 SRISAKORN/ISTOCK/GETTY IMAGES PLUS
SRISAKORN/ISTOCK/GETTY IMAGES PLUS
Dentinal Hypersensitivity Diagnosis
With careful consideration of myriad factors—from self-report to clinical exam—oral health professionals can effectively diagnosis and treat this common condition.
This course was published in the June 2020 issue and expires June 2023. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe dentinal hypersensitivity and its clinical manifestations.
- Discuss how to properly diagnose this common oral problem.
- Explain the prevention and management of dentinal hypersensitivity.
INTRODUCTION
How many patients do you treat for dentinal hypersensitivity? Do you have patients who experience sensitivity, but don’t tell you because they either believe sensitivity is normal, or they are afraid of restorative treatment to manage it? Or perhaps they think because it does not hurt all the time and if they don’t brush, it feels better, they can live with it. These are silent sufferers.
These patients will avoid activities, shun ice cream, and skip brushing areas that elicit pain. Of course, not brushing sensitive areas will only lead to more disease and more pain. The truth is, dentinal hypersensitivity is easy to treat once it is diagnosed. This article will help you diagnose hypersensitivity and provide immediate and effective treatment. It will also assist you in managing this condition to prevent further recession that can contribute to sensitivity issues.
Colgate Oral Pharmaceuticals is pleased to sponsor this CE article, “Dentinal Hypersensitivity Diagnosis” to support you as you care for your silent sufferers.
—Phyllis Martina, RDH, MBA
Senior Professional Education Manager
Colgate Oral Pharmaceuticals
Dentinal Hypersensitivity Is Highly Prevalent, Thus, Clinicians Must Be Well Versed on Its Diagnosis and Treatment.
Dentinal hypersensitivity (DHS) is characterized by fleeting, sharp pain to a tooth or teeth caused by an external thermal, tactile, or chemical stimulus.1–3 The pain felt in the area of DHS should disappear immediately once the external stimulus is removed; however the intensity may vary based on the amount of dentinal exposure.3 A variety of terms may be interchanged with DHS, including: dentinal sensitivity, cervical hypersensitivity/sensitivity, cemental hypersensitivity/sensitivity, and root hypersensitivity/sensitivity.4 The prevalence of DHS is reported to be between 3% and 98%.5 This wide range in prevalence is likely due to the variability in how studies define and assess DHS through questionnaires and/or clinical examinations.2,3,6–8 While DHS affects all ages, the peak occurrence is generally in middle-aged adults. DHS can impact all teeth and surfaces; however, it most commonly affects canines, first premolars, and the cervical margins on the facials of teeth.6,7
