 BROTHERS91 / E+ / GETTY IMAGES PLUS
BROTHERS91 / E+ / GETTY IMAGES PLUS
Help Your Patients Achieve a Beautiful Smile
Many options are available to ensure the effectiveness of tooth whitening.
This course was published in the June 2023 issue and expires June 2026. The authors disclose honoraria from Colgate-Palmolive Co. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 780
Educational Objectives
After reading this course, the participant should be able to:
- Discuss the history of tooth whitening.
- Identify the most commonly used methods of tooth whitening.
- Explain a novel in-office whitening treatment method.
Introduction
If you ask patients what they want, many will respond with “I want whiter teeth!” While they may have horrible oral malodor, rampant decay, puffy, bleeding gingiva, and bone loss, often their main concern is a youthful, beautiful, white smile.
The science and chemistry of bleaching or whitening have recently advanced — making it much easier for patients to whiten quickly and comfortably, without messy, oozing gels, trays that pinch, or tooth sensitivity. Colgate® Professional Optic White® In-Office Teeth Whitening Kit is one such option. This whitening kit includes a quick-drying, alcohol-based hydrogen peroxide serum in a brush- tipped pen and a comfortable LED tray. The pen is used to “paint” the hydrogen peroxide precisely on the facial aspects of the enamel, followed by wearing of the tray for just three 10-minute cycles.
This whitening process is much easier for you, too. You can forget the difficulty of sticky gels and gingival barriers — that’s right, NO gingival barrier required. The kit was designed to make it quicker and easier for you while offering no tooth sensitivity as a special added benefit for patients.
Your patients will get what they want: whiter teeth. And you get what you want: a happy patient.
— Phyllis Martina, RDH, MBA, Senior Professional Education Manager, Colgate Oral Pharmaceuticals, Inc.
Boosting the Success of Whitening Techniques
The popularity of tooth whitening has grown exponentially over the past 20 years. While oral health remains the crux of dental care, many patients seek out a dental professional for the hopes of improving the esthetics of their smile. Thus, oral health professionals need to be prepared to offer individualized approaches to patients seeking a whiter, brighter smile, once any oral health issues have been successfully addressed.
Many options are available to help patients achieve the esthetic results they desire. This article reviews the most common methods of tooth whitening as well as provides a close look at a novel in-office whitening approach.
The Beginnings of an Esthetic Smile
The desire for bright white teeth is not a modern phenomenon. The ancient Egyptians mixed pumice with white vinegar to create a bleaching paste.1 As the active ingredient in urine is ammonia, ancient Romans used it to lighten teeth.
In the mid-1800s, full-coverage crowns were implemented to cover discolored dentition. In an effort to develop less invasive solutions, chemicals — such as oxalic acid, chlorine, and even cyanide — were tried; however, their innate toxicity led to the abandonment of these techniques.
In the early 1900s, peroxide was utilized as a treatment for periodontal diseases; both providers and patients noticed whitening was a welcome side effect. As such, peroxide quickly became a popular compound for bleaching due to its efficacy and safety.2
Nightguard vital bleaching, in which carbamide peroxide gel is placed into custom-made trays, was introduced in 1989 by Haywood and Heymann, launching the contemporary at-home whitening trend.3
Components of Stain
When consistently exposed to pigmented substances, dental enamel can become stained. External sources, such as coffee, tea, and tobacco, are well known to cause extrinsic staining. The colored compounds from these substances are known as chromophores. These stains can be absorbed into the tooth or incorporated into calculus and biofilm, especially in difficult-to-clean regions of the dentition.4
Thinning of enamel may also cause tooth discoloration. Enamel is composed of 97% hydroxyapatite, which is naturally white in color. Dentin, however, is only made up of about 70% hydroxyapatite, giving it a yellowish hue.5
The enamel layer of the tooth can be thinned due to the natural aging process or abfraction from toothbrushing, erosion, or other processes. As the enamel layer is thinned, more of the dentin shows through, giving the teeth a yellow hue.
