 MICROGEN/ISTOCK/GETTY IMAGES PLUS
MICROGEN/ISTOCK/GETTY IMAGES PLUS
Risks to Oral Health Posed by Swimming
Teeth stain, dental pain, calculus buildup, and dental erosion can be side effects of exposure to pool chlorine.
This course was published in the August 2018 issue and expires August 31, 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the negative oral health effects of swimmer’s mouth.
- Discuss the importance of properly maintaining pool chemicals in preserving oral health.
- Recommend appropriate preventive strategies.
The standard recare interval to maintain oral health is every 6 months.4 Swimmers may need more frequent recare intervals and a personalized prevention regimen to reduce the effects of consistent exposure to chlorinated water. This article will discuss the possible oral health effects of chlorine exposure and provide prevention methods to counter the effects of chlorine on the oral cavity.
TOOTH STAINING
Staining of the dentition is one effect of exposure to pool chlorine. Teeth stain is a problem for swimmers because pool water contains chemical additives—such as antimicrobials—that give the water a higher pH than saliva. This causes salivary proteins to break down quickly and form organic deposits on swimmer’s teeth. Athlete swimmers, who swim laps more than 6 hours a week, expose their teeth to large amounts of chemically-treated water. The result is hard, brown calculus deposits that appear most frequently and noticeably on the front teeth (Figure 2 and Figure 3).5
DENTAL PAIN
Swimmers with predisposing oral pathology— such as acute or chronic periapical infection, caries, deep or failing restorations, or residual dental cysts, and those with sinusitis or recent history of surgery—are at risk of barodontalgia. Barodontalgia, which is characterized by dental pain, occurs when the teeth are exposed to a pressure gradient, such as that experienced by underwater divers or air travelers. Swimmers who frequently dive to the bottom of the deep end of a pool to perform breathing exercises and retrieve weights are at risk of barodontalgia. Research indicates that the severity of barodontalgia and the resulting deterioration of oral health correlate with the duration of barometric stress.6
Restorative materials are commonly affected by pressure gradients. Ultimately, the key to avoiding barodontalgia is optimum oral health. Oral health professionals should pay close attention to areas of dentin exposure, caries, fractured cusps, integrity of restorations and periapical pathology in at-risk patients.6
INCREASED CALCULUS BUILD UP
It takes just a day for bacteria to build up enough to make the mouth susceptible to disease.7 After exposure to fermentable carbohydrates, bacteria release acids, breaking down the enamel surfaces of teeth, especially above and below the gingival line and interdentally. Repeated acid attacks increasingly erode the enamel, eventually causing tooth decay and stain.8 Antimicrobials found in pool water have a much higher pH than saliva, which causes the proteins to break down and discolored deposits to form.
When plaque accumulates beneath the gingival margin, the associated buildup of bacteria and calculus can cause irritation and inflammation of the gingival tissue, leading to gingivitis and periodontal diseases. Irritated and inflamed gingiva typically appears red, or erythematous, and can bleed. Continued biofilm plaque accumulation can contribute to structural damage to teeth and the bone supporting the teeth and gingiva, as well as other health complications.9

DENTAL EROSION
Tooth structure starts to demineralize at a pH below 5.5. Specifically, caries lesions can develop on dentin starting at a pH of 6.0 to 6.9, and on enamel at a pH of 5.2 to 5.5.10 If a swimming pool is kept at the optimal pH of 7.4, tooth structure will not demineralize. However, if the pH of the swimming pool water becomes acidic, then exposed tooth structures may start to dissolve. This is usually seen in gas-chlorinated pool systems. The most inexpensive type of chlorination, chlorine as a gas provides 100% available chlorine and, therefore, requires strict safety procedures as inappropriate exposure is dangerous. This type of chlorination is uncommon today and is used mostly in very large, old public pools. Chlorine gas is highly acidic.11 Normally, swimming pools counteract this acid with a strong base, such as ash. If the swimming pool does not get enough base to counter the acid from the chlorine, then it can become acidic and start to dissolve the teeth of those who swim regularly.3