DHS can negatively impact patients’ lives and may affect patients performing daily activities. Patients may avoid eating certain foods, drinking particular drinks, and maintaining their oral health to prevent sensitivity from occurring.5,6 Despite much of the population experiencing DHS, it is often unrecognized and undiagnosed. Oral health professionals need to incorporate a combination of patient responses to specific questions, clinical examinations, and other tests to appropriately confirm if a patient presents with DHS and eliminate possible differential diagnoses. Once the diagnosis is confirmed, oral health professionals need to provide careful education on the cause and treatment of DHS. Numerous options for treatment of DHS currently exist; therefore, it is important to select treatments based on scientific evidence, patient’s needs and preference, and expertise.9
DENTINAL HYPERSENSITIVITY ETIOLOGY
The exact pathogenesis of DHS is unclear. In vitro, in situ, and epidemiological studies currently propose that exposed dentinal tubules respond to external stimuli and ultimately affect the dental pulp nerve.1–3,10 Multiple theories, such as direct innervation theory, odontoblast receptor theory, and Brännström’s hydrodynamic theory, are proposed to describe the mechanism of DHS. Each theory has limitations and does not account for all pain associated with DHS.3,4 The most widely accepted theory is the Brännström’s hydrodynamic theory which proposes that a stimulus—thermal, mechanical, chemical, or evaporative—strikes exposed dentinal tubules, causing a movement and change in the flow rate of the dentin fluid and generating an action potential in the nerves. This ultimately passes to the brain and produces pain.3,4 Research has found that when dentinal tubules are sensitive, they are wider and eight times more numerous than nonsensitive dentinal tubules.4
Identifying the potential cause(s) of DHS is critical, yet it is often an overlooked step in diagnosing and treating the condition. DHS is dependent on the loss of enamel and cementum, which exposes the dentin. Attrition, abrasion, erosion, and recession can lead to exposed dentin and are caused by a variety of reasons, including parafunctional habits, overzealous toothbrushing, highly acidic diet, chewing smokeless tobacco, and excessive vomiting.4,10,11 Further, mechanical trauma and periodontal diseases can lead to a loss of periodontal tissues and exposed dentin. Often these factors coexist and create an additive, synergistic effect to DHS.12

DIAGNOSIS OF DENTINAL HYPERSENSITIVITY
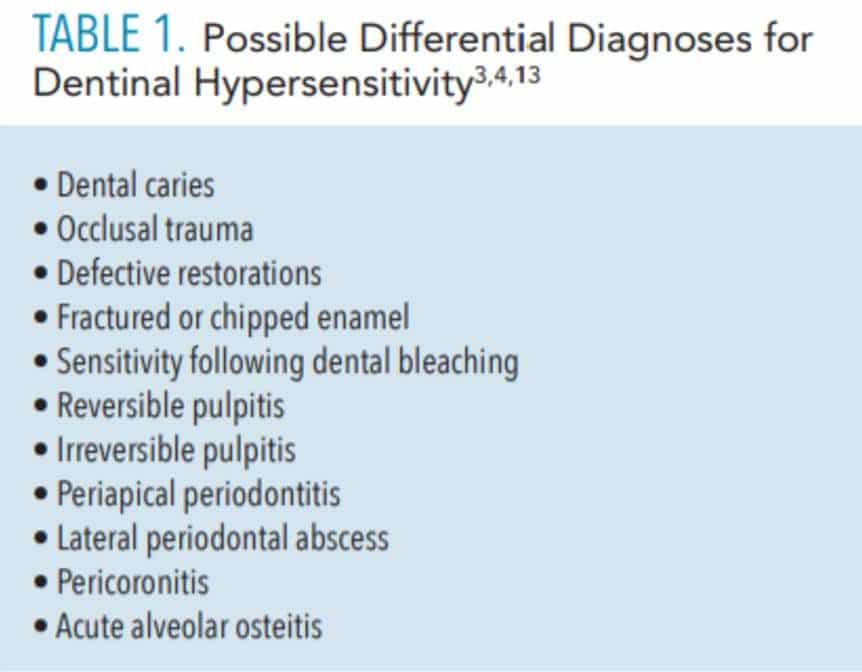
Diagnosing DHS is highly subjective in nature and often difficult to determine. There are a number of conditions presenting with similar characteristics and confounding problems that make DHS diagnosis challenging.13 It is critical to determine a correct diagnosis of DHS to appropriately and effectively relieve symptoms and treat DHS.4 Table 1 lists possible differential diagnoses.3,4,13 There is a lack in universally accepted guidelines for differential diagnosis of DHS and treatment; therefore, a thorough history, clinical examination, and other diagnostic tests are needed to determine if a patient has DHS.3,4