Extrinsic stains attached to the tooth’s surface can be easily removed by abrasives such a brushing with whitening toothpaste or dental prophylaxis; however, once the stain or chromophore has been absorbed into the tooth, whitening products are needed to remove it.
Bleaching Methods
Hydrogen peroxide acts by diffusing into the tooth through the enamel crystals to react with or oxidize chromophores, thus neutralizing the colors. Today, there are three ways to approach bleaching:
- In-office applied under the supervision of an oral health professional
- Professionally dispensed for at-home use
- Over-the-counter products
In-office bleaching is done under the supervision of the clinician and typically involves the use of gels with a high percentage (30% to 40%) of hydrogen peroxide. A light source is often used to accelerate the action of the peroxide.6
The use of high levels of hydrogen peroxide, however, causes side effects. Dentinal and pulpal sensitivities are frequently noted by patients due to the diffusion of the hydrogen peroxide molecules into the pulp chamber, causing changes in pulp connective tissue.7
Gingival tissue irritation and gingival recession caused by direct contact of the gel with gingival tissue are also commonly reported side effects. A gingival barrier should be used to protect the gingival tissue during the in-office application. Rapid bleaching may also cause the enamel to become dehydrated, creating an intense but temporary whitening effect.
Compliance with in-office whitening treatment is high. Treatments are usually completed in 1 to 2 hours. Some methods of in-office whitening require more intensive staff participation due to the need to implement a gingival barrier, administer the material, and assess for the presentation of side effects.
Professionally dispensed at-home whitening is also a safe and effective option. With this technique, the clinician fabricates a bleaching tray, which is made to fit perfectly over patient’s teeth in order to avoid direct contact of gingival tissues with the bleaching gel.
Professionally dispensed tray whitening uses less potent gels typically 10% to 22% carbamide peroxide or 4% to 10% hydrogen peroxide. In the presence of water, carbamide peroxide breaks down to release about 3.5% hydrogen peroxide.8 Therefore, professionally dispensed at-home bleaching must be applied nightly for 2 to 4 weeks.
The most common problem with the take home option is consistent use. Compliance with the daily use of gels and trays is problematic in some patients. In addition, resultant sensitivity also hinders this technique’s efficacy. Patients frequently overfill the trays with bleaching material, which increases the risk for sensitivity and gingival irritation.
Over-the-counter bleaching products have become increasingly popular due to ease of accessibility and low cost.9 These whitening products come in many different forms including whitening pens, strips, gels, and universal trays. Over-the-counter methods are effective in obtaining results similar to at-home bleaching, however, oral tissues are usually not protected from contact with peroxide.
Compliance is an issue, particulary when patients experience side effects. When consistent application falls off, results can vary with little to no improvement seen in tooth color.
Factors Impacting Results
Whitening results are impacted by concentration of the agent and the time the agent is active on the surface of the tooth. In order to reach the highest level of whitening, the concentration or the amount of time the active agent is applied must be high, which increases the potential for undesirable side effects.
Novel Whitening Technique
A new method of in-office tooth whitening has been introduced that doesn’t require the same levels of exposure or application time. This technique uses a brush to apply a whitening serum that is activated by a 410-nm LED ultraviolet light. The light is designed to boost the energy applied to the serum, directly affecting pigmented molecules.10 Noticeable results are seen after three applications for 10 minutes.

The pen delivery system allows for an easy and controlled application (Figure 1). The serum is applied with a brush and the carrier liquid quickly evaporates, leaving the whitening agent concentrated and stable on the surface of the tooth. The peroxide does not smear with simple movements of the lips or tongue or upon contact with saliva. Because only the concentrated form of the agent is left on the tooth, the risk of excess exposure to the active ingredient is reduced.11
The new system comes in a kit that includes lip retractors, light tray, charging cord and station, 10% hydrogen peroxide serum pen, and a 100% ethanol pen to reconstitute and remove the film following each 10-minute session. The trays should be fully charged prior to patient treatment. Once fully charged, the tray should last for four to five 10-minute sessions. Clinicians may want to show patients their current shade with a shade guide so a comparison can be made at the end of the session.