One study suggested that 15% of daily swimmers displayed enamel erosion, while only 3% of infrequent or nonswimmers experienced enamel erosion.12 A case report also details the significant dental erosion experienced by a competitive swimmer who swam in a gas-chlorinated swimming pool and experienced notable dental erosion within 27 days.3 Today, most public pools are more careful about testing the pH of the water to ensure it is not too acidic. However, this problem can still occur if regular pool maintenance is neglected.13
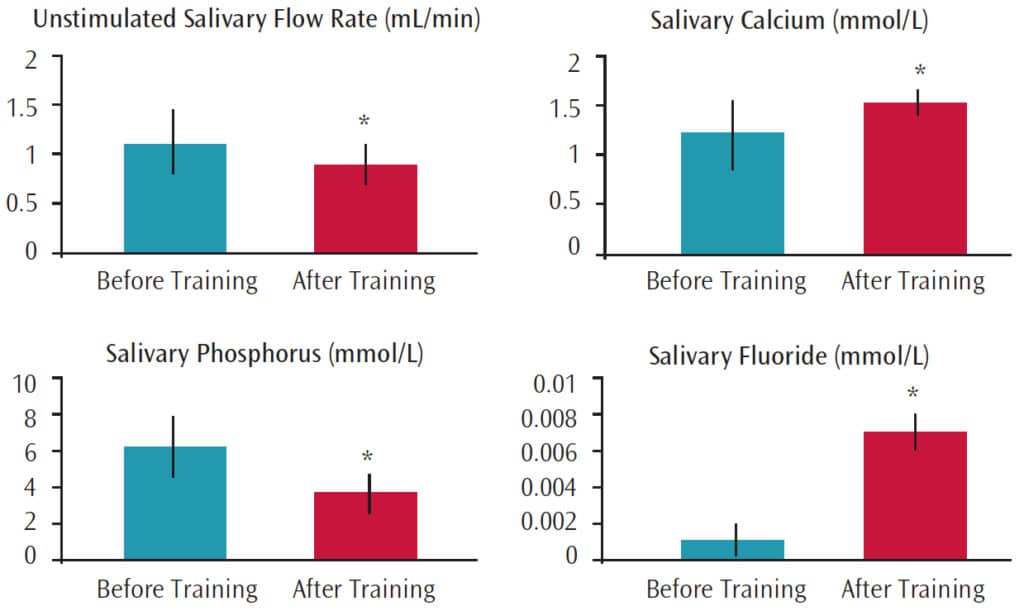
In a study of 22 competitive swimmers, researchers found that the composition and flow rates of their saliva were greatly impacted by the exposure to chemically treated water during swimming. The swimmers’ salivary flow rates and levels of phosphorus decreased, while their calcium and fluoride levels increased (Figure 4).14 With an increase in calcium and fluoride and a decrease in phosphorus, calculus formation is exaggerated. By decreasing the salivary flow, the oral environment is drier than normal and the amount of saliva is inadequate for flushing the debris and chlorine from the mouth. Saliva has a primary role of neutralizing the environment of the oral cavity.

CHLORINATION OF POOL WATER
Educating pool maintenance employees on the harmful effects of over-chlorinating pools is necessary. The pool water should be monitored carefully to keep the chemistry within normal ranges. The US Centers for Disease Control and Prevention recommends keeping the chlorine concentrations between 1.0 ppm and 3.0 ppm.13 Chlorine kills bacteria, but it takes time to work. Therefore, chlorine concentrations should always remain at the appropriate levels. When water is too acidic, it can erode pool linings, railings, and ladders. If there are areas of erosion and stain on such pool surfaces, the water could affect swimmers’ tooth structures in a similar manner.
The pH level of every swimming pool is important to monitor for two reasons. First, the bacteria-killing power of chlorine varies with the pH level of the pool. As pH goes up, the ability of chlorine to kill bacteria decreases. Second, a swimmer’s body has a pH between 7.2 and 7.8, so if the pool water is not kept in this range, the swimmers will begin to feel irritation in his or her eyes and skin. A pH below 7.0 or above 8.0 can be harmful.15
The optimum pH level in a pool is 7.2 to 7.8, which is considered a basic solution. In general, solids dissolve in acid and precipitate in bases. This means that in a basic swimming pool, the calcium and minerals present in the mouth will harden onto the teeth rather than dissolve (as they would if the pH were acidic, which is why teeth dissolve slowly when anything acidic is consumed). The higher the pH of the swimming pool, in combination with the antimicrobial compounds of the pool water, the more likely the proteins in the mouth will break down and mesh together with the minerals in the mouth to form a hard, yellowish-brown mineral deposit on the teeth.16
STRATEGIES TO REDUCE HARM
How often swimmers practice in a week is important. Depending on the swim team and individual swimmer, practices can be as often as twice a day, six days per week. This extended exposure to chemically treated water can be problematic. However, each swimmer will have individual responses to environmental factors.3,17 Coaches can help swimmers develop an appropriate breathing system that minimizes the mouth opening to reduce exposure to pool water. Swimmers may also benefit from rinsing with a solution to neutralize the acidity in the mouth following pool exposure.3
Appropriate oral hygiene habits should be assessed. These include proper brushing and interdental cleaning, in addition to the use of mouthrinse. Brushing the teeth immediately after swimming can be harmful, as the enamel surface is softened by the acidic chlorine and may be more easily brushed away.3 Therefore, simply rinsing with water, baking soda, or fluoride mouthrinse immediately after practice may help return the oral cavity to a neutral pH, decreasing the risk of acid erosion. Regularly receiving professional oral health care will reduce the presence of stain on the teeth.