CHIEF CONCERN AND PATIENT HISTORY
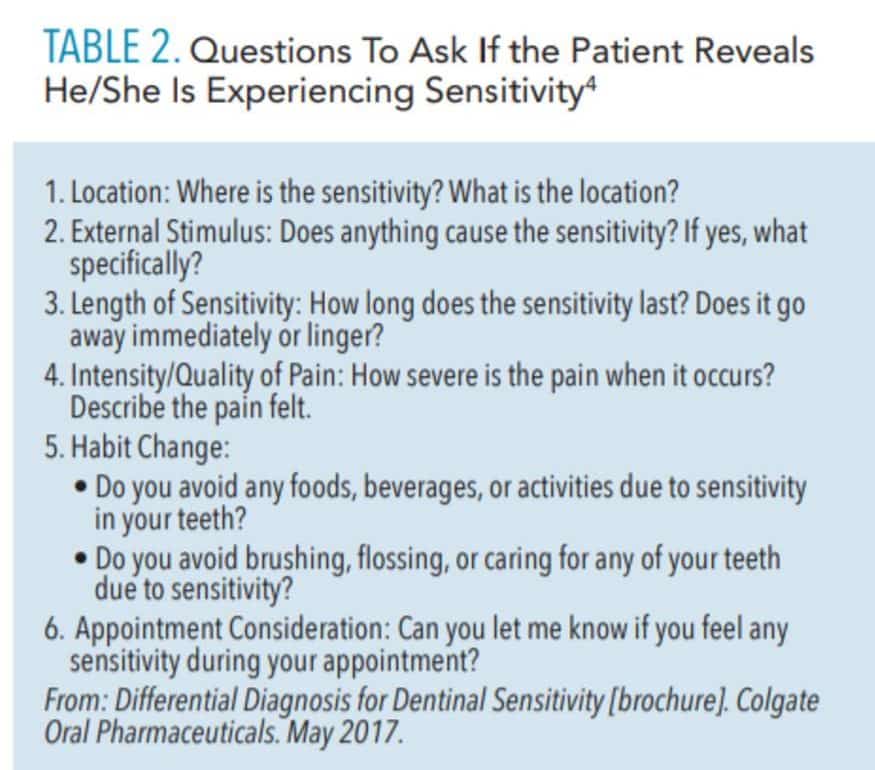
During the dental appointment, the oral health professional should learn about the patient’s chief concern and obtain an extensive history regarding that concern. Oral health professionals should ask questions to elicit understanding of the problem and conduct other examinations to assess for DHS and differentiate between other conditions. Table 2 lists the questions that should be asked if the patient reveals he/she is experiencing sensitivity.4 The responses to these questions will assist the oral health professional in differentiating conditions. For example, if the patient states that the pain is continuous, nontransient, spontaneous, or not caused by an external stimulus, then conditions other than DHS need to be considered.3,13
CLINICAL EXAMINATIONS AND TESTS
Diagnosis of DHS has previously relied on unprompted patient report; however, diagnosis should not solely rely on this.14 If patients reveal they experience tooth sensitivity, the area of sensitivity needs to be examined closer for evidence of dentinal exposure while considering that dentinal exposure may not be apparent depending on the severity.3,13
Radiographs should be taken according to the recommended guidelines set by the American Dental Association.15 Radiographs are of little use to determine DHS; however, they should be used to eliminate other conditions that cause sensitivity, such as caries, tooth fractures, defective restorations, and other pathological conditions. Intraoral photographs of the areas in question document findings and allow oral health professionals to assess exposure and condition over time.3
Other diagnostic tests for DHS should be considered to bolster patient self-report and a clinical examination. One of the most reliable ways to do this is to mimic the patient’s transient pain by applying a similar stimulus. Based on the patient’s chief concern, thermal or tactile stimuli can be applied to the location that DHS is suspected. To mimic a tactile stimulus, oral health professionals can use exploratory strokes with a dental explorer over the sensitive area. For mimicking air-flow stimuli, air from the air-water syringe should be carefully directed on the tooth surface. Further, there should be minimal gingival recession or root exposure if using the air from the air-water syringe.3 If a patient reports that the sensitivity is due to cold, then cold water may be applied to the area. With any of these tests, DHS should be considered if the pain is temporary and in combination with all other data collected.