The retractors are placed in the patient’s mouth after the pen has been clicked to begin expressing the serum. The serum should be brushed on in a gentle one- or two-stroke fashion from the gingiva to the direction of the incisal edge.
The pen normally requires one to two clicks between each tooth. Application is obvious as evaporation of the carrier leaves a thick white film on the tooth surface. If the pen tip mixes with saliva, the bristles may need to be wiped off so the serum expressed is fresh and uncontaminated. Clinicians need not cover the entire tooth surface; once the serum is applied, the peroxides will penetrate the enamel and spread laterally throughout the dentin.
The LED light tray is then applied. The tray has a built-in timer that beeps at 5 minutes to signify the halfway point and then beeps again at 10 minutes at which point the light will shut off. It may be easier to insert the tray with the lip retractor still in place and remove the retractors after the tray is fully seated.
Once the timer has indicated the end of 10 minutes, the old film is removed and the serum is reapplied for three different sessions of 10 minutes each. This is easily accomplished with the ethanol pen, cotton tip applicators, or gauze, or even allowing the patient to just brush with water. The old peroxide must be removed from the tooth surface in order to prevent the second and third applications from absorbing into the enamel.
The new in-office bleaching kit eliminates the need for applying gingival barriers, saving time. The compact light also eliminates the need for bulky storage. The reusable tray can be given to the patient on the day of treatment, preventing the need for expensive custom tray fabrication.
At-home maintenance pens are sold through the dental office. This home booster/maintenance pen can be used in combination with the tray. It is safe enough to be left on the teeth overnight and brushed off in the morning during the daily oral hygiene regimen.
In a study of 80 subjects, Paravina et al12 found that the use of this pen bleaching system provided an average of six shades of improvement using the Vita Bleachguide 3-D Master shade guide. The 39 subjects in the treatment group began the study with an average pretreatment shade of 17.69 and finished at an average of 11.70, demonstrating a six-shade improvement. The placebo group started at 18.22 and completed at an average of 18.15. No side effects were reported and a call 24 hours later to capture any delayed reactions did not find any adverse events.
Case Presentation
This patient had tried whitening in the past and was hesitant due to the severe tooth sensitivity she experienced as a result. After observing this kit being used on another person, she was motivated to try in-office whitening again.
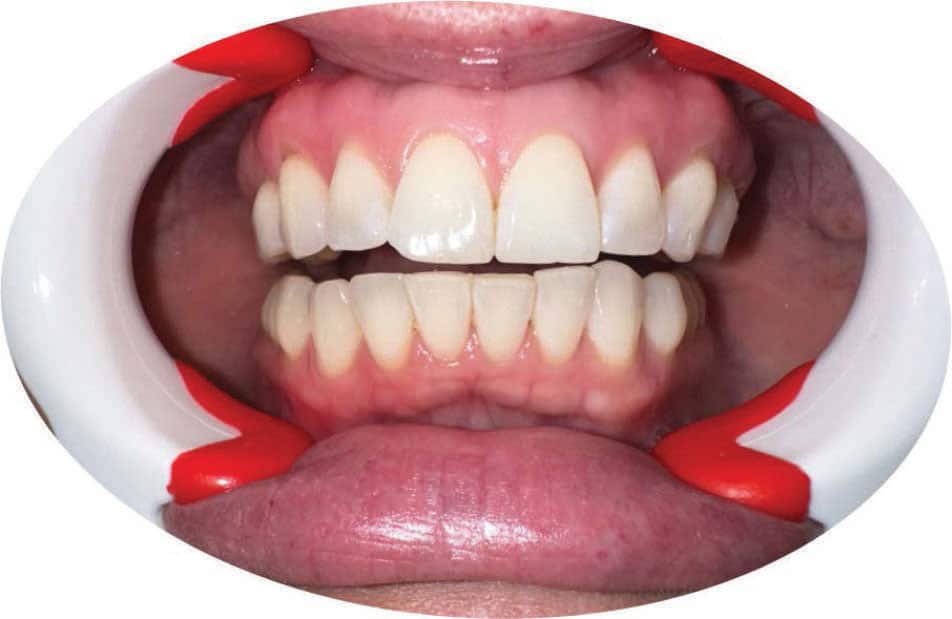
As seen in Figure 2, the retractors are applied and the teeth are dried. Figure 3 depicts delivery of the serum using the pen applicator. Once the serum carrier has evaporated, the solid peroxide (10%) is left remaining on the tooth’s surface. The tray is then inserted. It can be easier to insert the tray while the retractors are still in the mouth.

