 POLLYANA VENTURA/E+/GETTY IMAGES PLUS
POLLYANA VENTURA/E+/GETTY IMAGES PLUS
Considering Combined Orthodontic-Periodontic Treatment
Research suggests a multidisciplinary approach involving orthodontics and periodontal therapy helps support positive patient outcomes.
This course was published in the March 2021 issue and expires March 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the benefits and risks of combined orthodontic and periodontal therapy.
- Discuss the role of orthodontic regimens in periodontal health.
- Explain the types of orthodontic approaches used in concert with treatment of periodontal diseases or in support of periodontal health.
In many clinical scenarios that require correction of malocclusion or misaligned dentition, a multidisciplinary approach involving orthodontics and periodontal therapy can have favorable outcomes. The intricate relationship between these two disciplines has been heavily researched in recent years. Sound periodontium is ideal so orthodontic treatment does not become deleterious and promote periodontal diseases. Studies have indicated positive outcomes for combined nonsurgical periodontal therapy in conjunction with orthodontic treatment.
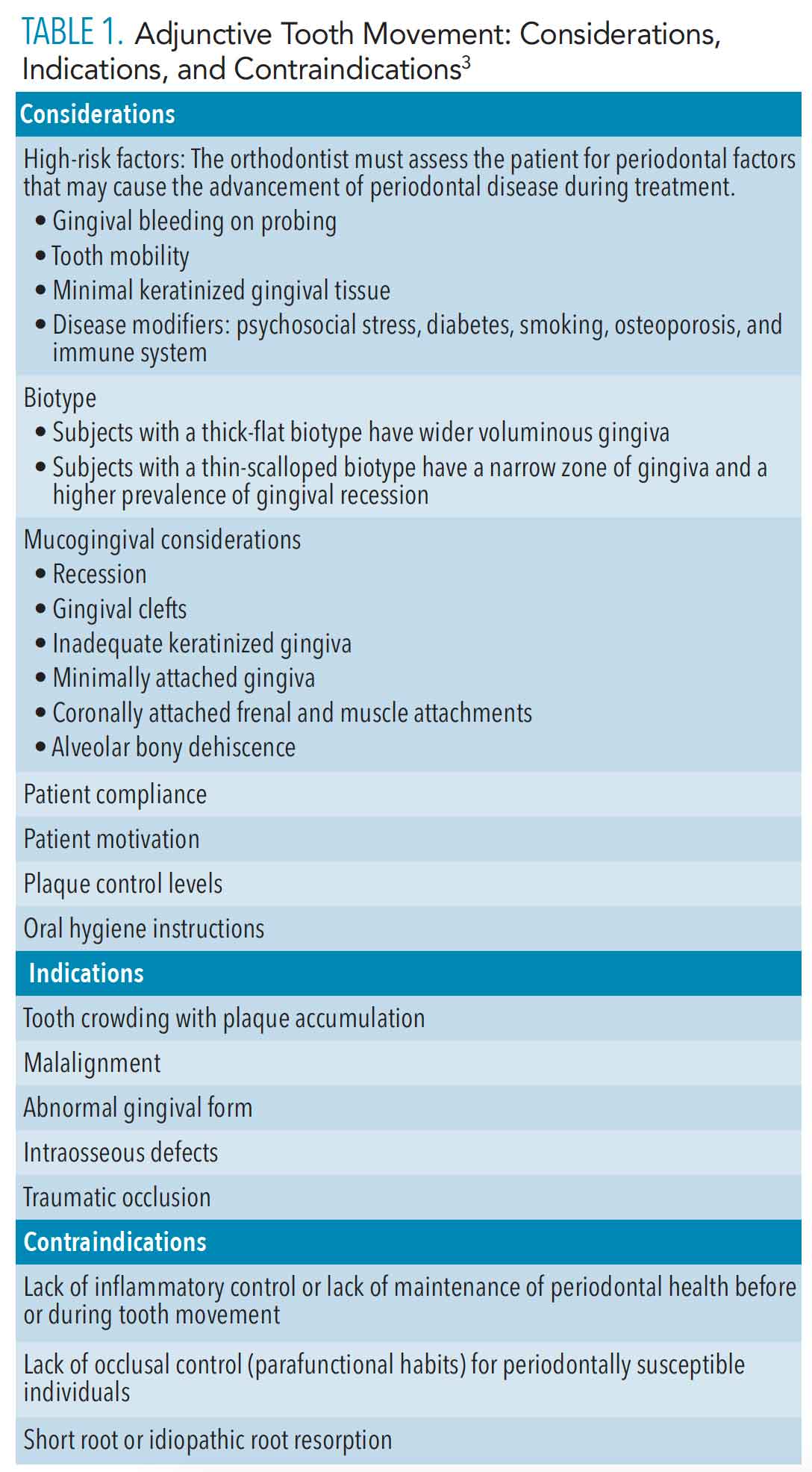
Orthodontic treatment is based on the principle that forces applied to teeth produce stresses on the periodontal ligament and, in turn, induce bone remodeling, which results in tooth movement. Because the periodontal ligament mediates this response, orthodontic treatment outcomes depend on the health status of the periodontium before, during, and after active orthodontic treatment.1 Periodontal diseases are a manifestation of pathogenic microbial biofilm. The pathology of periodontal diseases results in inflammation, which may lead to bone loss, pathologic migration, spacing, flared incisors, and trauma from occlusion. A periodontal-orthodontic multidisciplinary approach is well justified when managing such advanced cases.2 This approach significantly enhances periodontal health and dentofacial esthetics. However, various factors must be considered before moving forward with orthodontic treatment (Table 1).3 While tooth movement with reduced, but healthy, periodontium has been reported without additional attachment loss,1,2,4 if the orthodontic treatment involves tooth movement into and through a site with inflammation or angular bone loss, an enhanced rate of periodontal destruction may result.2,4
A well thought-out strategy must be developed for the management of susceptible patients to prevent the likelihood of periodontal damage during orthodontic treatment. With the goal of successful outcomes, periodontal health must be achieved before the course of the orthodontic treatment—and maintained throughout the procedure.
BENEFITS AND RISKS OF COMBINED THERAPY
