Diabetes Care Strategies
Oral health professionals need to remain up-to-date on best practices for treating patients with diabetes.
This course was published in the May 2014 issue and expires May 31, 2017. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the severity of diabetes mellitus nationally and globally.
- Discuss the signs, symptoms, and risk factors for diabetes.
- Explain the new guidelines and recommendations for treating patients with diabetes.
- Use best clinical practices when providing dental hygiene care for individuals with diabetes.
Diabetes mellitus is a chronic endocrine disorder characterized by an inability of the pancreas to produce enough insulin, the body’s inability to effectively use the insulin produced by the pancreas, or both. Worldwide, this disease affects 382 million people1 and is considered an epidemic. The drastic growth in prevalence is largely due to increases in weight and physical inactivity.2 By 2030, diabetes is projected to become the seventh leading cause of death, with total deaths expected to rise more than 50% over the next 10 years.2
There are four main types of diabetes: type 1, type 2, specific types of diabetes due to other causes, and gestational diabetes. Type 1 accounts for approximately 5% of adult cases and is characterized by deficient insulin production to the extent that daily administration of insulin is required. Type 2 occurs in 90% to 95% of all diagnosed cases of diabetes in adults, and is caused by a combination of insulin resistance and an inadequate compensatory insulin secretory response. Type 2 diabetes is largely associated with excess body weight and physical inactivity, and is becoming more common in children and adolescents.3,4
Other types of diabetes are caused by genetic defects in ?-cell function, genetic defects in insulin action, illness or medications that lead to the destruction of pancreatic beta cells, or the development of peripheral insulin resistance. Diseases that are associated with this type of diabetes include pancreatitis, Cushing’s syndrome, acromegaly, and cystic fibrosis. Associated medications include phenytoin, glucocorticoids, estrogens, and anti-rejection medications for organ transplants.5
Gestational diabetes refers to any degree of glucose intolerance with onset occurring during pregnancy. This type occurs in 2% to 10% of pregnancies4 and places both mother and child at risk for developing diabetes within 10 years to 20 years.
HEALTH CONSEQUENCES
There are numerous systemic health consequences of diabetes. Diabetes increases the risk of heart disease and stroke. Neuropathy, combined with reduced blood flow, increases the chances of foot ulcers, infections, and amputations (Figure 1). Long-term accumulated damage to the small blood vessels in the retina leads to diabetic retinopathy and blindness. Further, diabetes is the leading cause of end-stage renal disease and the need for kidney transplants.3 Associated with increased risk of cancers of the liver, pancreas, endometrium, colon/rectum, breast, and bladder, diabetes is also a risk factor for cognitive decline and dementia.6–8
RISK FACTORS
Multiple risk factors are associated with type 2 diabetes, including: family history of diabetes; overweight/obesity; unhealthy diet; physical inactivity; increasing age (age 45 and older); cardiovascular disease (CVD), hypertension, and dyslipidemia; ethnicity (African American, Alaska Native, American Indian, Asian American, Hispanic/Latino, or Pacific Islander); history of impaired glucose tolerance or prediabetes; history of gestational diabetes, history of giving birth to at least one baby weighing more than 9 pounds, and poor nutrition during pregnancy; polycystic ovary syndrome; acanthosis nigricans; and untreated sleep problems.9,10 The more risk factors, the higher the risk of type 2 diabetes.
SIGNS AND SYMPTOMS
Signs and symptoms of diabetes vary. In some cases, an individual may not experience any indicators of the disease. Commonly experienced signs include: frequent urination (polyuria), excessive thirst (polydipsia), increased hunger, unexplained weight loss, fatigue, lack of interest and difficulty with concentration, tingling or numbness sensations in the hands and feet, blurred vision, frequent infections, slow-healing wounds, sexual dysfunction, and gastroparesis.9,11 Signs occur rapidly and dramatically in type 1 diabetes; however, symptoms can be mild or absent with individuals developing type 2 diabetes, making it more difficult to detect.
