
Caries Classification
Effectively classifying caries lesions and implementing nonsurgical therapies, such as fluoride usage, can help reduce the damage done by tooth decay.
Dental caries remains a significant public health problem in the United States. By age 19, 67% of children will have experienced tooth decay.1 Once Americans reach the age of 75, 99% will have had dental caries.2 Oral health disparities persist despite sincere efforts by public health organizations to reduce disease incidence. Individuals with low socioeconomic status experience higher caries incidence and difficulty accessing professional dental care compared with their more affluent peers.3
Early-life risk factors for caries are especially relevant for oral health because permanent teeth start to develop in utero and during the first years of life.4,5 The “drill and fill” paradigm emphasizes treatment, not prevention of caries lesions and only negatively affects the caries disease process.6,7 It has been 10 years since Featherstone and colleagues presented their evidence-based model of caries management: caries management by risk assessment (CAMBRA). This approach relies on a careful analysis of a patients’ risk factors and protective factors. Oral health professionals assess the degree to which a patient’s individual risk factors outweigh the protective factors, and provide recommendations in order to tip the balance toward health. Thus, a patient who presents with an active caries lesion (clinically or radiographically visible) or has had a restoration placed in the past 3 years, is deemed high risk. Oral health professionals may perform a saliva flow test and/or bacterial culture, apply fluoride varnish, and recommend the use of prescription fluoride. Additional recommendations include increasing the frequency of a caries recare exam and recommending chewing gum containing xylitol. Those who exhibit positive oral health behaviors—such as maintaining good oral hygiene, adhering to an anti-cariogenic diet, and living in areas with community water fluoridation—are deemed low risk. Recommendations for this group may include decreasing the frequency of radiographs and professional fluoride application.8 Recently, a systematic literature review revealed that a majority of dentists and dental therapists would opt to intervene invasively (drill and fill) when a caries lesion confined to the enamel was diagnosed.4 The authors expressed concern regarding this philosophy and suggested that more emphasis should be placed on prevention.4 The caries process is dynamic and strongly affected by the host response and dietary habits. A lesion once considered in need of surgical intervention can be remineralized.9
International and national organizations have long recognized the need for a new caries classification system that incorporates evidence-based approaches to halt progression of caries lesions and minimize the need for surgical intervention.6,7 Thus, the International Caries Detection and Assessment System (ICDAS) and the American Dental Association Caries Classification System (ADA CCS) were created. The purpose of this article is to briefly review the systems and provide oral health professionals with additional resources on the subject.

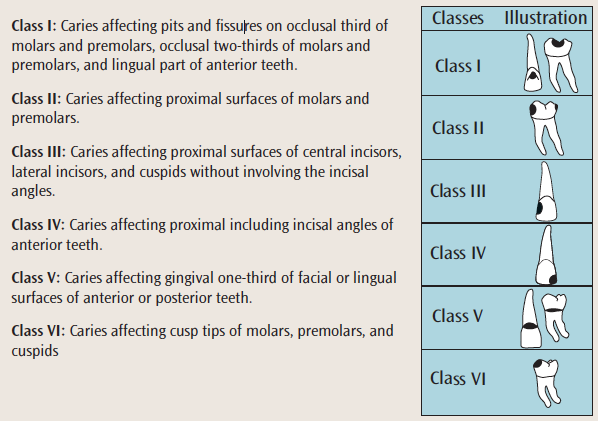
G.V. BLACK’S CLASSIFICATION OF DENTAL CARIES
For many years, caries lesions were classified according to G.V. Black’s Classification of Dental Caries, which was first introduced in 1908 and is still used today. Black’s original classification consisted of five categories, with a sixth added later (Table 1).10
Today, much more is known about the caries disease process and how to most effectively treat it. In 2001, the National Institutes of Health sponsored the Consensus Development Conference on Diagnosis and Management of Dental Caries Throughout Life. The consensus was that the effective identification and classification of caries are critical to its treatment, which should focus on less invasive strategies, such as the use of fluoride and antimicrobials and sealant placement.11
INTERNATIONAL CARIES DETECTION AND ASSESSMENT SYSTEM
The ICDAS is an evidence-based tool used to classify dental caries.12 The ICDAS Foundation is charged with updating and disseminating information regarding the system. First introduced in 2004, ICDAS has been updated as new innovations prove their effectiveness. The process, simplified, is as follows:
- Tooth surfaces are cleaned and visually inspected.
- The oral health professional uses a ball-point probe to examine the tooth surface. While still common in clinical practice, the use of an explorer to detect caries lesions has long been discouraged.13
- Lesions are scored from 0 to 6 (Table 2).
- Treatment recommendations are made based on the score.
AMERICAN DENTAL ASSOCIATION CARIES CLASSIFICATION SYSTEM
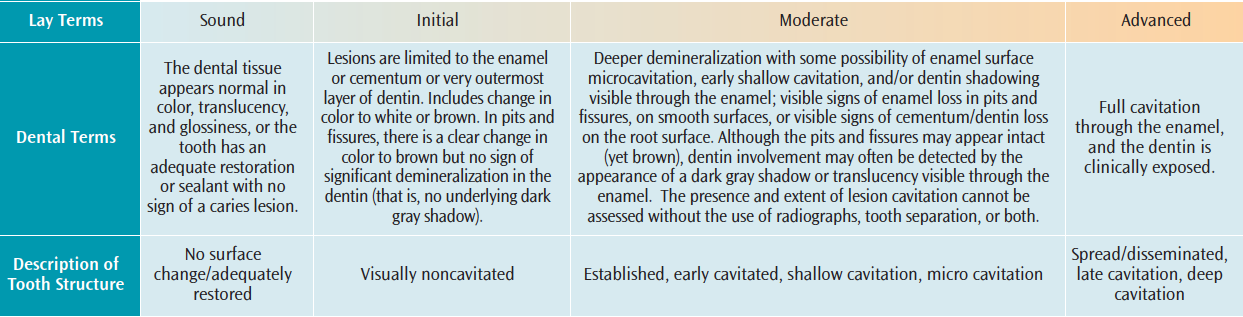
In 2008, the ADA Council on Scientific Affairs convened a group of experts to develop a new caries classification system that could be easily adapted in clinical practice.7 Similar to the ICDAS, the ADA CCS uses categories (sound, initial, moderate, advanced) to score a tooth surface’s clinical appearance (Table 3). The initial, moderate, and advanced categories are each subdivided to account for variations in appearance.
