Nutritional Strategies for Caries Reduction
Diet plays an integral role in promoting oral health.
This course was published in the August 2014 issue and August 31, 2017. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVE
After reading this course, the participant should be able to:
- Explain how the consumption of fermentable carbohydrates affects dental biofilm.
- Discuss how changes in modern eating habits have affected caries risks.
- Detail food choices that can inhibit caries incidence.
Dental caries is a chronic biofilm-mediated disease that originates from the interplay of cariogenic bacteria on the dentition, diet, and environment.1 Dental caries is a major health concern, and its treatment and management result in some of the highest direct costs of any disease. The expense of treatment is directly related to the progressive nature of tooth decay.2 While caries is a serious disease, it is also entirely preventable. Diet is an important factor in the fight against decay. Recent advances in the understanding of dental caries pathology support the role of dietary control in preventing tooth decay and promoting oral health.
Dental caries results from the interaction of specific bacteria within a type of biofilm called dental plaque.3 The normal oral flora is a multispecies biofilm that includes the cariogenic Streptococcus mutans, S. sobrinus, Lactobacillus, and Actinomyces, and the less cariogenic nonmutans streptococci.4 In fact, cariogenic bacteria obtain nutrients and produce lactic acid as a byproduct of fermentation, which results in acidification of the plaque, followed by demineralization of the enamel that may result in early signs of decay.
Frequent consumption of fermentable carbohydrates can negatively shift the ecological balance of the oral microflora. This sugar-driven biofilm alteration is associated with high proportions of acidogenic and aciduric (acid-tolerating) bacteria. This diet-driven increase in cariogenic species reduces healthy bacteria.4 Beighton5 revealed that excluding or reducing the fermentable carbohydrate content of the diet could beneficially modify the caries-inductive flora.
According to the extended ecological plaque hypothesis suggested by Takahashi and Nyvad,6 maintaining a microbial balance in the oral cavity neutralizes the acid producers in plaque biofilm and creates an environment that is favorable to the microflora that supports dental health. Environmental factors that change the composition and biochemical activities of plaque, such as the frequent consumption of fermentable carbohydrates, can result in a flora that shifts the pH balance of the biofilm toward demineralization and enamel loss.1,4,6
Despite the fact that caries is caused by a variety of bacterial species, there remains a strong relationship between caries development and high levels of S. mutans.7 Reducing the prevalence of these bacteria in the plaque community is one caries to re-establishing healthy plaque.1 Beighton5 describes S. mutans as an organism implicated in caries that is lacking the ability to endure environmental changes imposed by outside agents. For example, Tong et al8 discovered that S. oligofermentans, which exist exclusively in caries-free individuals, can inhibit S. mutans growth through metabolizing lactic acid into hydrogen peroxide.
DIET AND CARIES RISK
Dietary habits are influenced by genetic, cultural, and environmental factors. In a sample of 1,305 American children (age 3 to 12), Shaffer et al9 presented the first genome-wide association scan for dental caries that found several novel candidate genes that affect dental caries, including ACTN2, MTR, EDARADD, MPPED2, and LPO. The role of genes in the incidence of dental caries can be processed at two levels: enamel composition and taste sense. Genes that interfere with tooth enamel composition, such as ACTN2 and MTR, may increase caries susceptibility.9
To determine why people differ in their dietary choices, Shaw and Murray10 revealed that individuals’ genetic structures appear to influence the desire to consume carbohydrates. Genetic predisposition may also explain why some people consume low levels of sugar. For example, Rupesh and Nayak11 examined genetically determined taste sensitivity and noted that individuals with low sweet-taste sensitivity had a lower caries risk than those with high sweet-taste sensitivity. Likewise, Wendell et al12 identified two genes important to taste sensitivity—TAS2R38 and TAS1R2—that are associated with dental caries risk and/or protection. However, predicting dietary choices and diet-associated conditions with taste receptor specificity is not possible at this time.13
Eating habits have changed dramatically in recent decades. The daily intake of energy-dense, low-nutrient snack foods has greatly increased.14 Johansson et al14 conducted a large cohort study that revealed a significant association between the consumption of potato chips and caries status. The combination of starch and sucrose found in potato chips is what most likely increases their cariogenicity. In vivo studies have demonstrated that the hydrolyzed starch in chips has a rapid and significant pH-lowering effect that is similar to sucrose.15
The development of dental caries depends on several species of cariogenic bacteria and specific eating patterns. The more sugar the individual eats, the more nutrients the cariogenic bacteria receive. For example, the frequency of intake of foods and drinks sweetened with sucrose appears to be positively related to the incidence of dental caries.16 On the other hand, water and milk consumption have protective qualities against dental caries, especially in the primary dentition. Unfortunately, plain water and milk consumption has declined in the modern diet.17 Changes in beverage patterns—especially the increased consumption of soft drinks and powdered beverages—may increase dental caries rates among children.18 In addition, the consumption of sugary drinks at night or between meals is strongly associated with an increase in dental caries among preschool children.19 Such findings strongly support the need to limit access to soft drinks—particularly among school-age children.17
Poor eating habits can create a more favorable environment for cariogenic bacteria to thrive. Therefore, dietary alterations combined with organized community efforts are promising methods of promoting oral health, especially among children at high-caries risk.