DIAGNOSING DIABETES
Diagnosing diabetes occurs through blood assays, including the random plasma glucose, fasting plasma glucose, oral glucose tolerance test, and the glycated hemoglobin A1c (HbA1c or A1c) test. A1c is widely used as a marker of chronic glycemia, demonstrating average blood glucose levels over a 2-month to 3-month period. This test is critical in the management of individuals with diabetes as it correlates well with both microvascular and macrovascular complications. Testing results for the diagnosis of diabetes should be repeated (using the same blood test) to rule out laboratory error.12
PREVENTION AND CONTROL
Although diabetes is a serious health condition, studies have demonstrated that it can be prevented and controlled.13–16 Lifestyle changes, regular physical activity, smoking cessation, taking prescribed medications, eating a balanced diet, reaching and maintaining a reasonable body weight, taking vitamin D supplements, and improved sleep patterns are recommended.9,17 Early intervention with an interdisciplinary health care team that provides continuous, proactive, planned, patient-centered, and population-based care is appropriate.18
Within the past year, new guidelines and recommendations for the management of diabetes have been published. Medical guidelines from the American Diabetes Association and the American Association of Clinical Endocrinologists have been presented in addition to a consensus report concerning diabetes and periodontal diseases.
AMERICAN DIABETES ASSOCIATION GUIDELINES
The American Diabetes Association guidelines, “Standards in Medical Care in Diabetes—2013,”19 describe multiple aspects for testing, screening, preventing, monitoring, and managing diabetes. Dental hygienists can incorporate the recommendations described below as part of their assessment practices and preventive education programs.
In addition to the current criteria for the diagnosis of diabetes, the American Diabetes Association recommends testing to detect type 2 diabetes and prediabetes in asymptomatic individuals of any age who are overweight or obese (BMI ?25 kg/m2) and who have one or more risk factors for diabetes. Repeat testing should be performed every 3 years if tests are normal. Testing to detect type 2 diabetes and prediabetes is recommended for children and adolescents who are overweight and have two or more additional risk factors for diabetes.
Annual glucose testing is suggested for those with prediabetes, as is screening for and the treatment of modifiable risk factors for CVD. The American Diabetes Association recommends performing an A1c test at least twice per year for patients who are meeting treatment goals and have stable glycemic control. Quarterly A1c testing is recommended for those whose therapy has changed or who are not meeting glycemic goals.
Other tests are recommended to assess for systemic complications, including an annual test to analyze urine albumin and serum creatinine, and an initial dilated and comprehensive eye exam within 5 years of onset of diabetes with subsequent annual examinations performed by an ophthalmologist or optometrist. Individuals with diabetes should be screened for distal symmetric polyneuropathy at initial diagnosis of type 2 and 5 years after the diagnosis of type 1, and at least annually thereafter. A yearly comprehensive foot exam is recommended to identify risk factors predictive of ulcers and amputations.
An effective ongoing support program that targets weight loss of 7% of body weight and increases physical activity to at least 150 minutes/week of moderate activity, such as walking, is key for individuals with prediabetes. Adults with diabetes should be advised to engage in the same level of physical activity and encouraged to perform resistance training at least twice per week.
Self-monitoring of blood glucose is recommended for patients on multiple-dose insulin or insulin pump therapy at regular intervals, such as prior to meals and snacks, post-prandially, at bedtime, prior to exercise, and before performing critical tasks, such as driving.
A regimen of metformin—a biguanide type of drug used to treat type 2 diabetes—should be considered for those with prediabetes, obese individuals, at-risk individuals younger than 60, and women with prior gestational diabetes. If this treatment does not achieve or maintain the A1c target over 3 months to 6 months, a second oral agent should be added. For those with markedly symptomatic and/or elevated blood glucose levels or A1c, insulin therapy should be considered from the outset. Further, individuals who have been diagnosed with prediabetes or diabetes should receive individualized medical nutrition therapy to achieve treatment goals. Bariatric surgery may be considered for adults with BMI ?35 kg/m2 and type 2 diabetes, especially if the diabetes or comorbidities are difficult to control.
Blood pressure should be measured at every visit. Those with hypertension should be treated to a systolic goal of <140 mm Hg and a diastolic goal of <80 mm Hg. A fasting lipid profile should be measured annually. Statin therapy should be added to lifestyle therapy, regardless of baseline lipid levels. Further, aspirin therapy (72 mg to 162 mg/day) should be considered as a primary prevention strategy for those with diabetes at increased CVD risk. Smoking cessation should be a routine part of diabetes care.
Individuals with diabetes at risk for hypoglycemia should be asked about symptoms at each encounter. The preferred treatment for the conscious patient with hypoglycemia is glucose (15 g to 20 g). Glucagon should be prescribed for those individuals at a significant risk of severe hypoglycemia.
All patients with diabetes who are older than 6 months should receive an annual influenza vaccine. A pneumococcal vaccine is recommended for those age 2 and older. A revaccination is recommended for those older than 64 who were previously immunized more than 5 years prior. The hepatitis B vaccine is also recommended.