The patient then closes her mouth and the LED light is activated with the button on the handle (Figure 4). Following the 10-minute treatment time, the tray is removed, the retractors are replaced, and the 100% ethanol alcohol pen is applied to reconstitute the peroxide matrix into a liquid. The liquid is gently wiped away with a cotton tip applicator or similarly absorbent material (Figure 5).

The final shade improvement is seen in Figure 6. This patient demonstrated a five-shade improvement using the Vita Bleachguide shade guide. She was pleased with the results and reported no sensitivity or burning of her gingiva. The patient rinsed with cold water and reported the cold sensation as normal. She also stated how the whitening effect looked natural and did not look “bleached.”

This technology has a very low incidence of side effects while still able to achieve results comparable to other methods.

Conclusion
Supporting patients in achieving a beautiful smile is an important part of providing excellent oral healthcare. With many options available — from in-office to professionally dispensed to over-the-counter — oral health professionals are charged with helping patients sort through the options. The addition of the bleaching pen-based model provides more options for patients and its use may help reduce the risk of side effects while providing effective results.
References
- Boitsaniuk S, Kochan O, Levkiv M. Modern concepts of teeth whitening — a narrative review. EUREKA: Health Sciences. no. 2022;6:31–43.
- Kwon SR, Wertz PW. Review of the mechanism of tooth whitening. J Esthet Restor Dent. 2015;27:240–257.
- Haywood H, Heymann H. Nightguard vital bleaching. Quintessence Int. 1989;20:173–176.
- Rodríguez‐Martínez J, Valiente M, Sánchez-Martín MJ. Tooth whitening: From the established treatments to novel approaches to prevent side effects. J Esthet Restor Dent. 2019;31:431–440.
- Epple M, Meyer F, Enax J. A critical review of modern concepts for teeth whitening. Dent J (Basel). 2019;7:79.
- Kugel G, Ferreira S, Sharma S, Barker ML, Gerlach RW. Clinical trial assessing light enhancement of in-office tooth whitening. J Esthet Restor Dent. 2009;21:336-
- Kwon SR. Introduction to tooth whitening. Available at: lomalinda.elsevierpure.com/en/publications/introduction-to-tooth-whitening-2. Accessed May 8, 2023.347.
- Kielbassa AM, Maier M, Gieren AK, Eliav E. Tooth sensitivity during and after vital tooth bleaching: A systematic review on an unsolved problem. Quintessence Int. 2015;46:881–897.
- Dahl JE, Pallesen U. Tooth bleaching — a critical review of the biological aspects. Crit Rev Oral Biol Med. 2003;4:292–304.
- Silva Daltro TW, Gomes de Almeida SA, Dias MF, Lins-Filho PC, Vicente da Silva CH, Guimarães RP. The influence of violet led light on tooth bleaching protocols: in vitro study of bleaching effectiveness. Photodiagnosis Photodyn Ther. 2020;32:102052.
- Robo I, Heta S, Spiro K, Ostreni V. Topic: complications and side effects of dental whitening procedures. Available at: researchsquare.com/article/rs-1365431/v1. Accessed May 8, 2023.
- Paravina RD, Johnston WM, Powers JM.New shade guide for evaluation of tooth whitening—colorimetric study. J Esthet Restor Dent. 2007;19:276–283.
THIS TWO-UNIT CE COURSE IS SUPPORTED THROUGH AN UNRESTRICTED EDUCATIONAL GRANT FROM COLGATE.
From Dimensions of Dental Hygiene. June 2023; 21(6):25-29.