The orthodontic principle of bone remodeling, in conjunction with tooth movement, is used to create favorable alveolar changes in the periodontium of patients with periodontal diseases. It should be reiterated that periodontal disease must be controlled before performing orthodontic treatment. In addition, various adjunctive periodontal therapies may be required throughout treatment to maintain periodontal health. Orthodontic treatments involving tooth movement—such as extrusion, intrusion, rotation, and bodily movement—are thought to prevent further periodontal breakdown, reduce plaque retention, improve gingival form and oral function, and enhance esthetics (Figure 1).3,5,6
Extrusion (eruption) of a tooth or teeth and the reduction of the clinical crown height are known to reduce probing depths and infrabony defects. As the bone follows the tooth during extrusion, the resulting bone deposition fills the bony defect and achieves a more coronally positioned, healthy connective tissue attachment.5 Tooth extrusion is the least hazardous type of movement to solve individual tooth defects due to periodontal diseases.5
Orthodontic intrusion may be indicated for teeth with horizontal bone defects. However, reports of the benefits of intrusion therapy are conflicting. Research has shown intrusion forces are apically concentrated and can cause root resorption and deepened infrabony pockets of anterior teeth.7 The recommendation is to apply only light orthodontic forces during active intrusion, while maintaining plaque control to prevent further periodontal destruction.3 The tipping movement is produced when a single force is applied to the crown. The tooth rotates around its center of resistance, and there is an increase in pressure at the tooth crest and root apex. Plaque control and the application of light tipping orthodontic force play a vital role in preventing clinical attachment loss and angular bony defects.3,8
In patients with partially edentulous dentitions and reduced vertical bone height, orthodontic bodily tooth movement into constricted bone areas may be a possibility for space closure. For tooth movement into areas with considerably reduced alveolar ridges, bone procedures (such as guided bone regeneration) should be considered.9
Orthodontic uprighting of mesially tilted molars has several advantages. The mesial deposition of alveolar bone caused by the tooth’s distal movement allows the elimination of bony defects and plaque retentive areas, thus reducing periodontal probing depths.3,4
In addition, orthodontic treatment is justified as a part of periodontal therapy if used to reduce plaque accumulation, correct abnormal gingival and osseous forms, improve esthetics, and facilitate prosthetic replacement. Further studies are needed to investigate the effects of combined orthodontic-periodontic treatment in patients with periodontal diseases.
