 FANGXIANUO/E+/GETTY IMAGES PLUS
FANGXIANUO/E+/GETTY IMAGES PLUS
Implementing a Multifaceted Approach to Caries Prevention
To reduce caries prevalence, oral health professionals need to not only use the traditional interventions but also consider adjunctive therapies, behavior modification approaches, and legislative advocacy to improve the oral health of vulnerable populations.
Dental caries is a transmissible bacterial infection whose prevalence and severity are affected by multiple factors. It occurs on a continuum, with cycles of demineralization and remineralization occurring over years. If an incipient caries lesion is detected, or if risk behaviors are identified early, the process may be reversed and the tooth surface repaired. In the United States, caries is more prevalent in Hispanic (46%) and non-Hispanic black (44%) children than in non-Hispanic white children (31%) ages 2 through 8.1,2Globally, out of 7.6 billion people, 2.5 billion have untreated caries in permanent teeth and 573 million children have untreated caries in deciduous teeth.3 Caries development is a dynamic process involving four players: bacteria, fermentable carbohydrates, a tooth, and an extended time period.4,5 The prevailing caries prevention paradigm involves targeting bacteria (antimicrobial agents) and enamel (mainly through the use of fluoride). This approach has had limited success in reducing the worldwide prevalence of caries.6 The next generation of disease prevention, however, must include behaviors and actions outside of those traditionally supported.
Much has been written about the effects of fluoride on the caries process, including public health interventions such as community water fluoridation and various types of professional applications. Despite this, caries remains a significant chronic disease. The startling statistics are presented in Table 1, Table 2, and Table 3.1,2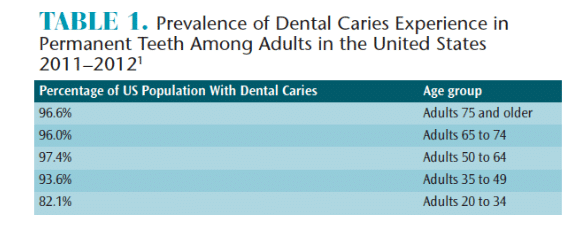
NONFLUORIDE CARIES PREVENTIVE AGENTS
The fact that fluoride effectively prevents, or at least decelerates the caries process is well known.7–10 However, some populations avoid its use due to concerns about the safety of consuming fluoride. As such, to provide culturally competent care to patients who may reject fluoride, oral health professionals should be familiar with nonfluoride caries preventive agents and their effectiveness.
Sodium bicarbonate, or baking soda, has long been used to treat periodontal diseases and dental caries.11–14 It is inexpensive, has high biocompatibility (produces no side effects, has no toxic effects), and is mildly abrasive (2.5 on Moh’s hardness scale and 65 on the radioactive dentin abrasivity test).15 Sodium bicarbonate’s effectiveness as a caries preventive agent is due to its bactericidal properties, effectively killing caries-causing bacteria, such as Streptococcus mutans, and its buffering capacity, raising salivary pH to normal levels after the consumption of carbohydrate-rich foods. Physically, the high solubility of baking soda allows it to penetrate oral biofilms, contributing to the acid-neutralizing effect. Baking soda is mostly used in dentifrices, but studies have also shown its efficacy as an oral rinse and in chewing gum (2% and 4% concentrations).16
Xylitol, a five-carbon sugar alcohol, inhibits bacterial metabolism, increases salivary flow, and reduces transfer of bacteria from mother to child.17–19 While xylitol is a naturally occurring sugar found in many fruits and vegetables, most of the supply used in packaged foods is from sustainable xylan-rich hardwood sources, such as birch and beechwood. A daily dose of 5 g to 6 g of xylitol must be consumed at least three times or more per day in syrups, wipes, gum, dentifrices, lozenges, mouthrinses, or snack foods to be effective.17,18 Some concern exists regarding the choking hazard posed by chewing gum and the American Academy of Pediatrics recommends against it for children younger than 4 and those with chewing or swallowing disorders.20 Nevertheless, xylitol use is supported by the American Academy of Pediatric Dentistry21 (AAPD) for caries prevention in children who have moderate- and high-risk caries risk and by the American Dental Association (ADA) for children who have previously experienced dental caries.19
Other agents that show promise in preventing caries are chlorhexidine, arginine, tricalcium phosphate, amorphous calcium phosphate-casein phosphopeptide (ACP-CPP), triclosan, and iodine. In 2011, the ADA’s Center for Evidence-Based Dentistry published its findings regarding nonfluoride caries preventive agents on the market in the US. A chairside guide is available for clinicians to download at: ebd.ada.org.19 A more recent systematic review did not make any recommendations regarding specific regimens due to the lack of well-controlled studies.22