CARIOSTATIC FOOD CHOICES
Sucrose is the most cariogenic carbohydrate.20 As such, sugar substitutes have emerged as promising alternatives to sucrose. Sugar substitutes commonly used to prevent caries are either sugar alcohols or artificial sweeteners. The United States Food and Drug Administration approves “sugar-free” products sweetened only with sugar alcohols, artificial sweeteners, or a combination of these sweeteners.21 These sugar alcohols or polyols are nonfermentative dietary sweeteners and include xylitol, D-glucitol (sorbitol), erythritol, mannitol, and maltitol.21 The most commonly used option is xylitol, which is a nonfermentable natural sugar alcohol. Xylitol is used worldwide as a sugar substitute. Clinical studies have shown that xylitol, within certain doses and frequencies, can be used as a safe and effective caries-limiting sweetener that reduces the number of mutans streptococci.22 The use of xylitol-containing products is recommended because the habitual use of xylitol is associated with a significant reduction in caries incidence and lesion remineralization.22,23 Xylitol is an effective noncariogenic sucrose substitute, and it may also be an effective anticariogenic agent.23
Artificial sweeteners also include aspartame, saccharine, sucralose, and acesulfame potassium, which are all noncariogenic. Due to their intense sweetness, artificial sweeteners are frequently added in small amounts to improve the flavor of sugar alcohols, which are typically less sweet.21
In recent years, much research and education have focused on the identification of food components and products with disease-preventing and health-promoting benefits. These “functional foods” are defined as foods that have the ability to reduce the risk of chronic disease, beyond their nutritional value.24 For example, Hu et al25 discovered that a novel compound (glycyrrhizol A)—which is extracted from licorice roots and manufactured in sugar-free lollipops—exerts a strong antimicrobial response to cariogenic bacteria. Wu24 found that grape seed extract, which is a rich source of proanthocyanidin, showed a positive effect on the remineralization of root caries lesions. Somanah et al26 investigated the effect of fermented papaya preparation on the growth, hydrophobicity, and acid production of S. mutans , S. mitis, and Lactobacillus acidophilus among individuals with diabetes. Results showed that low doses of the fermented papaya preparation helped reduce caries, plaque, and gingivitis in a high-risk population.
FIGURE 1. DR MARK J. WINTER / SCIENCE PHOTO LIBRARY
Raisins and cranberries appear to exert oral health benefits. The polyphenols in cranberries can reduce the formation of plaque biofilm and inhibit the production of acids by cariogenic bacteria.27 Green tea is considered a functional food for oral health due to its high content of catechins—especially epigallocatechin-gallate, which possesses antimicrobial effects against oral streptococci (Figure 1).28 While the use of functional foods is promising, the supporting evidence should be interpreted with caution, as most of these trials are in vitro or conducted on animals.
