 ZLIKOVEC / ISTOCK / GETTY IMAGES PLUS
ZLIKOVEC / ISTOCK / GETTY IMAGES PLUS
Clinical Decision Points as Guidelines for Periodontal Therapy
The advanced features of the 2018 American Academy of Periodontology/ European Federation of Periodontology classification system will help oral health professionals formulate effective treatment plans for patients in need of periodontal therapy.
This course was published in the June 2022 issue and expires June 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the features of the 2018 American Academy of Periodontology and the European Federation of Periodontology periodontal classification system.
- Define appropriate treatments for periodontal diseases based on the stages outlined in the classification system.
- List the varying stages of periodontal diseases used in the classification system.
In 2017, the American Academy of Periodontology and the European Federation of Periodontology held a world workshop to formulate an improved classification of periodontal disease. In 2018, the findings were published in the Journal of Periodontology and Journal of Clinical Periodontology.1 Since its publication, the 2018 classification has become the standard used to classify and describe periodontitis. However, the clinical application of the new classification as a guide to the delivery of care for patients in need of periodontal treatment has remained unclear. We recently published a paper describing “decision points” for periodontal therapy based on the new classification.2 The goal of the decision points is to assist the clinician in using the advanced features of the new classification system to help formulate effective treatment plans for patients in need of periodontal therapy. The decision points also assist clinicians in evaluating the effectiveness of periodontal therapies, thus, helping to determine when advanced therapies are needed as well as to better plan for optimal periodontal maintenance.
Periodontal Classification
The 2018 periodontal classification can be accessed in detail at: https://www.perio.org/wp-content/uploads/2019/08/Staging-and-Grading-Periodontitis.pdf. Table 1 outlines the essentials of the classification. In its simplest form, the classification can be summarized as Stage I being the earliest manifestation of periodontal disease and then graduating up through Stage II and III to Stage IV, which is the most severe manifestation of periodontal disease. The speed of periodontal disease progression is described as Grade A through C, with Grade A representing slow progression and Grade C indicating rapid progression.
The grade of a case is extremely important in determining the long-term prognosis of a patient but it requires more than a single evaluation of the patient. When periodontal patients are initially classified, they are graded as B until the passage of time permits a more accurate estimate of periodontal progression. If it is determined that a patient has rapidly progressing periodontal disease (Grade C), prompt referral to a periodontist is recommended.
The full classification article referenced earlier should be reviewed for more information on determining the speed of disease progression and assigning a grade.1
Definitions of Treatments
Self-Care Instruction. The need for meticulous self-care can’t be overemphasized. Not only does quality self-care help preserve oral health, it also facilitates ongoing diagnoses and disease management. Absent quality self-care, it’s difficult to determine if a site that shows persistent signs of inflammation (eg, bleeding on probing) is experiencing gingival or periodontal inflammation. This distinction can be important because gingivitis is easily addressed, whereas persistent periodontitis calls for additional scaling and root planing (SRP) and frequently advanced periodontal therapy.
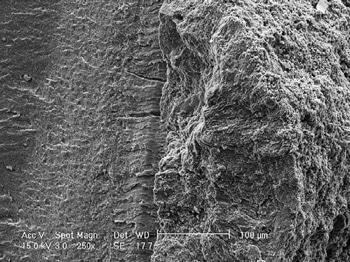
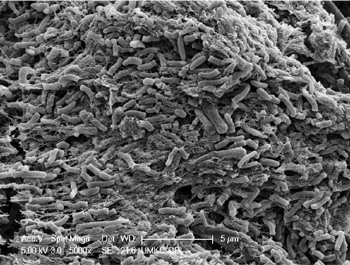
SRP. This periodontal therapy removes calculus and roughness from the root surfaces of diseased (periodontally involved) teeth. Unfortunately, the removal of all calculus from the root surface can be very difficult if the teeth have more than a few millimeters of periodontal pocketing. While bacterial plaque is the proximate cause of periodontal degeneration, once subgingival calculus has formed, it must be completely removed from the root for SRP to be a successful treatment for periodontal diseases. So-called “disinfection of the root surface” (removal of subgingival surface plaque but not subgingival calculus) is inadequate when subgingival calculus is present. Figure 1 and Figure 2 show that bacteria are harbored in residual calculus.
Studies show that even sterile calculus is cytotoxic, meaning it kills periodontal cells.3 There are many clinical observations that residual calculus is present at sites that do not respond adequately to periodontal treatment. Also, multiple studies have shown that skilled operators with unlimited operating time frequently leave a large percentage of undisturbed and fractured calculus on root surfaces following routine closed (blind) SRP.4 Additional studies have shown that “microislands” of calculus remain after SRP even with direct (open) visualization of the root surfaces. Thus, residual and fractured subgingival calculus remaining after SRP is undoubtedly a major cause of inadequate treatment of periodontitis.5
Advanced Therapy. Advanced periodontal therapy goes beyond traditional closed SRP. Advanced therapy may involve advanced visualization techniques, such as the use of a videoscope or periodontal endoscope, surgical access for (open) debridement of the periodontal lesion, and/or soft or hard tissue regenerative procedures. The type of advanced therapy used should be an informed, educated, and justifiable decision made by the therapist. Repeated unsuccessful closed SRP does not represent advanced therapy. If closed SRP does not resolve signs of periodontal inflammation, the patient should be informed of the need for and availability of advanced therapy.