Occlusal caries constitutes approximately 80% of the caries seen in children up to age 13.23 Application of sealants as soon as the permanent teeth erupt has long been supported but is still underutilized, especially in the populations that need sealants the most. Many erroneously believe their application is limited to children. Sealants can be applied to any deciduous or permanent molar without adverse effects.23,24 Additionally, sealants can be applied to prevent incipient lesions from progressing into larger lesions. According to a recent Cochrane Review, sealants produce an 11% to 51% reduction in occlusal caries compared with no sealant application.24
Although not a prevention agent, silver diamine fluoride (SDF)—a new therapy that arrests cavitated lesions—may significantly reduce the burden of tooth decay in children, adolescents, and patients with special needs. Guidelines recommending the use of 38% SDF to arrest cavitated caries lesions in the primary dentition of these populations were published by the AAPD in 2017.25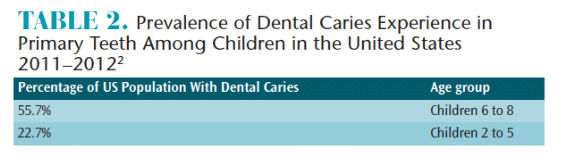
BEHAVIORAL APPROACHES AND RISK ASSESSMENT
Helping improve patients’ health involves more than providing scientific information and performing procedures.26 Applying evidence-based approaches to behavior modification is the best way to empower patients, providing them with the tools they need to change unhealthy habits.
Regarding caries prevention, the main factor that requires intervention is reducing consumption of fermentable carbohydrates. Sugars are either monosaccharides (single-ring) or disaccharides (two or more monosaccharides) and are present naturally in fruits, vegetables, and grains, or added during processing. Sucrose (table sugar) is a disaccharide and the most cariogenic of the sugars because it is fermented by oral bacteria. Added sugars are incorporated into products by the food industry in order to increase shelf life and to enhance taste.27 American children consume, on average, 13.1% to 17.5% of their total daily energy from added sugar (this equates to 19 teaspoons of added sugar daily); 11.2% to 14.5% of American adults’ total daily energy comes from added sugar.28 Reducing an individual’s consumption of free sugars to less than 10% of daily dietary intake will profoundly affect oral and systemic health.28–30 Practicing effective oral hygiene behaviors (eg, biofilm removal) can also help prevent dental caries.
Motivational interviewing (MI) has been the focus of many well-conducted studies that have demonstrated its effectiveness in improving oral health literacy and, consequently, the adoption of healthy habits.31 MI focuses on enhancing the patient’s intrinsic motivation.32 In applying MI, oral health professionals use techniques, such as attentive listening, open-ended questions, and summation, to create a partnership with patients, which is supportive and compassionate. MI also allows patients to analyze the socioeconomic and environmental factors that have the greatest influence on their behaviors.
Caries risk assessment is an evidence-based approach that requires an analysis of the risk factors (habits, behaviors, and environmental contributors to disease), which increase the probability of caries development. Caries management by risk assessment (CAMBRA) provides tools (risk assessment forms for those ages 0 to 5 and 6 to adult) to analyze and address a patient’s risk factors and protective factors.33 Unfortunately, CAMBRA remains underutilized in spite of its proven efficacy in preventing caries and widespread availability.34,35 In 2014, a Current Dental Terminology (CDT) code was created for oral health professionals to bill insurance companies for performing a caries risk assessment (D0601: Caries risk assessment, low risk; D0602: Caries risk assessment, moderate risk; and D0603: Caries risk assessment, high risk).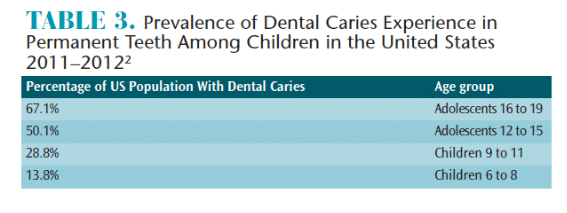
ADVOCACY
Oral health professionals need to also consider advocating through legislative channels to improve oral health. Legislative advocacy involves working with lawmakers and organizations to gain support for a cause. This can take many forms such as lobbying, petition drive, writing letters to politicians, organizing public demonstrations, and digital advocacy (using social media for advocacy).
Oral health has historically received little attention from the federal government with the reason most often cited as lack of available funding. Oral health professionals must get involved if they want to ensure the solvency of such programs as the Children’s Health Insurance Program (CHIP), which covers dental care for children in low-income families.36 The American Dental Hygienists’ Association (ADHA), American Dental Education Association (ADEA), ADA, AAPD, and the Children’s Dental Health Project actively support legislative efforts that seek to improve the nation’s oral health. Information on these efforts, and how to become involved are available by visiting their websites.