RECOMMENDATIONS OF THE AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS
In 2013, the American Association of Clinical Endocrinologists published a comprehensive diabetes management algorithm and principles for the management of type 2 diabetes.20 This document provides models for evaluating overweight and obese individuals; a prediabetes algorithm that addresses lifestyle modifications of CVD risk factors, anti-obesity therapies, and antihyperglycemic therapies; a glycemic control algorithm that describes monotherapy, dual therapy, and triple therapy medication management; an algorithm for adding/intensifying insulin; and a CVD risk factor modification algorithm that addresses therapeutic lifestyle changes and management of dyslipidemia and hypertension.
The principles of the American Association of Clinical Endocrinologists algorithm for the treatment of type 2 diabetes include the following recommendations:20
- Lifestyle optimization is essential and should engage the entire diabetes team
- A1c target must be individualized based on age, comorbidity, duration of diabetes, risk of hypoglycemia, patient motivation and adherence, life expectancy, etc; an A1c of 6.5% or less is considered optimal
- Blood glucose monitoring is key
- Choice of therapies must be individualized and include complementary mechanisms of action for optimum glycemic control
- Minimizing the risk of hypoglycemia and weight gain is a priority
- Effectiveness of therapy must be evaluated frequently (every 3 months) until stable
- Safety and efficacy should be given higher priorities than initial cost of medications
As part of the health care team, dental hygienists can reinforce these recommendations by working together with patients and their medical practitioners to promote improved health.
PERIODONTAL-DIABETES GUIDELINES
In 2013, Chapple and Genco21 summarized a consensus report on behalf of a joint working group of the European Federation of Periodontology and the American Academy of Periodontology. This group reviewed epidemiological evidence from multiple studies examining the impact of periodontal diseases on diabetes incidence, control, and complications. The working group noted that consistent and robust evidence has emerged over the past 20 years demonstrating that severe periodontal diseases adversely affect glycemic control, and that there is a direct and dose-dependent relationship between the severity of periodontitis and diabetes complications in patients with diabetes. Further, the group reported that there is emerging evidence that supports an increased risk for diabetes among patients with severe periodontitis.
With respect to interventions, the group noted that randomized controlled trials have consistently demonstrated that mechanical periodontal therapy is positively associated with approximately a 0.4% reduction in A1c at 3 months. This clinical impact is equivalent to adding a second medication to a regimen for managing diabetes. Also, the group noted there is no current evidence to support the adjunctive use of antimicrobials for the periodontal management of patients with diabetes.
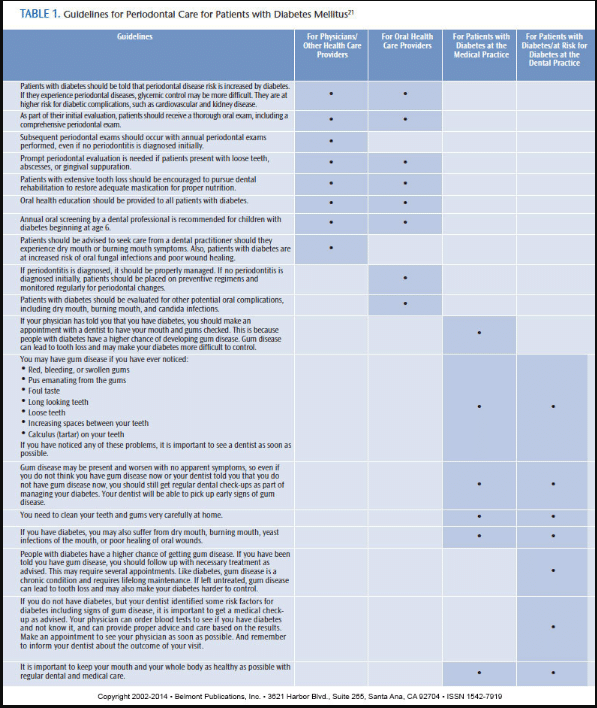
As a result of the group’s efforts, current guidelines for periodontal care for individuals with diabetes were proposed. These guidelines are offered for physicians and other medical professionals, oral health professionals, and patients with diabetes, and are summarized in Table 1.21
PRACTICAL APPLICATION
Oral health professionals should consider customizing dental and dental hygiene care for patients with diabetes. In addition, reviewing signs and symptoms of diabetes and risk factors should be part of the health history to identify those individuals who may have prediabetes or diabetes but have not yet been diagnosed. Given the potential for comorbidities, patients should be questioned concerning other health conditions and referrals made to medical providers for treatment. Monitoring of glucose and vital signs should be performed at the start of each appointment, and patients should be questioned about frequency of hypoglycemic episodes in order to be prepared to manage this emergency.
