
Fluoride’s Role in Caries Prevention
While fluoride is key to preventing tooth decay, aspects of its usage can greatly affect efficacy.
Fluoride is the most effective strategy against dental caries. Its regular use is recommended by most prominent health organizations, including the American Dental Association (ADA), United States Food and Drug Administration (FDA), Environmental Product Declarations, International Association for Dental Research, American Academy of Pediatric Dentistry, American Medical Association, and Centers for Disease Control and Prevention (CDC). In fact, community water fluoridation has been called one of the 10 greatest public health accomplishments of the 20th century,1 and the widespread use of fluoride toothpaste is considered responsible for the decline in caries prevalence in both developed and developing countries.
It was thought that fluoride ingested systemically during tooth formation would lead to better mineralized structure and, consequently, greater resistance to dental caries; however, numerous studies have shown that this effect is small and probably limited to pits and fissures.2 Fluoride offers the greatest benefits when applied topically after tooth eruption by affecting demineralization and remineralization episodes occurring between tooth structure and dental plaque.3 This topical, post-eruptive effect can provide benefits throughout the lifespan. Laboratory studies have shown that fluoride may be bactericidal or bacteriostatic. The concentration needed to exert this effect, however, is relatively high and unlikely to occur frequently in vivo.4
Numerous systematic reviews have shown that fluoride delivered by various methods is effective against caries.5–10 Today, a wide variety of commercially available fluoride products with varying concentrations are available that present an array of advantages and limitations (Figure 1). This review includes the most common fluoride products commercially available in the US and provides a discussion on how to enhance their efficacy and minimize side effects.
In addition to community fluoridated water, which is available to approximately 75% of the US population, fluoride products are available in self-applied and professionally applied versions.
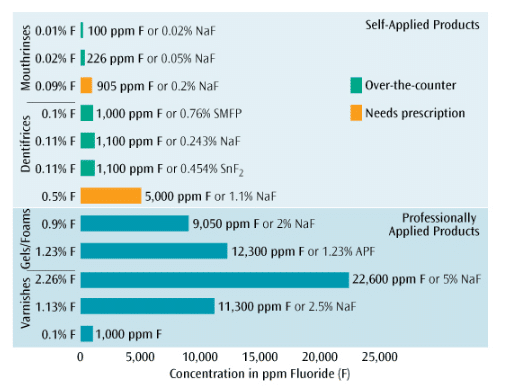
SELF-APPLIED PRODUCTS
Self-applied products include dentifrices, mouthrinses, and supplements. Dentifrices, or toothpastes, are the most available and widely used oral health care product in the US and in most countries.11 Strong evidence has shown that brushing with fluoride dentifrice is effective in reducing caries in children and adolescents.5 Therefore, toothbrushing with fluoride dentifrice is the most important and efficient strategy to control caries.12
Several factors are associated with the effectiveness of dentifrice.11 In the US, most dentifrices contain sodium fluoride (NaF) as the active ingredient, while other toothpastes use either stannous fluoride (SnF2) or sodium monofluorophosphate. SnF2-containing dentifrices potentially reduce biofilm formation while they deliver fluoride.13 Dentifrice formulation is complex, and incorrectly formulated or poorly manufactured products can have reduced anti-caries efficacy.14 Quality standards for toothpaste fabrication are regulated by the FDA and the International Organization for Standardization to ensure adequate levels of efficacy and safety. Additionally, manufacturers may go through a rigorous vetting process to receive the ADA Seal of Acceptance.
