is often added to processed food to enhance taste. However, reducing the amount and frequency of exposure to sugar in the diet of both children and adults is an important consideration in preventing caries and reducing caloric intake.51 Noncariogenic sweeteners offer an attractive alternative to sugar when used in moderation. The identification of safe, palatable, heat stable, non/low-caloric, noncariogenic sweetener substitutes for the more cariogenic and calorie heavy sugars such as sucrose, glucose, fructose, and maltose continue to be actively pursued for use by the food industry. Consumers can safely enjoy a range of nutritive and non-nutritive sweeteners when consumed in a diet that is guided by current nutrition recommendations such as the Dietary Guidelines for Americans.54 To best serve their patients, oral health care workers should stay abreast of the new alternative sweetener products that are becoming available and approved or recognized by the FDA.
REFERENCES
- Center for Disease Control and Prevention. National Oral Heal Surveillance System. Available at: www.cdc.gov/nohss. Accessed June 21, 2010.
- Ogden CL, Yanovski SZ, Carroll MD, Flegal KM. The epidemiology of obesity. Gasteroenterology. 2007;132:2087-2102.
- Wang Y, Beydoun MA. The obesity epidemic in the United States-Gender, age, socioeconomic, racial/ethnic, and geographic characteristics: A systematic review and metaregression analysis. Epidemiol Rev. 2007;29:6-28.
- Jensen ME. Diet and dental caries. Dent Clin North Am. 1999;43:615-633.
- Gustfsson BE, Wuensel CE, Lanke LS, et al. The Vipeholm dental caries study. The effect of different levels of carbohydrate intake on caries activity in 436 individuals observed for 5 years. Acta Odontol Scand. 1954;2:232-364.
- American Academy of Pediatrics Committee on Nutrition. Policy statement on prevention of overweight and obesity. Pediatrics. 2003;112:424-430.
- Sheinin A, Makinen KK. Turku sugar studies: an overview. Acta Odontol Scand. 1976;34:405-408.
- Harel-Raviv M., Laskaris M, Chu KS. Dental caries and sugar consumption into the 21st century. Amer J Dent. 1996;9:184-190.
- Holt RD. Foods and drinks at 4 daily time intervals in a group of young children. Br Dent J. 1991;170:137-143.
- Rugg-Gunn AJ. Diet and dental caries. In: The Prevention of Dental Diseases. 2nd Ed. Murray JJ, ed. New York: Oxford University Press; 1989:4-114.
- Scheinin A, Makinen KK. Turku sugar studies I-XXI. Acta Odontol Scand. 1975;33(Suppl 70):1-349.
- Koulourides T, Bodden R, Keller S, et al. Cariogenicity of nine sugars tested with an intraoral device in man. Caries Res. 1976;10:427-441.
- Kandelman D. Sugar, alternative sweeteners and meal frequency in relation to caries prevention: new perspectives. Br J Nutr. 1997;77(Suppl 1):S121-128.
- Sreebny L. Sugar and human dental caries. World Rev Nutr Diet. 1982;40:19-65.
- Burt BA. Relative consumption of sucrose and other sugars: has it been a factor in reduced caries experience? Caries Res. 1993;27(Suppl 1):56-63.
- Weinhrauch MR, Diehl V. Artificial sweeteners-do they bear a carcinogenic risk? Annals Oncology. 2004;15:1460-1465.
- Kingborn AD, Kaneda N, Baek N-I, et al. Noncariogenic intense natural sweeteners. Med Res Rev. 1998;18:347-360.
- Manion CV, Howard J, Ogle B, et al. Aspartame effect in sickle cell anemia. Clin Pharmacol Ther. 2001;69:346-355.
- Goerss AL, Wagner GC, Hill WL. Acute effects of aspartame on aggression and neurochemistry of rats. Life Sci. 2000;67:1325-1329.
- Wurtman R. Neurochemical changes following high-dose aspartase with dietary carbohydrates. New Engl J Med. 1983;389:429-430.
- Wurtman RJ. Aspartame: possible effect on seizure susceptibility. Lancet. 1985;2:1060.
- Olney JW, Faber NB, Spitznagel E, et al. Increasing brain tumor rates: is there a link to aspartame. J Neuropatho Exp Neurol. 1996;55:1115-1123.
- National Cancer Institute Fact Sheet, Artificial Sweeteners and Cancer. Available at: www.cancer.gov/cancertopics/factsheet/Risk/artificial-sweeteners. Accessed June 21, 2010.
- Mukherjee A, Chakrabarti J. In vivo cytogenetic studies on mice exposed to acesulfame-K—a non-nutritive sweetener. Food Chem Toxicol. 1997;35:1177-1179.
- Kroger M, Meister K, Kava R. Low-calorie sweeteners and other sugar substitutes: A review of the safety issues. Comprehensive Reviews Food Science Food Safety. 2006;5(2):35-47.
- Federal Register. 63:16417, April 3, 1998.