The use of fluoride mouthrinse is also beneficial for caries prevention and may be a prudent addition to a swimmer’s oral hygiene regimen. A literature review of fluoride mouthrinses as a means of preventing dental caries in children and adolescents found that regular, supervised use of a fluoride mouthrinse by children and adolescents reduced caries and stain in permanent teeth.18
The topical application of fluoride varnish or gel in the professional dental setting may also support oral health in this population. The use of prescription fluoride mouthrinses or toothpastes may be indicated. Swimmers may want to rinse or brush with a fluoride product before entering the pool to prevent teeth from damage.
Chewing gum containing xylitol may also help swimmers reduce their caries risk. Individuals need to consume 5 g to 6 g of xylitol at least three times or more per day to gain caries-prevention benefits.19,20 In addition to gum, xylitol can also be found in syrups, wipes, dentifrices, lozenges, mouthrinses, and snack foods.19.20 Agents designed to support enamel health, such as arginine, and remineralization, such as calcium phosphate technologies, may also be helpful.19–21 The use of a power toothbrush may be beneficial. Research shows that the use of a power brush can significantly reduce stain and buildup on teeth when compared with manual toothbrushes.22 Oral health professionals should make individualized recommendations after evaluating medical and dental histories and clinical examinations.
SUMMARY
Asking patients about their exposure to chemically treated pools is prudent when developing appropriate recare intervals and recommending oral hygiene regimens. Should oral health professionals notice a patient is experiencing negative oral health effects related to pool exposure, they should suggest that the patient and/or parent/caregiver check with the local swimming pool maintenance coordinator to ensure the pH level of the pool is within normal limits.9
REFERENCES
- USA Swimming. About USA Swimming. Available at: usaswimming.org/Home/about/usa-swimming. Accessed July 10, 2018.
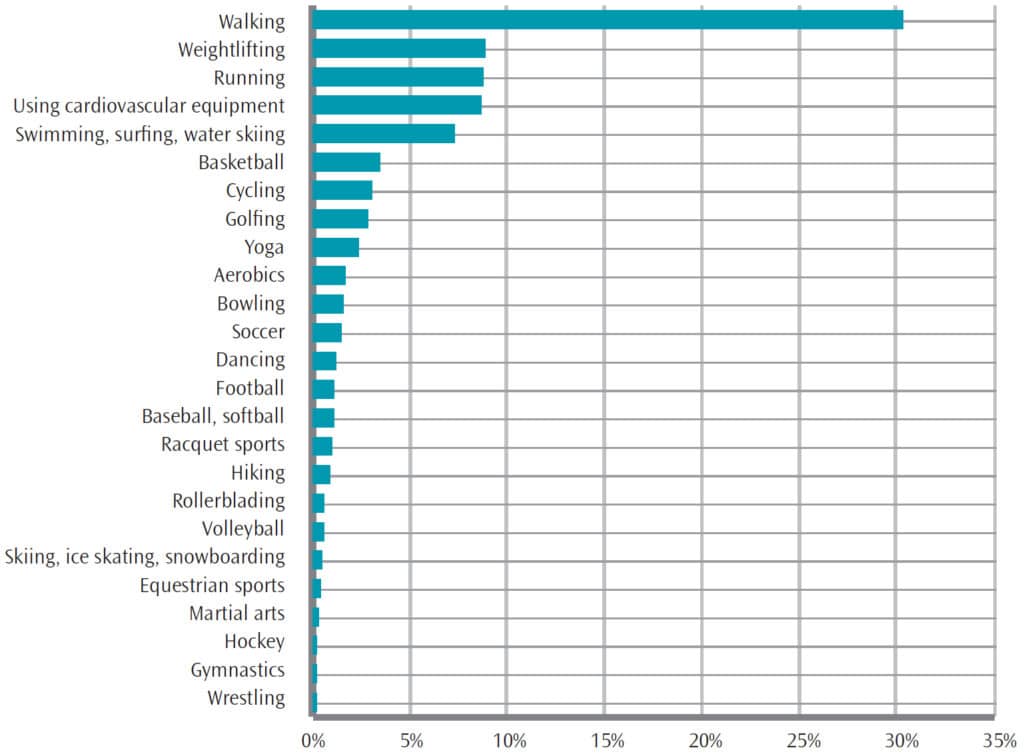
- United States Bureau of Labor Statistics. Exercise Among Americans. Available at: bls.gov/opub/ted/ 2016/sports-and-exercise-among-americans.htm. Accessed July 10, 2018.