Laser-based periodontal therapy is sometimes promoted as a stand-alone substitute for closed SRP or as an adjunct to traditional SRP. However, assessment of nearly 30 years of comparative studies suggest no additive benefit to lasers.6 Advanced therapy may be performed by anyone who is adequately trained to legally perform such therapy. Nevertheless, no matter who performs it, advanced therapy necessitates a level of care equivalent to that expected of a fully-trained periodontist.2
Reevaluation of Therapy. Reevaluation of the patient following all levels of periodontal therapy is mandatory in order to evaluate if the therapy has restored periodontal health. Depending on the treatment performed, patient reevaluation should occur at 6 weeks to 3 months post-therapy. If the patient returns to periodontal health after treatment, active therapy can be considered completed and the patient can be put on a maintenance schedule. If on reevaluation the patient continues to have inflammation, bleeding on probing, or deep pockets, the patient must be informed of the need for and availability of advanced care. Performing any level of periodontal therapy and not reevaluating the results and informing the patient of the availability of any necessary additional treatment or maintenance care, when appropriate, constitutes inadequate care.
Periodontal Maintenance. Periodontal disease is never completely cured but it can be controlled. Patients who have been diagnosed with periodontal disease (Stage I through Stage IV) and adequately treated should always be placed on a schedule aimed at maintaining periodontal health. Seminal to proper maintenance care are routine reevaluations to determine if active periodontitis has returned. Patients who continue to show signs of active periodontitis (Stage I through Stage IV) should not be placed in periodontal maintenance but should be provided advanced periodontal therapy.
Classification of Periodontitis and Treatment
Gingivitis. Gingivitis is not classified as a periodontal disease but as gingival inflammation. Pocket depth is not appreciably increased in gingivitis. The treatment for gingivitis is patient education and oral prophylaxis. SRP is not appropriate care for gingivitis. Studies have shown that SRP in shallow pockets can actually cause an increase of clinical attachment loss (CAL).7
Stage I Periodontitis. This stage of periodontitis is characterized by pocket depth of ≤ 4 mm, clinical attachment loss of 1 mm to 2 mm, and/or radiographic bone loss of < 15%. Stage I treatment is usually performed by the primary practitioner following a nonsurgical protocol. Treatment usually consists of oral hygiene instruction, oral prophylaxis of pockets of 3 mm or less, SRP performed in deeper pockets, site-by-site reevaluation and recording of responses to treatment ideally at 6 weeks post-treatment, and, assuming adequate response to therapy, placement of the patient on a periodontal maintenance plan that may start at every 3 months with a goal of every 6 months. Complete periodontal reevaluation is necessary at each maintenance visit. If active disease recurs or progression of anatomic damage is noted, the patient should be returned to active therapy at the stage of periodontal disease presented at the time of reevaluation.
Stage II Periodontitis. This stage is characterized by pocket depth of ≤ 5 mm, CAL of 3 mm to 4 mm, and/or radiographic mostly horizontal bone loss of between 15% and 33%. Limited furcation (class I) involvement may be noted.
Stage II treatment may be carried out by the primary practitioner or the patient may be referred to a periodontist. The decision for referral will be based on a thorough evaluation of the patient’s periodontal condition and the skill level of the practitioner. Stage II treatment usually consists of oral hygiene instruction, oral prophylaxis of pockets of 3 mm or less, SRP performed in 4 mm to 5 mm periodontal pockets, and reevaluation of response to treatment ideally at 6 weeks post-treatment.
Assuming the response to therapy is adequate, the patient should be placed on a periodontal maintenance schedule. It should be noted that adequate response to closed SRP is less likely to occur in some Stage II cases compared with Stage I cases. Many factors may be responsible, but the most frequent cause is the inadequate removal of all subgingival calculus and roughness using blind SRP. If the patient has not returned to periodontal health at the time of reevaluation, he or she should not be placed on a periodontal maintenance schedule but active therapy should continue—modified to better address the unique nature of the circumstances. This might consist of further closed SRP but advanced care is almost always indicated.
On the other hand, if the patient displays periodontal health, he or she should be placed on a periodontal maintenance schedule of every 3 months with reevaluation at each maintenance visit. If signs of active disease recur or progression of disease is noted, the patient should be returned to active therapy at the stage of periodontal disease presented at the time of reevaluations.
Stage III Periodontitis. This is an advanced stage of the disease and will usually not fully respond to nonsurgical (SRP) therapy. Based on this, initial referral to a periodontist for advanced care should be considered. Stage III periodontitis is characterized by pocket depth of ≥ 6 mm, CAL ≥ 5 mm, radiographic bone loss of 33 % or more, multiple class I to class III furcation involvements, and/or loss of one tooth to three teeth due to periodontal disease.