Comprehensive oral, caries, and periodontal examinations should be routinely performed in those with prediabetes and diabetes, and frequent dental hygiene appointments are needed to maintain periodontal health. Patients with prediabetes and diabetes should receive education about their oral and general health and encouraged to use prevention strategies that include lifestyle changes, smoking cessation, and weight management. These individuals can be taught how to conduct oral self-exams and advised to contact the dental office should they experience xerostomia, burning mouth, fungal infection, gingival bleeding, or abscesses. Patients need to understand the relationship between oral health and diabetes management. Annual eye, foot, and general health exams should be encouraged. In working together with other health care providers and patients with diabetes or prediabetes, dental hygienists can play a significant role in helping these individuals improve their health.
REFERENCES
- International Diabetes Federation. Diabetes: facts and figures. Available at: idf.org/worlddiabetesday/ toolkit/gp/facts-figures. Accessed April 23, 2014.
- Danaei G, Finucane MM, Lu Y, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011;378:31–40.
- World Health Organization. Global Status Report on Noncommunicable Diseases 2010. Available at: who.int/nmh/publications/ ncd_report2010/en. Accessed April 23, 2014.
- United States Department of Health and Human Services, National Diabetes Education Program. The Facts About Diabetes: A Leading Cause of Death in the US. Available at: ndep. nih.gov/diabetes-facts. Accessed April 23, 2014.
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;36(Suppl 1):S67–S74.
- Suh S, Kim KW. Diabetes and cancer: is diabetes causally related to cancer? Diabetes Metab J. 2011;35:193–198.
- Cukierman T, Gerstein HC, Williamson JD. Cognitive decline and dementia in diabetes—systematic overview of prospective observational studies. Diabetologia. 2005;48: 2460–2469.
- Biesses GJ, Staekenborg S, Brunner E, et al. Risk of dementia in diabetes mellitus: a systematic review. Lancet Neurol. 2006;5:64–74.
- National Diabetes Information Clearinghouse. Am I At Risk For Type 2 Diabetes? Taking Steps to Lower Your Risk of Getting Diabetes. Available at: diabetes.niddk.nih.gov/dm/pubs/riskfortype2. Accessed April 23, 2014.
- International Diabetes Federation. Diabetes Risk Factors. Available at: idf.org/worlddiabetesday /toolkit/gp/risk-factors. Accessed April 23, 2014.
- International Diabetes Federation. Diabetes Warning Signs. Available at: idf.org/worlddiabetesday/toolkit/gp/warning-signs. Accessed April 23, 2014.
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2013;36(Suppl 1):S67–S74.
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393–403.
- Knowler WC, Fowler SE, Hamman RF, et al. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet. 2009;374:1677–1686.
- Gaede P, Lund-Andersen H, Parving HH, et al. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Eng J Med. 2008;358:580–591.
- Wolf AM, Conaway Mr, Crowther JQ, et al. Translating lifestyle intervention to practice in obese patients with type 2 diabetics: Improving control with activity and nutrition (ICAN) study. Diabetes Care. 2004;27:1570–1576.
- International Diabetes Federation. Diabetes: Reduce Your Risks. Available at: idf.org/ worlddiabetesday/toolkit/gp/risk-factors. Accessed April 23, 2014.
- National Institutes of Health, National Diabetes Education Program. Redesigning the Health Care Team: Diabetes Prevention and Lifelong Management. Bethesda, Md: United States Department of Health and Human Services; 2011.
- American Diabetes Association. Executive summary: Standards of medical care in diabetes—2013. Diabetes Care. 2013;36(Suppl 1):S4–S10.
- Tamez-Pérez HE, Proskauer-Peña SL, Hern?ndez-Coria MI, Garber AJ. AACE comprehensive diabetes management algorithm 2013. Endocr Pract. 2013; 19:736–737.
- Chapple ILC, Genco R. Diabetes and periodontal diseases: consensus report of the Joint EFP/AAP workshop on periodontitis and systemic diseases. J Periodontol. 2013; 84(Suppl 4): S106–S112.
From Dimensions of Dental Hygiene. May 2014;12(5):63–67.