- Centerwall BS, Armstrong CW, Funkhouser LS, Elzay RP. Erosion of dental enamel among competitive swimmers at a gas-chlorinated swimming pool. Am J Epidemiol. 1986;123:641–647.
- Valier AR, Lam KC. Beyond the basics of clinical outcomes assessment: selecting appropriate patient-rated outcomes instruments for patient care. Athletic Training Education Journal. 2015;10(1):91–100.
- Swimmers teeth not pearly white? JAMA. 1995;274:1902.
- Robichaud R, McNally M. Barodontalgia as a differential diagnosis: symptoms and findings. J Can Dent Assoc. 2005;71:39–42.
- Baghele ON. Prevalence of dental erosion among young competitive swimmers: a pilot study. Compend Contin Educ Dent. 2013;34:e20–24.
- Watts A, Addy M. A review of tooth discoloration and staining. Br Dent J. 2001;190:309–316.
- Virginia T, Schoeler L. Can chlorine in swimming pools dissolve or stain your teeth? South African Journal of Sports Medicine. 2009;21:1.
- Delgado AJ, Olafsson VG. Acidic oral moisturizers with pH below 6.7 may be harmful to teeth depending on formulation: a short report. Clin Cosmet Investig Dent. 2017;9:81–83.
- Pool Info: Chlorine Pool Chemistry. Available at: poolcenter.com/chlor. Accessed July 10, 2018.
- Leads from the MMWR. Erosion of dental enamel among competitive swimmers—Virginia. JAMA. 1983;250:716.
- From the CDC: Swimming pools need more chlorine. Journal of the American Osteopathic Association. 1999;99(8):396.
- Bretz WA, Carrilho MR. Salivary parameters of competitive swimmers at gas-chlorinated swimming-pools. J Sports Sci Med. 2013;12:207–208.
- Zebrauskas A, Birskute R, Maciulskiene V. Prevalence of dental erosion among the young regular swimmers in Kaunas, Lithuania. J Oral Maxillofac Res. 2014;5:2.
- Hara AT, Carvalho JC, Zero DT. In: Causes of dental erosion: extrinsic factors. In: Amaechi BT, ed. Dental Erosion and its Clinical Management. New York: Springer; 2015:69–96.
- Barker T. Correlation analysis with scatter plots. In: Pro Data Visualization Using R and JavaScript. New York: Apress Media LLC; 2013:157–176.
- Bidwell J. Fluoride mouthrinses for preventing dental caries in children and adolescents. Public Health Nurs. 2017;35:85–87.
- Riley P, Moore D, Ahmed F, Sharif MO, Worthington HV. Xylitol-containing products for preventing dental caries in children and adults. Cochrane Database Syst Rev. 2015;3:CD010743.
- Richards D, Duane B, Sherriff A. Maternal consumption of xylitol for preventing dental decay in children. Available at: cochranelibrary-wiley.com/doi/10.1002/14651858.CD010202/abstract;jsessionid=A121CC3D4630C45CE876F1AA548CF8F6.f02t02. Accessed July 10, 2018.
- Rethman MP, Beltrán-Aguilar ED, Billings RJ, et al. Nonfluoride caries preventive agents. Full report of a systematic review and evidence-based recommendations. J Am Dent Assoc. 2011;142:1065–1071.
- Hunt SA. The relative cleaning effectiveness of manual and powered toothbrushes. J Clin Dent. 2002;13:211–2114.
From Dimensions of Dental Hygiene. August 2018;16(8):45-48.