FIGURE 2. ALFRED PASIEKA / SCIENCE PHOTO LIBRARY
Milk and milk products are considered caries protective. Milk protein is an effective buffer, and dairy products contain bioactive components with cariostatic properties (calcium, phosphate, casein, whey protein, lactose, and milk fat).29,30 For example, casein (Figure 2)—which is 80% of the bovine milk protein and 20% to 45% of human milk protein—seems to inhibit the adhesion of mutans streptococci to saliva-coated hydroxyapatite. Casein also helps calcium phosphates reach demineralized surfaces on the tooth.31,32 Milk also contains whey proteins, lactoferrin, lysozyme, and antibodies that promote oral health via their interactions with various cariogenic bacteria.32 Likewise, Tanaka et al29 found an association between a high consumption of yogurt and a low prevalence of dental caries in young children. Llena and Forner33 reported that the intake of cheese and nuts was associated with reduced caries incidence.
Probiotics, the fermented milk products that contain viable bacteria, also appear to protect against dental caries.34,35 Probiotics can be introduced through various media, including milk, yogurt, cheese, ice cream, chewing gum, tablets, lozenges, and oral rinses.36 Several clinical studies revealed that a regular daily consumption of probiotic lactobacilli and bifidobacterium decreased the number of cariogenic streptococci in saliva and dental plaque, resulting in reduced caries risk.34,35,37
A systematic review37 that investigated the effects of probiotics on caries incidence and the levels of mutans streptococci and/or lactobacilli found that probiotics reduced the numbers of mutans streptococci. The difference observed in the effects of probiotics on lactobacilli counts was not statistically significant. Haukioja et al38 and Slawik et al39 reported that the cariogenic potential of lactobacilli and the high-sugar content of probiotic milk drink should be investigated in future long-term studies. There is a need for controlled and well-designed clinical trials that investigate the probiotic microbiota and their acidogenicity.
The use of functional foods may be a helpful adjunct to traditional caries prevention strategies, such as effective oral hygiene, fluoride therapy, sealants, and regular professional dental care. Additional randomized clinical trials are needed before the cariostatic activity mechanism of functional foods are well understood.
ORAL HEALTH EDUCATION
 Caries is a multifactorial disease that is affected by many factors, including social and economical determinants, such as behavior, knowledge, attitude, education, socioeconomic status, and income.40 Efforts to adjust dietary behavior through oral health education programs have been undertaken across the world.16 For instance, Köhler and Andréen41 demonstrated a successful reduction of S. mutans in children and their mothers who participated in a preventive program that included dietary counseling. This reduction of S. mutans was associated with delayed bacterial colonization and reduced caries incidence in children when offered to mothers during the emergence of their children’s primary teeth.41
Caries is a multifactorial disease that is affected by many factors, including social and economical determinants, such as behavior, knowledge, attitude, education, socioeconomic status, and income.40 Efforts to adjust dietary behavior through oral health education programs have been undertaken across the world.16 For instance, Köhler and Andréen41 demonstrated a successful reduction of S. mutans in children and their mothers who participated in a preventive program that included dietary counseling. This reduction of S. mutans was associated with delayed bacterial colonization and reduced caries incidence in children when offered to mothers during the emergence of their children’s primary teeth.41
Oral hygiene education and promotion integrated with dietary counseling are integral to the prevention of dental caries. Tinanoff and Palmer42 found that teaching parents/caregivers how to reduce high-frequency exposures to sugars was helpful in reducing caries rates. Likewise, Moynihan and Petersen43 suggest that combining oral hygiene instruction with nutrition education in schools and in childbirth curricula is effective. In a practice-based intervention, Kressin et al44 revealed that clinicians significantly reduced the incidence of early childhood caries through parental counseling. While further research is needed to support the direct role of oral hygiene instruction in reducing caries, dental visits should still incorporate oral health promotion, patient education, and patient compliance strategies.
CONCLUSION
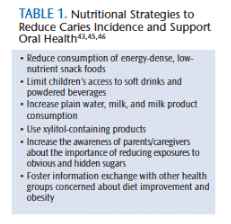
Improving nutrition literacy and encouraging healthy food choices may help reduce caries rates, which is especially important among vulnerable populations. Table 1 summarizes the key nutritional strategies that can decrease caries incidence and support oral health.43,45,46
The direct relationship between nutrition and dental caries is complicated. Thus, there is a clear need for further exploration into the nutritional factors related to the prevention and/or treatment of dental caries. Such studies would offer important clinical implications for future efforts in caries prevention. In addition, effective preventive strategies should consider the potential role of oral health promotion, dietary counseling, and public nutrition education.