ORTHODONTIC REGIMENS AND PERIODONTAL HEALTH
Compromised dentition—such as flared incisors, crowded teeth, and mesially inclined molars—creates isolated infrabony areas that serve as sites for etiological factors to populate, resulting in the formation of periodontal pockets and infrabony defects.7,10 The orthodontic appliances that are used to correct these maligned and mispositioned teeth can also treat these periodontal defects.
Intrusive mechanisms are indicated for the realignment of anteriorly displaced incisors and obtaining space closure. An intrusion utility arch is a frequent appliance used in this clinical scenario and includes the placement of a continuous wire on four incisors and first molars. The apparatus uses the first molar as an anchorage to apply approximately 100 g of force. In combined orthodontic-periodontal therapy, the load varies and depends on periodontal support of the associated dentition.10 This appliance produces a decrease in infrabony pockets in patients with interproximal defects and significant probing depths (≥ 6 mm).10
Removable orthodontic appliances have also proven useful in managing periodontal pockets associated with mesially inclined molars. A T-loop is the mechanism of choice frequently applied to simple removable appliances to upright mesially inclined molars. The T-loop extends into the buccal vestibular area and applies force to the teeth by a bonded button on a molar distal to the tooth in question. Studies have shown that with maintenance of oral hygiene and monitoring the periodontal status of both the mesially inclined molar and bonded tooth, significant improvement of periodontal tissues can occur.11 Positive outcomes include a reduction of bleeding on probing (specific to the area of disease), decreases in inflammation and clinical attachment loss, and remodeling of interproximal bone.11 To note, using removable devices to upright molars results in tipping and extrusion of the molar necessitating occlusal adjustment.
Various orthodontic appliances can be placed to produce orthodontic extrusion and contribute to treating localized periodontal diseases.5 Coronal migration of an impacted or intruded tooth increases the bone ridge and amount of attached gingiva.5,7 Passive extrusion is achieved using orthodontic brackets placed on the buccal surface of teeth adjacent to the tooth in question. This movement is optimal as it does not promote the movement of the anchored tooth, producing little to no effect on its periodontium.4 Extrusion forces are apt for the tooth requiring restorative work due to crown fracture, and its retained root requires coronal migration for an adequate crown-to-root ratio.5 A more rigid process can be applied through elastic band placement in the canal of a retained root. This band will have a hook on its most coronal end and connect to a rigid wire placed in a restoration on an adjacent tooth’s occlusal surface. This process can be challenging to execute on posterior teeth, however, due to the potential impact of occlusion.5,7
For optimal results, periodontal health should be achieved using surgical or nonsurgical periodontal therapy before the application of orthodontic appliances.4 Frequent clinical observation is warranted, and prophylaxis should be performed throughout orthodontic therapy to decrease plaque accumulation and mitigate disease progression.