Percussion should be used to rule out conditions from occlusal and dental trauma. If there is pain associated with percussion, then a DHS diagnosis is not warranted, and other conditions should be considered. DHS and a fractured tooth may produce similar transient pain. Along with visual inspection and transillumination to observe a fractured tooth, oral health professionals should instruct the patient to bite down on a cotton swab and then gently roll his/her bite over the swab. If pain occurs during this test, then it is from a fractured tooth or defective restoration, not DHS.3
TREATMENT OPTIONS
Following the diagnosis of DHS, oral health professionals should suggest treatment options based on the extent and severity of the problem. There are no universally used treatment modalities and treatment should be based on the patient’s needs, ease of use, and scientific evidence.6,9 Treatment options include patient education to address predisposing etiological issues and behavioral control, noninvasive treatments for relief, and, potentially, restorative and surgical treatment.13 Treatment options can first begin with inexpensive, noninvasive, and easy-to-perform options. If those options do not provide relief, then more invasive measures may need to be considered.16
PATIENT EDUCATION AND PREDISPOSING ETILOGICAL ISSUES TO ADDRESS
Patient education is a critical step in relief from DHS. This instruction should be tailored to each patient based on the etiological factors predisposing him/her to DHS and external stimulus causing the DHS. Education may include techniques in proper self-care, recommendation of product(s) for relief, nutritional counseling, or a combination of all of these. If possible, a reduction or elimination of the predisposing factors leading to DHS should be considered to prevent further progression of erosion, attrition, and recession.3,13,17
If the oral health professional identifies that DHS is a result of gingival recession from toothbrushing technique, then the patient should be educated on gentle toothbrushing strategies to prevent further worsening of the hard and soft tissues. The oral health professional can suggest holding the toothbrush with the index finger, middle finger, and thumb of the dominant hand to hold instead of palming the brush. Patients should use a soft or extra-soft toothbrush or a power toothbrush with a pressure sensor.3,1317–19
Medical conditions, such as gastric reflux or bulimia, may contribute to dental erosion and gingival recession.3,10 If these conditions are present or suspected, the oral health professional should consider nutritional counseling to prevent dental erosion and encourage the patient to consult with a dietitian or nutritionist.20 If the cause of gingival recession is from bruxism, methods to reduce the occurrence are warranted, including facial muscle massage, heat compress, and stress management. An occlusal guard may be considered to prevent further damage from bruxism.
NONINVASIVE TREATMENTS FOR RELIEF
A multitude of products are approved to provide relief for DHS. Product selection should be based on scientific evidence, individualized patient needs, and expertise of the clinician. DHS products are classified based on the mechanism of action, mode of action, and active ingredients. The mechanism of action for desensitizing agents occur in one of two ways: desensitizing the nerves, or occluding the dentinal tubules.21
The mode of action varies based on where the application takes place—at-home or in-office—and the delivery of the product. At-home applications typically are the most cost-effective means to relieve sensitivity and generally include toothpastes, mouthrinses, and serums.16,22 At-home products can be applied multiple times throughout the day; however, these products may take several days or weeks to provide DHS relief. When recommending any product, manufacturer guidelines must be followed, and oral health professionals need to educate patients on proper use. Toothpastes and mouthrinses have a variety of active ingredients that provide relief for DHS, including 5% potassium nitrate, 1.1% sodium fluoride, and 0.4% stannous fluoride.23 Potassium nitrate is commonly combined with sodium fluoride or amorphous calcium phosphate. Toothpastes and mouthrinses typically require repeated use over several days or weeks to achieve relief. In addition, the abrasiveness of the toothpaste should be considered. Serums with arginine and calcium carbonate as the active ingredient block the dentinal tubules to relieve pain.24 Combining arginine and calcium carbonate allows for the product to occlude the tubule to provide a quick seal and rapid, profound relief.23
In-office products include adhesive agents, varnishes, and serums. Adhesive agents desensitize the nerves and contain the active ingredients 5% glutaraldehyde and 35% hydroxyethyl methacrylate (HEMA) or HEMA with 0.5% sodium fluoride.24 These agents can be applied to exposed dentin prior to dental hygiene care or at completion of the appointment. Fluoride varnish typically contains 5% sodium fluoride and occludes the dentinal tubules.22,25 The length of time the fluoride varnish should remain on tooth surfaces depends on the product. Fluoride varnish can be applied at the completion of the dental hygiene appointment.