- ADHA: adha.org/advocacy
- ADEA: adea.org/state-advocacy-toolkit.aspx
- ADA: ada.org/en/advocacy
- AAPD: aapd.org/advocacy
- Children’s Dental Health Project: cdhp.org
Advocacy requires first and foremost a passion for a cause and a means of communicating that passion. There exists great promise in the use of social media for improving the population’s health literacy and empowerment.37
CONCLUSION
Dental caries continues to be a significant chronic disease, affecting the most vulnerable populations in the US. From an economic perspective, using prevention techniques makes fiscal sense: every dollar invested on measures to prevent oral disease saves the American taxpayer as much as $50 in emergency care for the underserved.26 From an ethical perspective, a disease prevention paradigm (as opposed to a treatment-centered approach) is more closely aligned with the values of the dental hygiene profession. In striving to reduce caries prevalence, dental hygienists should use the primary interventions—fluoride, sealants, and behavior modification approaches—and add adjunctive therapies, as needed. However, public health scholars and agencies have recognized the need for multiple interventions in ensuring the adoption of healthier behaviors in populations.38 For this reason, it is important for oral health professionals to advocate legislatively and understand the effects of socioeconomic status and environment on health behaviors, in addition to remaining aware of alternative caries preventive agents.
REFERENCES
- Dye BA, Thornton-Evans G, Li X, Iafolla T. Dental caries and tooth loss in adults in the United States, 2011–2012. NCHS Data Brief. 2015;197:197.
- Dye BA, Thornton-Evans G, Li X, Iafolla T. Dental caries and sealant prevalence in children and adolescents in the United States, 2011-2012. NCHS Data Brief. 2015;191:1–8.
- Kassebaum NJ, Smith AGC, Bernabé E, et al. Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. J Dent Res. 2017;96:380–387.
- Henry RK, Goldie, MP. Cariology and caries management. In: Gillivan P, ed. Dental Hygiene: Applications to Clinical Practice. Philadelphia: F,A, Davis; 2016.
- Darby M, Walsh M. Dentition assessment. In: Bowen M, ed. Dental Hygiene Theory and Practice. 4th ed. St. Louis. Elsevier Saunders; 2014.
- Lagerweij MD, van Loveren C. Declining caries trends: are we satisfied? Curr Oral Health Rep. 2015;2:212–217.
- Philip A, Sims E, Houston J, Konieczny R. 63 million Americans exposed to unsafe drinking water. USA Today. August 14, 2017.
- The National Academies of Sciences Engineering Medicine. Fluoride in Drinking Water: A Scientific Review of EPA’s Standards. Available at: https://doi.org/10.17226/11571. Accessed April 16, 2018.
- Beltrán-Aguilar ED, Barker L, Dye BA. Prevalence and severity of dental fluorosis in the United States, 1999-2004. NCHS Data Brief. 2010;53:1–8.
- Jiménez-Farfán MD1, Hernández-Guerrero JC, Juárez-López LA, Jacinto-Alemán LF, de la Fuente-Hernández J. Fluoride consumption and its impact on oral health. Int J Environ Res Public Health. 2011;8:148–160.
- Legier-Vargas K, Mundorff-Shrestha SA, Featherstone JDB, Gwinner L. Effects of sodium bicarbonate dentifrices on the levels of cariogenic bacteria in human saliva. Caries Res. 1995;29:143–147.
- Pratten J, Wiecek J, Mordan N, et al. Physical disruption of oral biofilms by sodium bicarbonate: an in vitro study. Int J Dent Hyg. 2016;14:209–214.
- Chandel S, Khan MA, Singh N, Agrawal A, Khare V. The effect of sodium bicarbonate oral rinse on salivary pH and oral microflora: a prospective cohort study. Natl J Maxillofac Surg. 2017;8:106–109.
- Ghassemi A, Vorwerk LM, Hooper WJ, Putt MS, Milleman KR. A four-week clinical study to evaluate and compare the effectiveness of a baking soda dentifrice and an antimicrobial dentifrice in reducing plaque. J Clin Dent. 2008;19:120–126.
- Myneni SR. Effect of baking soda in dentifrices on plaque removal. J Am Dent Assoc. 2017;148:S4–S9.
- Zero DT. Evidence for biofilm acid neutralization by baking soda. J Am Dent Assoc. 2017;48:S10–S14.
- Riley P, Moore D, Ahmed F, Sharif MO, Worthington HV. Xylitol-containing products for preventing dental caries in children and adults. Cochrane Database Syst Rev. 2015;3:CD010743.