- Grice HC, Goldsmith LA. Sucralose-an overview of the toxicity data. Food Chem Toxicol. 2000;38(Suppl 2):S1-S6.
- Walters DE, Prakash I, Desai N. Active conformations of neotame and other high- potency sweeteners. J Med Chem. 2000; 43:1243-1245.
- Prakash I, Bishay IE, Desai N, et al. Modifying the temporal profile of the high- potency sweetener neotame. J Agric Food Chem. 2001;49:786-789.
- Witt J. Discovery and development of neotame. World Rev Nutr Diet. 1999; 85: 52-57.
- Wennerholm K, Arends J, Birkhed D et al. Effect of xylitol and sorbitol in chewing-gums on mutans streptococci, plaque pH and mineral loss of enamel. Caries Res. 1994;28:48-54.
- Hyams JS. Sorbitol intolerance: an unappreciated cause of functional gastrointestinal complaints. Gastroenterology. 1983; 84:30-33.
- Bertrand MG. Rechercheszur quelques derives du xylose. Bull Soc Chim Paris. 1891;5:554-557.
- Fischer E, Stahel R. Zur kenntnis der xylose. Ber Dtsch Chem Ges. 1891;24:528- 539.
- Isokangas P, Alanen P, Tiekso J, et al. Xylitol chewing gum in caries prevention: a field study in children. J Am Dent Assoc. 1988;117:315-320.
- Makinen KK, Bennett CA, Hujoel PP, et al. Xylitol chewing gum and caries rate: a 40 month cohort study. J Dent Res. 1995;74:1904-1913.
- Autio, JT. Effect of xylitol chewing gum on salivary streptococcus mutans in preschool children. J Dent Child. 2002;69:81-86.
- Hayes C. The effect of non-cariogenic sweeteners on the prevention of denal caries: A review of the evidence. J Dent Ed. 2001;65:1106-1109.
- Makinen KK, Makinen PL, Pape HR Jr, et al. Conclusion and review of the Michigan xylitol program (1986-1995) for the prevention of dental caries. Int Dent J. 1996;46:22-34.
- Makinen KK. The rocky road of xylitol to its clinical application. J Dent Res. 2000;79:1352-1355.
- Makinen KK, Isotupa KP, Kivilompolo T, Makinen PL, Toivanen J, Soderling E. Comparison of erythritol and xylitol saliva stimulants in the control of dental plaque and mutans streptococci. Caries Res. 2001;35:129-135.
- Uhari M, Kontiokari T, Koskela M, Niemela M. Xylitol chewing gum in prevention of acute otitis media: double blind randomized trial. Brit Med J. 1996;313:1180- 1184.
- Newberne PM, Conner MW, Estes P. The influence of food additives and related materials on lower bowel structure function. Toxicol Pathol. 1988;16:184-199.
- Ludwig B, Schindler E, Bohl J, Pfeiffer J, Kremer G. Reno-cerebral oxalosis induced by xylitol. Neuroradiology. 1984;26:517-521.
- What is Erythritol Sweetener? Available at: www.ehow.com/facts_5028505_erythritol-sweetener.html. Assessed June 21, 2010.
- Donner TW, Wilber JF, Ostowski D. D-tagatose, a novel hexose: acute effects on carbohydrate tolerancein subjects with and without type 2 diabetes. Diabetes, Obesity and Metabolism 1999;1:285-289.
- Levin GV. Tagatose, the GRAS sweetener and health product. J Medicinal Food. 2002;5:23-36.
- Cardello HMAB, Da Silva MAPA, Damasio MH. Measurement of the relative sweetness of stevia extract, aspartame and cyclamate/saccharin blend as compared to sucrose at different concentrations. Plant Foods Hum Nutr. 1999;54:119-130.
- Lewis WH. Early uses of stevia rebaudiana (Asteraceae) leaves as a sweetener in Paraguay. Econ Bot. 1982;46:336-337.
- Nabors LO, Gelardi RC. Alternative Sweeteners. 2nd ed. New York: Marcel Dekker Inc; 1991:1-450.
- Agency Response Letter GRAS Notice No. GRN 000253. Available at: www.fda.gov/Food/FoodIngredientsPackaging/ GenerallyRecognizedasSafeGRAS/GRASListings/ucm154989.htm. Accessed June 21, 2010.
- Chan P, Tomlinson B, Chen Y-J, et al. A double-blind placebo-controlled study of the effectiveness and tolerability of oral stevioside in human hypertension. Br J Clin Pharmacol. 2000;50:215-220.
- Matsui M, Matsui K, Kawasaki Y, et al. Evaluation of the genotoxicity of stevioside and steviol using in vitro and one in vivo mutagenic assays. Mutagenesis. 1996;11:573-579.
- Position of the American Dietetic Association. Use of nutritive and non-nutritive sweetners. J Am Diet Assoc. 2009;104:255-275.
From Dimensions of Dental Hygiene. July 2010; 8(7): 58-61.
