 ANDRESR/E+/GETTY IMAGES PLUS
ANDRESR/E+/GETTY IMAGES PLUS
The Role of Fluoride in Caries Prevention
With a variety of concentrations, application types, and delivery methods, clinicians can recommend the right fluoride product for their patients’ individual needs.
Dental caries remains the most common chronic disease of childhood.1 According to a National Center for Health Statistics data brief on dental caries and dental sealant prevalence in the United States, 37% of children age 2 to 8 experienced caries in primary teeth and 60% of adolescents age 12 to 19 developed caries in permanent teeth from 2011 to 2012.2 The fight against caries remains ongoing and multifaceted. To date, however, fluoride remains the most effective tool in the caries prevention armamentarium.
APPLICATION AND CONCENTRATION
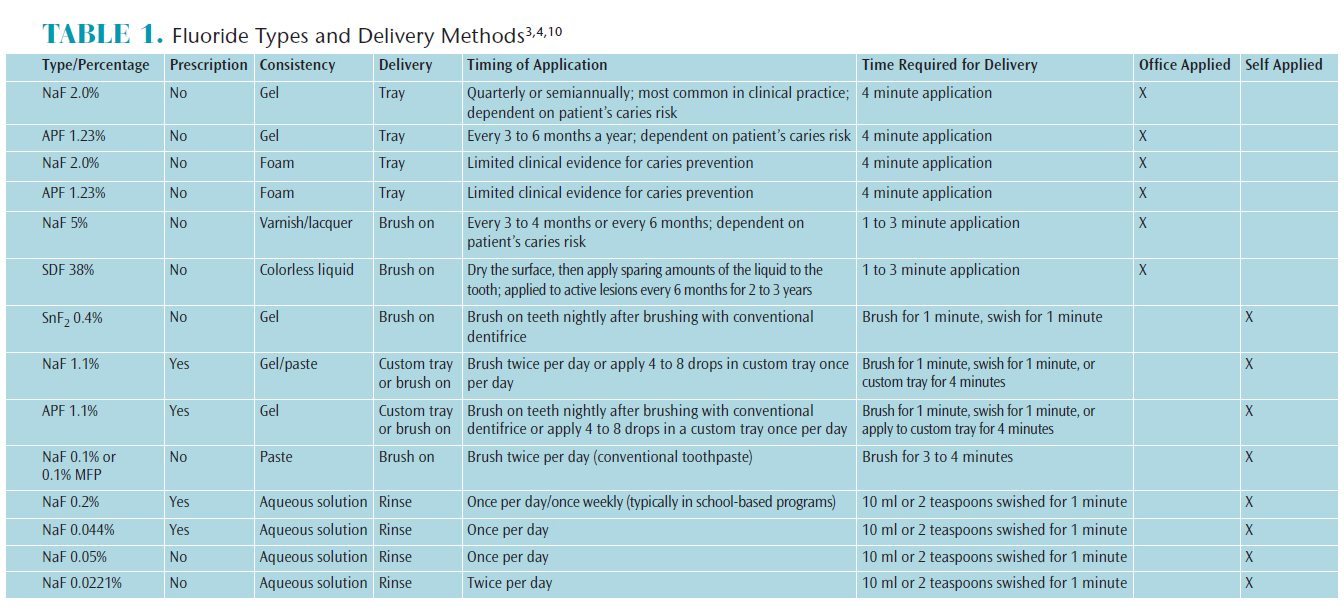
Fluoride is available in different compounds, consistencies, and delivery methods. Professionally applied fluorides include neutral sodium fluoride (NaF), acidulated phosphate fluoride (APF), stannous fluoride (SnF2), and silver diamine fluoride (SDF).3–5 These compounds are available in different application methods, such as gel, foam, varnish, or liquid, as well as varying percentages of fluoride concentration. There are also different delivery methods such as trays, brush-on varnishes, or liquids.4 The concentration of 5% NaF is available as a brush-on varnish for professional application, while 2.0% NaF and 1.23% APF concentrations come in a gel or foam that is applied via trays.3
In 2013, the American Dental Association’s Council on Scientific Affairs (ADA CSA) conducted a systematic review and published clinical recommendations for the use of professionally applied fluoride.6 The findings support a 4-minute application of both NaF and APF.6 Limited evidence was found to support the use of foam for coronal caries prevention in all age groups.6 Studies have shown that 1.23% fluoride gel and 5% NaF varnish are effective in reducing caries in high-risk children.7
SDF is used to arrest and prevent caries and reduce dentinal hypersensitivity.5,9,10 SDF is a colorless topical medicament composed of 25% to 29% silver, 5% to 6% fluoride, and ammonia.8 The silver component acts as an antimicrobial agent, while the fluoride aids in remineralization. The ammonia is used to stabilize the solution.5 In vitro studies show that artificial lesions treated with silver diamine fluoride become more resistant to biofilm formation and additional caries formation.8-10