A recent systematic review demonstrated that dentifrices need at least 1,000 ppm of fluoride to be effective;5 most dentifrices in the US contain 1,100 ppm of fluoride. High-fluoride prescription dentifrices (5,000 ppm) are indicated for patients at increased risk of caries, particularly root caries, because significantly higher amounts of fluoride are needed to prevent or arrest root caries lesions compared to enamel lesions.15 Clinical studies have shown prescription dentifrices’ efficacy in children at high-caries risk16 and older adults.17,18
Patients’ behavior during and after toothbrushing directly affects dentifrice efficacy.11 Dentifrice quantity, brushing frequency, brushing time, and rinsing are important determinants for fluoride retention in the oral cavity and resulting caries control.19 The general recommendation is to brush teeth at least twice per day, with one of the brushing periods occurring just before bedtime to extend the fluoride action period. A longer brushing time increases fluoride concentrations in saliva and plaque.19 Thorough rinsing with a large quantity of water, however, reduces fluoride retention11,20 and therefore should be discouraged for patients at high-caries risk. The following options can be suggested: spit without rinsing, rinse with a very small amount of water mixed with the dentifrice remaining in the mouth, or rinse with a fluoride mouthrinse11 (only for patients using over-the-counter fluoride dentifrices).

* Store securely to avoid accidental ingestion by children
Recommendations are in agreement with the American Dental Association Guide for Toothpaste Use for Young Children24 and Topical Fluorides Use25
Dentifrice ingestion by children may be associated with an increased risk of dental fluorosis,21 although it is usually mild and does not interfere with quality of life.12,22 To minimize dentifrice swallowing, toothbrushing in children should be supervised or performed by an adult, using a smaller amount of dentifrice (Table 1).23,24
The regular use of fluoride mouthrinses has been associated with a reduction in caries prevalence among children.10 Mouthrinses are currently indicated only for patients at increased caries risk older than 6. Over-the-counter mouthrinses (100 ppm or 226 ppm fluoride) are recommended for use once or twice per day. High-concentration prescription rinses (905 ppm fluoride) also are available and can be recommended for daily or weekly use.25 The frequency of use for any mouthrinse should be customized to the patient’s needs and should not be implemented by those who are using prescription dentifrice (5,000 ppm fluoride). When used after brushing, fluoride-free mouthrinses have the potential to reduce the anti-caries efficacy of fluoride dentifrices.11 Conversely, patients at increased caries risk who use fluoride-free mouthrinses regularly should be advised to increase their fluoride exposure by replacing fluoride-free mouthrinse with a fluoride-containing mouthrinse.
Dietary fluoride supplements, such as tablets, drops, or lozenges, were first introduced to provide systemic fluoride in areas where water fluoridation was not available.26 Currently, supplements are recommended for children age 6 months to 16 years who live in areas with low fluoride levels in the community water supply (<0.3 ppm) and who are at increased risk of tooth decay.27 The recommended daily dose is 0.25 mg of fluoride for children 6 months to 3; 0.5 mg for children 3 to 6; and 1 mg for children 6 to 16.27 A recent systematic review26 found that the use of fluoride supplements is associated with a reduction in caries incidence in permanent teeth when compared to patients who received no fluoride supplement (effect is unclear on deciduous teeth). When compared to topical fluoride administration, however, this beneficial effect is lost.
PROFESSIONALLY APPLIED PRODUCTS
Fluoride also can be applied in the dental office on patients with increased caries risk to complement their self-applied fluoride regimen or to compensate for a lack of compliance. Professionally applied products are also recommended for patients with disabilities that limit motor coordination, those who are immunocompromised, and individuals with significantly low salivary flow. The goal is to form reservoirs of fluoride-like precipitations that can release fluoride into saliva or plaque when the pH drops on dental plaque and oral surfaces. These professionally applied products do not increase fluorosis risk, probably due to the long duration between applications.28 They are typically applied two times to four times per year, depending on the patient’s needs.25
Numerous studies have demonstrated the efficacy of fluoride gels and varnishes in reducing caries incidence.6,9 Fluoride foams may exhibit similar efficacy to gels, but few clinical studies have evaluated them.29 Concerns about their efficacy exist, as the concentration of fluoride per area of covered tooth surface is reduced.25
Gels and foams are available in two fluoride formulations: 1.23% acidulated phosphate fluoride (APF) containing 12,300 ppm fluoride and neutral 2% NaF containing 9,050 ppm fluoride. Most efficacy studies have been conducted using APF; however, this formulation can damage tooth-colored restorations due to its low pH (~3.5). For patients with these types of restorations, neutral gel is indicated. While many gels and foams are marketed for 1-minute application based on in vitro/in situ data,30 the current recommendation based on clinical trials6 is for a 4-minute application. Gel/foam applications are indicated only for individuals at increased caries risk who are older than 6 due to potential risk of acute toxicity. For younger children, fluoride varnish is recommended.