REFERENCES
- Smith EG, Spatafora GA. Gene regulation in S. mutans : complex control in a complex environment. J Dent Res. 2012;91:133–141.
- Sheiham A. Dietary effects on dental diseases. Public Health Nutr. 2001;4:569–591.
- Bowen WH. Do we need to be concerned about dental caries in the coming millennium. Crit Rev Oral Biol Med. 2002;13:126–131.
- Marsh PD. Are dental diseases examples of ecological catastrophes? Microbiology. 2003;149:279–294.
- Beighton D. Can the ecology of the dental biofilm be beneficially altered? Adv Dent Res. 2009;21:69–73.
- Takahashi N, Nyvad B. The role of bacteria in the caries process: ecological perspectives. J Dent Res. 2011;90:294–303.
- Becker MR, Paster BJ, Leys EJ, et al. Molecular analysis of bacterial species associated with childhood caries. J Clin Microbiol. 2001;40:1001–1009.
- Tong H, Chen W, Merritt J, Qi F, Shi W, Dong X. Streptococcus oligofermentans inhibits Streptococcus mutans through conversion of lactic acid into inhibitory H2O2: a possible counteroffensive strategy for interspecies competition. Mol Microbiol. 2007;63:872–880.
- Shaffer JR, Wang X, Feingold E, et al. Genome-wide association scan for childhood caries implicates novel genes. J Dent Res. 2011;90:1457–1462.
- Shaw L, Murray JJ. A family history study of caries-resistance and caries-susceptibility. Br Dent J. 1980;148:231–235.
- Rupesh S, Nayak UA. Genetic sensitivity to the bitter taste of 6-n propylthiouracil: a new risk determinant for dental caries in children. J Indian Soc Pedod Prev Dent. 2006;24:63–68.
- Wendell S, Wang X, Brown M, et al. Taste genes associated with dental caries. J Dent Res. 2010;89:1198–1202.
- Wright JT. Defining the contribution of genetics in the etiology of dental caries. J Dent Res. 2010;89:1173–1174.
- Johansson I, Holgerson PL, Kressin NR, Nunn ME, Tanner AC. Snacking habits and caries in young children. Caries Res. 2010;44:421–430.
- Lingström P, Birkhed D, Ruben J, Arends J. Effect of frequent consumption of starchy food items on enamel and dentin demineralization and on plaque pH in situ. J Dent Res. 1994;73:652–660.
- O’Mullane D. Can prevention eliminate caries? Adv Dent Res. 1995;9:106–109.
- Levy SM, Warren JJ, Broffitt B, Hillis SL, Kanellis MJ. Fluoride, beverages and dental caries in the primary dentition. Caries Res. 2003;37:157–165.
- Marshall TA, Levy SM, Broffitt B, et al. Dental caries and beverage consumption in young children. Pediatrics. 2003;112:e184–191.
- Declerck D, Leroy R, Martens L, et al. Factors associated with prevalence and severity of caries experience in preschool children. Community Dent Oral Epidemiol. 2008;36:168–178.
- Paes Leme AF, Koo H, Bellato CM, Bedi G, Cury JA. The role of sucrose in cariogenic dental biofilm formation—new insight. J Dent Res. 2006;85:878–887.
- Ly KA, Milgrom P, Rothen M. Xylitol, sweeteners, and dental caries. Pediatr Dent. 2006;28:154–163.
- Söderling EM. Xylitol, mutans streptococci, and dental plaque. Adv Dent Res. 2009;21:74–78.
- Mäkinen KK. Sugar alcohols, caries incidence, and remineralization of caries lesions: a literature review. Int J Dent. 2010;2010:981072.
- Wu CD. Grape products and oral health. J Nutr. 2009;139:1818S–1823S.
- Hu CH, He J, Eckert R, et al. Development and evaluation of a safe and effective sugar-free herbal lollipop that kills cavity-causing bacteria. Int J Oral Sci. 2011;3:13–20.
- Somanah J, Bourdon E, Bahorun T, Aruoma OI. The inhibitory effect of a fermented papaya preparation on growth, hydrophobicity, and acid production of Streptococcus mutans, Streptococcus mitis, and Lactobacillus acidophilus: its implications in oral health improvement of diabetics. Food Sci Nutr. 2013;1:416–421.