Once the tooth surface has been cleaned, the hard tissue examination can begin. The oral health professional, utilizing a good source of light, air dries the teeth and begins a visual inspection of all surfaces, noting any that appear white (chalky) or discolored. A ball-point probe or rounded explorer is then used to evaluate surface texture. For approximal lesions, radiographs are recommended. Radiographic recommendation guidelines should be followed.14 As these guidelines cannot consider the individual variations of each patient, clinicians are encouraged to use them as part of their decision-making process but they may opt to override the recommendations based on patient needs. The ADA also suggests the use of elastomeric tooth separation to help accurately detect interproximal decay.7
Neither the ICDAS nor the ADA CCS recommend the use of caries detection devices. Most of these devices use light and lasers to detect caries lesions before they are clinically detectable. Changes in tooth density will cause light, heat, and electrical stimuli to transmit differently when compared to healthy hard tissues. The May 2015 issue of the ADA Professional Product Review includes a review of manufacturer claims and determined that the devices are better suited to help manage the caries disease process.15These devices have yet to reach a level of reliability to make them capable of determining the presence of caries lesions.
CONCLUSION
In a 2015 survey of dentists, the National Dental Practice-Based Research Network discovered that more than 70% of respondents were unaware of the ADA CCS.16 Dental caries is a preventable, infectious disease whose eradication will require the diligent use of new, evidence-based methodologies and therapies. As the ICDAS and ADA CCS include a thorough assessment of caries risk factors (sugary foods/drinks, low socioeconomic status, xerostomia, community water fluoridation, visible plaque, deep pits/fissures, history of caries, pathogenic bacteria, use of fluoride dentifrice) incorporating one of these systems into a caries-prevention program—along with the use of fluoride and nonfluoride caries preventive agents—will help ensure positive outcomes. The responsibility of detecting and managing caries falls on all dental team members, not just the dentist. Oral health professionals have an ethical responsibility to promote those practices that most benefit patients. Table 4 provides a list of resources so clinicians can learn more about both the ICDAS and ADA CCS approaches.
Researchers have advanced the management of the caries disease process by creating caries classification systems. Now it is up to clinicians in private practice to implement the evidence so that caries can be more effectively reduced across all populations.
REFERENCES
- Dye BA, Thornton-Evans G, Li X, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011–2012. NCHS Data Brief. 2015;191:1–8.
- Dye BA, Thornton-Evans G, Li X, Iafolla T. Dental caries and tooth loss in adults in the United States, 2011–2012. NCHS Data Brief. 2015;197:197.
- Shaefer HL, Miller M. Improving access to oral health care services among underserved populations in the US: is there a role for mid-level dental providers? J Health Care Poor Underserved. 2011:22:740–744.
- Innes NP, Schwendicke F. Restorative thresholds for carious lesions: systematic review and meta-analysis. J Dent Res. 2017;96:501–508.
- William V, Messer LB, Burrow MF. Molar incisor hypomineralization review and recommendations for clinical management. Pediatr Dent. 2006;3:224–232.
- FDI World Dental Federation. 2012 Classification of Caries Lesions of Tooth Surfaces and Caries Management Systems. Available at: fdiworlddental.org/resources/policy-statements-and-resolutions/classification-of-caries-lesions-of-tooth-surfaces-and. Accessed June 26, 2017.
- Young DA, Nový BB, Zeller GG, et al. The American Dental Association Caries Classification System for clinical practice: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2015;146:79–86.
- Young DA, Featherstone JD. Caries management by risk assessment. Community Dent Oral Epidemiol. 2013;41:53–63.
- Weinstein P, Harrison R, Benton T. Motivating mothers to prevent caries confirming the beneficial effect of counseling. J Am Dent Assoc. 2006;137:789–793.
- Black GV. Extracts from the last century. Susceptibility and immunity by dental caries by G.V. Black. Br Dent J.1981;151:10.
- NIH Consensus Development Conference on Diagnosis and Management of Dental Caries Throughout Life. Bethesda, Maryland, March 26-28, 2001. Conference Papers. J Dent Educ. 2001;65:935–1179.
- International Caries Detection and Assessment System Foundation. International Caries Detection and Assessment System. Available at: icdas.org. Accessed June 26, 2017.
- Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007;369:51–59.
- American Dental Association and Food and Drug Administration. Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure. Available at: ada.org/~/media/ADA/Member%20Center/FIles/Dental_Radiographic_Examinations_2012.pdf. Accessed June 26, 2017.
- Young DA, Slayton R. A DA Professional product review: Caries detection devices. ADA Professional Product Review. 2015;10(2):1–3.
- National Dental Practice-Based Research Network. Quick Poll Results—Caries Classification System. Available at:nationaldentalpbrn.org/tyfoon/site/fckeditor/Caries%20Classification.pdf. Accessed June 26, 2017.
Featured photo by FTWITTY/ISTOCK/GETTY IMAGES PLUS
From Dimensions of Dental Hygiene. July 2017;15(7):17-18, 21.

{kind=link}