Over-the-counter (OTC) self-applied fluoride compounds are NaF, APF, and SnF2. They are available as gels, pastes, and liquids. The concentrations vary from a low-potency solution of 0.0221% to a prescription-strength solution of 0.2% or 0.044%. The liquid is swished for 1 minute daily. NaF and APF are also available as a 1.1% prescription gel or paste. Self-applied gels and pastes are brushed-on or used in custom trays. The compound 0.4% SnF2 is a gel that is brushed-on nightly after brushing with an OTC fluoride dentifrice. OTC fluoride dentifrices contain 0.1% NaF or 0.1% sodium monofluorophosphate (MFP) and are used twice daily. Table 1 provides details on fluoride compounds, consistencies, and delivery methods.
CONCLUSION
Prevention is the best approach when addressing dental caries in all age groups. Implementing an evidence-based approach that utilizes caries risk assessment tools and protocols sets the stage for the best possible oral health outcomes.11 Evidence shows that fluoride is a safe and effective method of caries prevention, regardless of which type of compound, consistency, or delivery method is implemented.12
References
- Benjamin RM. Oral health: the silent epidemic. Public Health Rep. 2010;125:158–159.
- Dye BA, Thornton-Evans G, Li X, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011-2012. NCHS Data Brief. 2015;191:1–8.
- Wilkins EM, Wyche CJ, Boyd LD. Fluorides. Clinical Practice of the Dental Hygienist. 12th ed. New York: Wolters Kluwer; 2017:593–618.
- Walsh M, Darby ML. Dental Hygiene Theory and Practice. 4th ed. Philadelphia: Saunders; 2015.
- Rosenblatt A, Stamford T, Niederman R. Silver diamine fluoride: a caries “silver-fluoride bullet.” J Dent Res. 2009;88:116–1125.
- Weyant RJ, Tracy SL, Anselmo TT, et al. American Dental Association Council on Scientific Affairs expert panel on topical fluoride caries preventive agents: Topical fluoride for caries prevention: Executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013;144:1279–1291.
- American Academy of Pediatric Dentistry. Guideline on fluoride therapy. Pediatr Dent. 2013;35:E165.
- Featherstone J, Horst JA. Fresh approach to caries arrest in adults. Decisions in Dentistry. 2015;1:36–44.
- Knight GM, McIntyre JM, Craig GG, Mulyani, Zilm PS, Gully NJ. Inability to form a biofilm of streptococcus mutans on silver fluoride- and potassium iodide-treated demineralized dentin. Quintessence Int. 2009;40:155–161.
- Horst JA, Ellenikiotis H, Milgrom PM, UCSF Silver Caries Arrest Committee. UCSF protocol for caries arrest using silver diamine fluoride: Rationale, indications, and consent. J Calif Dent Assoc. 2016;44:16.
- Jenson L, Budenz AW, Featherstone JD, Ramos-Gomez FJ, Spolsky VW, Young DA. Clinical protocols for caries management by risk assessment. J Calif Dent Assoc. 2007;35:714–723.
- American Academy of Pediatric Dentistry. Guideline on Fluoride Therapy. Available at: aapd.org/media/Policies_Guidelines/G_fluoridetherapy.pdf. Accessed January 19, 2017.
From Dimensions of Dental Hygiene. February 2017;15(2):21-22.

{kind=link}