As use of hand and ultrasonic instrumentation may elicit DHS and cause patient discomfort, serums with arginine and calcium carbonate or adhesive agents should be considered to provide relief during the appointment and allow for instrumentation following application. Further, the abrasiveness of products, such as the grit of prophy paste, needs to be considered when a patient has DHS. Oral health professionals need to refer to manufacturer guidelines to ensure appropriate use of the product and provide accurate written and verbal post-care instructions for the patient.
Restorative treatment may be needed to combat DHS by covering areas of erosion, recession, and abrasion. These treatments may include direct restorations with resin-based composites or glass ionomer or indirect restorations with crowns or veneers to cover areas of erosion or abrasion causing DHS.13 If the cause of DHS is due to secondary dentin exposure from periodontitis, then treatment of that disease is needed to prevent further worsening of the tooth structures.3 Periodontal treatments may include guided tissue regeneration, flap surgery, and free gingival graft treatment to cover areas of gingival recession.26
Documentation of all findings—from chief concern to follow-up questions to clinical examination, to diagnostic test—must be completed. The written documentation should also include patient education and recommended products. This allows oral health professionals to continue to assess the condition over time and ensure appropriate management and care for patients with DHS.
CONCLUSION
DHS is a highly prevalent dental condition that is characterized by a sharp, temporary pain from an external stimulus. DHS can be difficult to diagnose and differentiate between other oral conditions. Careful consideration of patient self-report, clinical examination, and other tests are critical to differentiate DHS diagnosis and other conditions. Specific questions to the patient on intensity, severity, and location regarding sensitivity should be included during each dental appointment for patients presenting with sensitivity. Educating the patient, determining and eliminating the external stimulus causing the transient pain, and selecting in-office or at-home treatments should be considered. Treatment recommendations need to be based on individual patient needs and scientific evidence.
REFERENCES
- Absi EG, Addy M, Adams D. Dentine hypersensitivity. A study of the patency of dentinal tubules in sensitive and non-sensitive cervical dentine. J Clin Periodontol. 1987;14:280–284.
- Canadian Advisory Board on Dentin Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J Can Dent Assoc. 2003;69:221–226.
- Liu XX, Tenenbaum HC, Wilder RS, Quock R, Hewlett ER, Ren YF. Pathogenesis, Diagnosis and Management of Dentin Hypersensitivity: An Evidence-Based Overview for Dental Practitioners. In press.
- Davari AR, Ataei E, Assarzadeh H. Dentin hypersensitivity: etiology, diagnosis and treatment; a literature review. J Dent (Shiraz). 2013;14:136–145.
- Spileth CH, Tachou A. Epidemiology of dentin hypersensitivity. Clin Oral Invest. 2013;17(Suppl 1):S3–S8.
- Kopycka-Kedzierawski DT. Management of dentin hypersensitivity by Practitioners in the National Dental Practice-Based Research Network. J Am Dent Assoc. 2017;148:728–736.
- Kopycka-Kedzierawski DT, Meyerowitz C, Litaker MS, et al. Management of dentin hypersensitivity by National Dental Practice-Based Research Network practitioners: results from a questionnaire administered prior to initiation of a clinical study on this topic. BMC Oral Health. 2017;17:1–7.
- Mantzourani M, Sharma D. Dentine sensitivity: past, present and future. J Dent. 2013;41 (Suppl 4):S3–S17.