![*click to enlarge]() SURGICAL TECHNIQUES
SURGICAL TECHNIQUES
The use of nonsurgical periodontal therapy before and during the initiation of orthodontic treatment is associated with increased orthodontic success and positive periodontal outcomes. Surgical periodontal techniques have also been shown to promote periodontal health and successful clinical outcomes.3 A circumferential supracrestal fibrotomy consists of removing epithelial attachments of involved teeth by inserting a surgical blade into the gingival sulcus of involved teeth. This procedure has proven effective in conjunction with root planing to prevent inflammatory granulation tissue formation in the periodontal space. Applying this surgical technique with orthodontic forces results in realignment and radiologic bone redisposition.7
Guided tissue regeneration techniques used in periodontics to regenerate lost periodontium have particular clinical indications. With narrow, two- or three-walled infrabony defects, this technique is extremely useful. Orthodontic mechanisms that contribute to transforming initial horizontal lesions to deep, narrow bony defects can be surgically treated via guided tissue regeneration with higher probability of success.7
Mucogingival considerations also play an essential role prior to orthodontic treatment. An adequate amount of keratinized and attached gingiva around the tooth’s cervical area is necessary for periodontal health and preventing future bone loss and gingival recession. For cases with limited attached gingiva and thin gingiva, the probability of recession is higher during orthodontic movement.3 A free gingival graft is a reliable, predictable, and common augmentation procedure to gain the attached gingiva. But other mucogingival methods, such as connective tissue grafts, can be used as well. It is preferable to perform gingival augmentation before orthodontic treatment, but various clinicians also recommend its use post-orthodontics.3

PERIODONTALLY ACCELERATED OSTEOGENIC ORTHODONTICS
Periodontally accelerated osteogenic orthodontics (PAOO) has become more popular recently, partly due to the increase in adult orthodontic therapy. Introduced by Wilcko et al,12 this technique incorporates a surgical aspect to orthodontic treatment to increase alveolar bone width, reduce incidences of apical root resorption, and stabilize the post-orthodontic periodontium (ie, reduced recession), all while shortening total active treatment time. Cases with short roots or requiring intrusion can also be treated using PAOO, with minimal complications reported.
This modality uses the concept of bone healing introduced by Frost13 known as regional acceleratory phenomenon (RAP). This technique accelerates naturally occurring processes in hard and soft tissue, such as perfusion, bone remodeling, and connective tissue formation (up to tenfold when in the presence of a noxious stimulus).14 These processes occur all the time during biologic homeostasis. When an injury or damage occurs, local factors initiate a cascade that signals the body to initiate healing of the affected area.
In case selection involving PAOO procedures, cone-beam computed tomography plays an important role in evaluating alveolar bone width. In PAOO, a full-thickness mucoperiosteal flap is needed to access the alveolar bone. This technique introduces the noxious stimulus in the form of corticotomies around tooth roots. Particulate bone grafts are used to increase the width of alveolar bone and provide support for periodontal tissues post-therapy. Mucogingival defects requiring connective tissue grafting can be performed at this time (as needed). The RAP process begins within days of the stimulus and mostly subsides by 6 months. It is vital to engage the orthodontic wires within the first 2 weeks and perform follow-up adjustments every 2 weeks thereafter to take full advantage of the RAP process.15
The RAP effect causes transient osteopenia in the surrounding alveolar bone.16,17 In turn, decreased bone density facilitates more rapid tooth movement. The decreased pressure needed on the compression side of the periodontal ligament may play a role in the reduced incidence of root resorption seen in PAOO cases.18,19
FINAL THOUGHTS
The intricate relationship between these two disciplines has been the subject of much study in recent years. The consensus is that orthodontic treatment is favorable when the periodontium is healthy. A team approach involving the orthodontist, periodontist, and restorative dentist should consider the indications for combined periodontal-orthodontic treatment in patients diagnosed with periodontal diseases, as outlined in Table 1. When applied strategically, various orthodontic forces—such as extrusion, intrusion, rotation, and bodily movement—can prevent further periodontal breakdown and, in some cases, improve radiographic bone levels, as shown in Figure 1.
When performed prior to applying orthodontic forces, various periodontal surgical options can prevent future attachment loss. For instance, mucogingival surgeries can help improve the attached gingiva, preventing gingival recession. The concepts of RAP and PAOO have been a game changer in adult orthodontics and for patients with thin biotypes. A radiographic analysis performed pretreatment can help define the patient’s biotype, and treatment can be customized accordingly. In closing, when combined with orthodontic treatment, the use of RAP, PAOO, and other periodontal techniques can result in favorable overall treatment outcomes.