- Bonifait L, Grenier D. Cranberry polyphenols: potential benefits for dental caries and periodontal disease. J Can Dent Assoc. 2010;76:130.
- Xu X, Zhou XD, Wu CD. The tea catechin epigallocatechin gallate suppresses cariogenic virulence factors of Streptococcus mutans. Antimicrob Agents Chemother. 2011;55:1229–1236.
- Tanaka K, Miyake Y, Sasaki S. Intake of dairy products and the prevalence of dental caries in young children. J Dent. 2010;38:579–583.
- Shetty V, Hegde AM, Nandan S, Shetty S. Caries protective agents in human milk and bovine milk: an in vitro study. J Clin Pediatr Dent. 2011;35:389–392.
- Merritt J, Qi F, Shi W. Milk helps build strong teeth and promotes oral health. J Calif Dent Assoc. 2006;34:361–366.
- Danielsson Niemi L, Hernell O, Johansson I. Human milk compounds inhibiting adhesion of mutans streptococci to host ligand-coated hydroxyapatite in vitro. Caries Res. 2009;43:171–178.
- Llena C, Forner L. Dietary habits in a child population in relation to caries experience. Caries Res. 2008;42:387–393.
- Näse L, Hatakka K, Savilahti E, et al. Effect of long-term consumption of a probiotic bacterium, Lactobacillus rhamnosus GG, in milk on dental caries and caries risk in children. Caries Res. 2001;35:412–420.
- Cildir SK, Germec D, Sandalli N, et al. Reduction of salivary mutans streptococci in orthodontic patients during daily consumption of yogurt containing probiotic bacteria. Eur J Orthod. 2009;31:407–411.
- World Health Organization. Health and Nutritional Properties of Probiotics in Food Including Powder Milk with Live Lactic Acid Bacteria: Report of a joint FAO/WHO expert consultation on evaluation of health and nutritional properties of probiotics in food including powder milk with live lactic acid bacteria. Available at: who.int/foodsafety/publications/fs_management/en/probiotics.pdf. Accessed July 9, 2014.
- Laleman I, Detailleur V, Slot DE, Slomka V, Quirynen M, Teughels W. Probiotics reduce mutans streptococci counts in humans: a systematic review and meta-analysis. Clin Oral Investig. 2014;18:1539–1552.
- Haukioja A, Söderling E, Tenovuo J. Acid production from sugars and sugar alcohols by probiotic lactobacilli and bifidobacteria in vitro. Caries Res. 2008;42:449–453.
- Slawik S, Staufenbiel I, Schilke R, et al. Probiotics affect the clinical inflammatory parameters of experimental gingivitis in humans. Eur J Clin Nutr. 2011;65:857–863.
- Maltz M, Jardim JJ, Alves LS. Health promotion and dental caries. Braz Oral Res. 2010;24(Suppl 1):18–25.
- Köhler B, Andréen I. Influence of caries-preventive measures in mothers on cariogenic bacteria and caries experience in their children. Arch Oral Biol. 1994;39:907–911.
- Tinanoff N, Palmer CA. Dietary determinants of dental caries and dietary recommendations for preschool children. Refuat Hapeh Vehashinayim. 2003;20:8–23,78.
- Moynihan P, Petersen PE. Diet, nutrition and the prevention of dental diseases. Public Health Nutr. 2004;7:201–226.
- Kressin NR, Nunn ME, Singh H, et al. Pediatric clinicians can help reduce rates of early childhood caries: effects of a practice based intervention. Med Care. 2009;47:1121–1128.
- Bader JD, Rozier RG, Lohr KN, Frame PS. Physicians’ roles in preventing dental caries in preschool children: A summary of the evidence for the U.S. Preventive Services Task Force. Am J Prev Med. 2004;26:315–325.
- American Dietetic Association. Position paper: nutrition and oral health. J Am Diet Assoc. 2003;5:615–625.
A version of this article appeared in the October 2012 issue of Journal of the California Dental Association and is reprinted with permission.
From Dimensions of Dental Hygiene. August 2014;12(8):30–33.