- ADA Center for Evidence-Based Dentistry. About EBD. Available at: https://ebd.ada.org/en/about. Accessed May 21, 2020.
- Addy M. Tooth brushing, tooth wear and dentine hypersensitivity—are they associated? Int Dent J. 2005;55(4 Suppl 1):261–267.
- Bartlett D, Smith, BGN. Definition, classification, and clinical assessment of attrition, erosion and abrasion of enamel and dentine. In: Addy M, Embery G, Edgar WM, Orchardson R, eds. Tooth Wear and Sensitivity. London: Martin Dunitz; 2000:87–92.
- Holland GR, Narhi MN, Addy M, Gangarosa L, Orchardson R. Guidelines for the design and conduct of clinical trials on dentine hypersensitivity. J Clin Periodontol. 1997;24:808–813.
- Gillam DG. Current diagnosis of dentin hypersensitivity in the dental office: an overview. Clin Oral Investig. 2013;17(Suppl 1):S21–S29.
- Cunha-Cruz J, Wataha JC, Heaton LJ, et al. The prevalence of dentin hypersensitivity in general dental practices in the northwest United States. J Am Dent Assoc. 2013;144:288–296.
- American Dental Association Council on Scientific Affairs and US Department of Health and Human Services Food and Drug Administration. Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure. Available at: ada.org/~/media/ADA/Publications/ADA%20News/Files/Dental_Radiographic_Examinations_2012.pdf?la=en. Accessed May 21, 2020.
- Schmidlin PR, Sahrmann P. Current management of dentin hypersensitivity. Clin Oral Investig. 2013;17(Suppl 1):S55–559.
- West NX, Lussi A, Seong J, Hellwig E. Dentin hypersensitivity: pain mechanisms and aetiology of exposed cervical dentin. Clin Oral Invest. 2013;17(Suppl 1):S9–S19.
- Miglani S, Aggarwal V, Ahuja B. Dentin hypersensitivity: recent trends in management. J Conserv Dent. 2010;13:218–224
- Suge T, Kawasaki A, Ishikawa K, Matsuo T, Ebisu S. Effects of plaque control on the patency of dentinal tubules: an in vivo study in beagle dogs. J Periodontol. 2006;77:454–459.
- Delgado AJ, Ólafsson VG. Strategies for managing erosive tooth wear. Dimensions of Dental Hygiene. 2019;17(10):34–39.
- Panagakos F, Schiff T, Guignon A. Dentin hypersensitivity: Effective treatment with an in-office desensitizing paste containing 8% arginine and calcium carbonate. Am J Dent. 2009;22(Special Issue A):3A–7A.
- Strassler HE, Serio FG. Dentinal hypersensitivity: etiology, diagnosis and management. Available at: https://dentalacademyofce.com/courses/2057/PDF/1103cei_sensitivity_rev1.pdf. Accessed May 21, 2020.
- Hatrick CD, Eakle WS. Dental Materials: Clinical Applications for Dental Assistants and Dental Hygienists. 3rd ed. St. Louis: Saunders; 2015:96–109.
- Schiff T, Delgado E, Zhang YP, Cummins D, eVizio W, Mateo LR. Clinical evaluation of the efficacy of an in-office desensitizing paste containing 8% arginine and calcium carbonate in providing instant and lasting relief of dentin hypersensitivity. Am J Dent. 2009;22 (Special Issue A):8A–15A.
- Ritter AV, de L. Dias W, Miguez P, Caplan DJ, Swift EJ. Treating cervical dentin hypersensitivity with fluoride varnish: A randomized clinical study. J Am Dent Assoc. 2006;137:1013–1020.
- Douglas de Oliveira DW, Oliveira-Ferreira F, Flecha OD, Goncalves PF. Is surgical root coverage effective for the treatment of cervical dentin hypersensitivity? A systematic review. J Periodontol. 2013;84:295–306.
From Dimensions of Dental Hygiene. June 2020;18(6):24-28.