Fluoride varnish is becoming the most commonly used fluoride product in dental offices because of the evidence supporting its efficacy,9 ease of use, patient acceptance, application time, and safety. It is recommended for individuals of all ages with increased caries risk. Most fluoride varnishes contain 22,600 ppm fluoride in a resin carrier. Some have other potentially beneficial ingredients, including calcium phosphate technologies, but supporting clinical evidence is not yet available.
Experts have suggested that prophy-cup prophylaxis or professional toothbrushing before the application of gels/foams or varnishes might not provide additional efficacy benefit;25 however, it might be desirable for patients with poor oral hygiene. Most varnishes need to be applied to dry enamel/dentin surfaces.
Recurrent caries, a common problem in high-risk patients, could potentially be reduced by the use of fluoride-releasing restorative materials. Glass-ionomers and their resin-modified varieties are able to affect bacterial metabolism under simulated cariogenic conditions in vitro.31 In other laboratory and in situ studies, these materials have been shown to increase fluoride concentration in the local environment, protecting against caries around recently placed restorations (short-term studies). Clinical studies have not shown consistent results of this caries-inhibiting benefit.31 Because of this, relying solely on the preventive properties of these materials is not recommended and other fluoride sources should be included in the caries management strategy.
CONCLUSION
Fluoride is effective in preventing caries lesions and even reversing incipient lesions. However, it does not eliminate the causal factors of dental caries. As such, fluoride should be used as part of a comprehensive caries-management strategy. Fluoridated water and dentifrices are indicated for all ages. Toothbrushing with fluoride dentifrice is considered the most efficient and important strategy against dental caries. Professionally applied and prescription fluoride products are indicated only for patients at increased risk. Lastly, fluoride therapy should be adjusted consistently based on individual patient factors.
REFERENCES
- Centers for Disease Control and Prevention. Ten great public health achievements—United States, 1900-1999. MMWR Morb Mortal Wkly Rep. 1999;48:241–243.
- Singh KA, Spencer AJ, Brennan DS. Effects of water fluoride exposure at crown completion and maturation on caries of permanent first molars. Caries Res. 2007;41:34–42.
- ten Cate JM. Current concepts on the theories of the mechanism of action of fluoride. Acta Odontol Scand. 1999;57:325–329.
- Bradshaw DJ, Marsh PD, Hodgson RJ, Visser JM. Effects of glucose and fluoride on competition and metabolism within in vitro dental bacterial communities and biofilms. Caries Res. 2002;36:81–86.
- Walsh T, Worthington HV, Glenny AM, Appelbe P, Marinho VC, Shi X. Fluoride toothpastes of different concentrations for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2010;1:CD007868.
- Marinho VC, Higgins JP, Logan S, Sheiham A. Fluoride gels for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2002;2:CD002280.
- Marinho VC, Higgins JP, Logan S, Sheiham A. Topical fluoride (toothpastes, mouthrinses, gels or varnishes) for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003;4:CD002782.
- Marinho VC, Higgins JP, Sheiham A, Logan S. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003;1:CD002278.
- Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2013;7:CD002279.
- Marinho VC, Higgins JP, Logan S, Sheiham A. Fluoride mouthrinses for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003;3:CD002284.
- Parnell C, O’Mullane D. After-brush rinsing protocols, frequency of toothpaste use: fluoride and other active ingredients. Monogr Oral Sci. 2013;23:140–153.