CASE STUDY

esthetics. In collaboration with an orthodontist, the treatment plan included periodontally accelerated osteogenic orthodontic therapy to align her teeth, increase alveolar bone width,
stabilize the periodontium, and decrease the anticipated active treatment time (A). Cone-beam imaging focused on lower anteriors shows a thin biotype (B and C).


successful positioning of the lower anteriors, with acceptable biotype (B).
REFERENCES
- Tondelli PM. Orthodontic treatment as an adjunct to periodontal therapy. Dental PresJ J Orthod. 2019;24:80–92.
- Panwar M, Jayan B, Arora V, Singh S. Orthodontic management of dentition in patients with periodontally compromised dentition. J Indian Soc Periodontol. 2014;18:200–204.
- Vanarsdall RL. Orthodontics and periodontal therapy. Periodontol 2000. 1995;9:132–149.
- Zasciurinskiene E, Lindsten R, Slotte C, Bjerklin K. Orthodontic treatment in periodontitis-susceptible subjects: a systematic literature review. Clin Exp Dent Res. 2016;2:162–173.
- Bach N, Baylard JF, Voyer R. Orthodontic extrusion: periodontal considerations and applications. J Can Dent Assoc. 2004;70:775–780.
- Han JY. A comparative study of combined periodontal and orthodontic treatment with fixed appliances and clear aligners in patients with periodontitis. J Periodontal Implant Sci. 2015;45:193–204.
- Cao T, Xu L, Shi J, Zhou Y. Combined orthodontic-periodontal treatment in periodontal patients with anteriorly displaced incisors. Am J Orthod Dentofacial Orthop. 2015;148:805–813.
- Deepa D, Mehta DS, Puri VK, Shetty S. Combined periodontic-orthodontic-endodontic interdisciplinary approach in the treatment of periodontally compromised tooth. J Indian Soc Periodontol. 2010;14:139–143.
- Gorbunkova A, Pagni G, Brizhak A, Farronato G, Rasperini G. Impact of orthodontic treatment on periodontal tissues: a narrative review of multidisciplinary literature. Int J Dent. 2016;2016:4723589.
- Corrente G, Abundo R, Re S, Cardaropoli D, Cardaropoli G. Orthodontic movement into infrabony defects in patients with advanced periodontal disease: a clinical and radiological study. J Periodontol. 2003;74:1104–1109.
- Köseoğlu S, Fidancıoğlu A, Sağlam M, Savran L. Management of a periodontal pocket using a removable orthodontic appliance and nonsurgical periodontal therapy. Case Rep Dent. 2015;2015:374850.
- Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: two case reports of decrowding. Int J Periodontics Restorative Dent. 2001;21:9–19
- Frost HM. The regional acceleratory phenomenon: a review. Henry Ford Hosp Med J. 1983;31:3–9.
- Bockow R. Treatment planning with corticotomy-facilitated orthodontics. Sem Orthod. 2014;20:228–238.
- Murphy KG, Wilcko MT, Wilcko WM, Ferguson DJ. Periodontal accelerated osteogenic orthodontics: a description of the surgical technique. J Oral Maxillofac Surg. 2009;67:2160–2166.
- Cano J, Campo J, Bonilla E, Colmenero C. Corticotomy-assisted orthodontics. J Clin Exp Dent. 2012;4:e54–e59.
- Lee W. Corticotomy for orthodontic tooth movement. J Korean Assoc Oral Maxillofac Surg. 2018;44:251–258.
- Iino S, Sakoda S, Ito G, Nishimori T, Ikeda T, Miyawaki S. Acceleration of orthodontic tooth movement by alveolar corticotomy in the dog. Am J Orthod Dentofacial Orthop. 2007;131:448.e1–8.
- Ren A, Lv T, Kang N, Zhao B, Chen Y, Bai D. Rapid orthodontic tooth movement aided by alveolar surgery in beagles. Am J Orthod Dentofacial Orthop. 2007;131:160.e1–10.
From Dimensions of Dental Hygiene. March 2021;19(3):26-28,31.