Stage III treatment will almost always necessitate the use of advanced periodontal therapy. Stage III treatment will usually consist of oral hygiene instruction; exhaustive evaluation of risk factors such as anatomic concerns or systemic medical concerns; SRP performed usually on all teeth; reevaluation of response to initial treatment (SRP) at 6 weeks; treatment planning for advanced therapy including a prosthetic treatment plans if indicated; performing advanced therapy, which will frequently be surgical in nature and may include therapy aimed at sculpting remaining tissue and/or aimed at regenerating lost tissue (bone and/or soft tissue); and placement on a periodontal maintenance and reevaluation schedule of a minimum of every 3 months depending on the response to therapy. More frequent maintenance visits may be indicated in some situations with the goal being to increase the time between maintenance intervals if patient response permits. As in all cases, if active disease returns or progression of disease is noted, the patient should be returned to active therapy at the stage of periodontal disease presented at the time of re-evaluation.
Stage IV Periodontitis. This stage is characterized by periodontal tissue degeneration greater than would be expected based on existing etiologic factors such as the amount of plaque, calculus accumulation, age, and other risk factors. There may also be evidence of past rapidly occurring episodes of bone and attachment loss. Stage IV periodontitis will also frequently present as multiple lost teeth and extensive prosthetic needs due to bite collapse and other factors. The periodontal conditions for Stage IV, such as pocket depth, CAL, furcation involvement, and other factors, are the same as in Stage III. The difference between the two stages is the extent of damage and the loss of greater than three teeth to periodontal disease.
Treatment of Stage IV periodontitis will require a team effort. Because of tooth loss and occlusal changes, prosthetic planning will always be part of therapy. Additionally, other disciplines will likely be needed, including orthodontics, endodontics, and physician consultation. The treatment of Stage IV periodontitis is usually best performed under the supervision of a periodontist. Advanced care is necessary for treatment of Stage IV cases and will vary with each patient. A specific description of therapy for Stage IV periodontitis is beyond the scope of this paper.
Summary
Several studies report that many “hopeless” periodontal teeth are salvageable for extended periods of time with appropriate and timely periodontal therapy.9–11 The treatment recommendations presented here are based on our many years of private practice, academic, and public health experience. Treatment should always be individualized for each patient, so no single treatment approach is correct for all patients or even for the same patient at different times. In early cases of periodontal disease (Stage I and possibly Stage II), basic treatments, such as oral hygiene instruction and SRP, may be adequate, but, in many cases, these treatments will be inadequate. This can only be determined by meticulous and frequent reevaluations that hopefully lead to appropriate modulations of subsequent care. Moreover, if periodontitis is not controlled by the treatment rendered, the patient must be informed of the need for and the availability of advanced care. In closing, the repeated use of basic therapies—such as closed (blind) SRP that fail to control periodontitis—is neither adequate nor ethical.
References
- Caton JG, Armitage G, Berglundh T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions—introduction and key changes from the 1999 classification. J Periodontol. 2018;89(Suppl 1):S1–S8.
- Harrel SK, Cobb CM, Sottosanti JS, Sheldon LN, Rethman MP. Clinical decisions based on the 2018 classification of periodontal diseases. Compend Contin Educ Dent. 2020;43:52–56.
- Ziauddin SM, Alam MI, Mae M, et al. Cytotoxic effects of dental calculus particles and freeze-dried Aggregatibacter actinomycetemcomitans and Fusobacterium nucleatum on HSC-2 oral epithelial cells and THP-1 macrophages. J Periodontol. September 5, 2021. Online ahead of print.
- Caffesse RG, Sweeney PL, Smith BA. Scaling and root planing with and without periodontal flap surgery. J Clin Periodontol. 1986;13:105–210.
- Harrel SK, Wilson TG Jr., Tunnell JC, Stenberg WV. Laser identification of residual microislands of calculus and their removal with chelation. J Periodontol. 20;91:1562–1568.
- Cobb CM. Lasers and the treatment of periodontitis: the essence and the noise. Periodontol 2000. 2017;75:205–295.
- Cobb CM. Nonsurgical periodontal therapy: mechanical. Annals Periodontol. 1996;1:443-490.
- Cobb CM, Sottosanti JS. A re-evaluation of scaling and root planing. J Periodontol. 2021;92:1370–1378.
- De Beule F, Alsaadi G, Peric M, Brecx M. Periodontal treatment and maintenance of molars affected with severe periodontitis (DPSI =4): an up to 27-year retrospective study in a private practice. Quintessence Int. 2017;48:391–405.
- Díaz-Faes L, Guerrero A, Magán-Fernández A, Bravo M, Mesa F. Tooth loss and alveolar bone crest loss during supportive periodontal therapy in patients with generalized aggressive periodontitis: Retrospective study with follow-up of 8 to 15 years. J Clin Periodontol. 2016;43:1109–1115.
- Graetz C, Dörfer CE, Kahl M, et al. Retention of questionable and hopeless teeth in compliant patients treated for aggressive periodontitis. J Clin Periodontol. 2011;38:707–714.
From Dimensions of Dental Hygiene. June 2022; 20(6)28,31-33.