- Cury JA, Tenuta LM. Evidence-based recommendation on toothpaste use. Braz Oral Res. 2014;28:1–7.
- Makin SA. Stannous fluoride dentifrices. Am J Dent. 2013;26:3A–9A.
- Lippert F. An introduction to toothpaste—its purpose, history and ingredients. Monogr Oral Sci. 2013;23:1–14.
- Petersson LG. The role of fluoride in the preventive management of dentin hypersensitivity and root caries. Clin Oral Investig. 2013;17(Suppl 1):S63–S71.
- Nordstrom A, Birkhed D. Preventive effect of high-fluoride dentifrice (5,000 ppm) in caries-active adolescents: a 2-year clinical trial. Caries Res. 2010;44:323–331.
- Baysan A, Lynch E, Ellwood R, Davies R, Petersson L, Borsboom P. Reversal of primary root caries using dentifrices containing 5,000 and 1,100 ppm fluoride. Caries Res. 2001;35:41–46.
- Ekstrand KR, Poulsen JE, Hede B, Twetman S, Qvist V, Ellwood RP. A randomized clinical trial of the anti-caries efficacy of 5,000 compared to 1,450 ppm fluoridated toothpaste on root caries lesions in elderly disabled nursing home residents. Caries Res. 2013;47:391–398.
- Zero DT, Creeth JE, Bosma ML, et al. The effect of brushing time and dentifrice quantity on fluoride delivery in vivo and enamel surface microhardness in situ. Caries Res. 2010;44:90–100.
- Duckworth RM. Pharmacokinetics in the oral cavity: fluoride and other active ingredients. Monogr Oral Sci. 2013;23:125–139.
- Wong MC, Clarkson J, Glenny AM, et al. Cochrane reviews on the benefits/risks of fluoride toothpastes. J Dent Res.2011;90:573–579.
- Chankanka O, Levy SM, Warren JJ, Chalmers JM. A literature review of aesthetic perceptions of dental fluorosis and relationships with psychosocial aspects/oral health-related quality of life. Community Dent Oral Epidemiol. 2010;38:97–109.
- Ellwood RP, Cury JA. How much toothpaste should a child under the age of 6 years use? Eur Arch Paediatr Dent. 2009;10:168–74.
- Fluoride toothpaste use for young children. J Am Dent Assoc. 2014;145:190–191.
- Weyant RJ, Tracy SL, Anselmo TT, et al. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013;144:1279–1291.
- Tubert-Jeannin S, Auclair C, Amsallem E, et al. Fluoride supplements (tablets, drops, lozenges or chewing gums) for preventing dental caries in children. Cochrane Database Syst Rev. 2011;12:CD007592.
- Rozier RG, Adair S, Graham F, et al. Evidence-based clinical recommendations on the prescription of dietary fluoride supplements for caries prevention: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2010;141:1480–1489.
- Wong MC, Glenny AM, Tsang BW, Lo EC, Worthington HV, Marinho VC. Topical fluoride as a cause of dental fluorosis in children. Cochrane Database Syst Rev. 2010;1:CD007693.
- Jiang H, Bian Z, Tai BJ, Du MQ, Peng B. The effect of a bi-annual professional application of APF foam on dental caries increment in primary teeth: 24-month clinical trial. J Dent Res. 2005;84:265–268.
- Calvo AF, Tabchoury CP, Del Bel Cury AA, Tenuta LM, da Silva WJ, Cury JA. Effect of acidulated phosphate fluoride gel application time on enamel demineralization of deciduous and permanent teeth. Caries Res. 2012;46:31–37.
- Wiegand A, Buchalla W, Attin T. Review on fluoride-releasing restorative materials—fluoride release and uptake characteristics, antibacterial activity and influence on caries formation. Dent Mater. 2007;23:343–362.
From Dimensions of Dental Hygiene. March 2015;13(3):18,20,22,24-25

{kind=link}