- Richards D, Duane B, Sherriff A. Maternal consumption of xylitol for preventing dental decay in children. Available at: cochranelibrary-wiley.com/doi/10.1002/14651858.CD010202/abstract;jsessionid=A121CC3D4630C45CE876F1AA548CF8F6.f02t02. Accessed April 16, 2018.
- Rethman MP, Beltrán-Aguilar ED, Billings RJ, et al. Nonfluoride caries preventive agents. Full report of a systematic review and evidence-based recommendations. J Am Dent Assoc. 2011;142:1065–1071.
- American Academy of Pediatrics. Chewing gum. Available at: aap.org/en-us/about-the-aap/aap-press-room/aap-press-room-media-center/Pages/Chewing-Gum.aspx. Accessed April 16, 2018.
- American Academy of Pediatric Dentistry (AAPD). Policy on the Use of Xylitol. Available at: aapd.org/media/Policies_Guidelines/P_Xylitol.pdf. Accessed April 16, 2018.
- Wang Y, Li J, Sun W, Li H, Cannon RD, Mei L. Effect of non-fluoride agents on the prevention of dental caries in primary dentition: A systematic review. PLoS One. 2017;12:e0182221.
- Papageorgiou SN, Dimitraki D, Kotsanos N, Bekes K, van Waes H. Performance of pit and fissure sealants according to tooth characteristics: A systematic review and meta-analysis. J Dent. 2017;66:8–17.
- Ahovuo-Saloranta A, Forss H, Walsh T, Nordblad A, Mäkelä M, Worthington HV. et al. Pit and fissure sealants for preventing dental decay in permanent teeth. Cochrane Database Syst Rev. 2017;7:CD001830.
- AAPD. Use of Silver Diamine Fluoride for Dental Caries Management in Children and Adolescents, Including Those with Special Health Care Needs. Available at: aapd.org/media/policies_guidelines/ g_sdf.pdf. Accessed April 16, 2018.
- Morad R. Attention on prevention. Scientific American. October 19, 2016. Available at: scientificamerican.com/products/the-future-of-oral-health/attention-on-prevention/?wt.ac=SA_Custom_Colgate_LNDG. Accessed April 16, 2018.
- Moss M. The extraordinary science of addictive junk food. NY Times Magazine. February 20, 2013. Available at: nytimes.com/2013/02/24/magazine/the-extraordinary-science-of-junk-food.html?mcubz=0. Accessed April 16, 2018.
- Marshall T. Nomenclature, characteristics, and dietary intakes of sugars. J Am Dent Assoc. 2015;146:61–64.
- Sheiham Aubrey, James WPT. Diet and dental caries: the pivotal role of free sugars reemphasized. J Dent Res. 2015;94:1341–1347.
- Drewnowski A, Rehm CD. Consumption of added sugars among US children and adults by food purchase location and food source. Am J Clin Nutr. 2014;100:901–907.
- Yevlahova A. Models for individual oral health promotion and their effectiveness: a systematic review. Aust Dent J. 2009; 54:190–197.
- Macri D, Parness J. Strategies for improving patient compliance. Dimensions of Dental Hygiene. 2015;13(12):27–29.
- Young DA, Featherstone JDB, Roth JR. Caries Management By Risk Assessment-A Practitioner’s Guide. J Calif Dent Assoc. 2007;35:678.
- Urban R, Rowe D. Knowledge, attitudes and practices of dental hygienists regarding caries management by risk assessment. J Dent Hyg. 2015;89:55–62.
- Norton W, Funkhouser E, Makhija SK, et al. Concordance between clinical practice and published evidence: findings from The National Dental Practice-Based Research Network. J Am Dent Assoc. 2014;45:22–31.
- American Dental Association. ADA weighs in on ACA repeal. Available at: ada.org/en/publications/ada-news/2017-archive/january/ada-weighs-in-on-aca-repeal. Accessed April 16, 2018.
- Capurro D, Cole K, Echavarría MI, Joe J, Neogi T, Turner AM. The use of social networking sites for public health practice and research: a systematic review. J Med Internet Res. 2014;16:e79.
- Kaplan R, Spittel M, David D, eds. Population health: behavioral and social science insights. Available at: ahrq.gov/professionals/education/curriculum-tools/population-health/index.html. Accessed April 16, 2018.
From Dimensions of Dental Hygiene. May 2018;16(5):21-22, 24-25.

{kind=link}
I follow this author on LinkedIn and she’s always talking about this, not relying on fluoride so much.
[…] parents and caregivers on the multiple factors that influence caries prevalence and severity may provide insights into why some children present with caries, while others don’t. Clinicians […]