The Relationship Between Facial Paralysis and Xerostomia
I have consistently observed the presence of xerostomia among patients with facial paralysis. Is there an association between the two?
QUESTION: I have consistently observed the presence of xerostomia among patients with facial paralysis. Is there an association between the two?
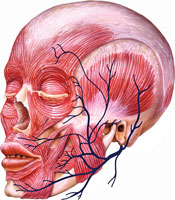
ANSWER: Facial paralysis affects the cranial nerve VII, also known as the facial nerve (Figure 1). The functions of the facial nerve are very complex; the motor fibers are responsible for innervation of all facial muscles, such as the frontalis, orbicularis oris, and others. It also has a sensory component, which is responsible for taste to the anterior two-thirds of the tongue, as well as tear and saliva production. Particularly, the submandibular and sublingual glands receive their parasympathetic innervation from the facial nerve.
Xerostomia is one of the possible side effects of facial paralysis. Although there is no definite explanation for the association between dry mouth and facial paralysis, it is most likely due to the affected facial nerve impacting saliva production, but it may also be related to drooling caused by facial weakness. Management of xerostomia related to facial paralysis should be treated similarly to medication-induced xerostomia. Addressing dry mouth symptoms is important because, if left untreated, patients are at increased risk of fungal infections, dental caries, periodontal diseases, and other oral problems.1,2
Mechanical stimulation of the salivary glands with sugar-free chewing gum may be helpful. In addition, saliva substitutes—including tablets, sprays, swabs, gels, and mouthrinses—may alleviate symptoms. Professional dental care and exposure to topical fluoride products should be encouraged in order to prevent dental disease from occurring or progressing. Patients should be advised to drink plenty of water and to avoid alcohol, caffeine, and tobacco.1,3
ACKNOWLEDGMENTS
- FIGURE 1: BO VEISLAND / SCIENCE PHOTO
References
- Guggenheimer J, Moore PA. Xerostomia: etiology, recognition and treatment. J Am Dent Assoc. 2003;134:61–69.
- Weinburg MA, Theile CM, Fine JB. In: Cohen M, ed. Oral Pharmacology for the Dental Hygienist. 2nd ed. Upper Saddle River, NJ: Pearson Education Inc; 2012.
- United States Department of Health and Human Services. Dry mouth? Don’t delay treatment. Available at: www.fda.gov/forconsumers/consumerupdates/ucm254273.htm. Accessed September 12, 2013.
From Dimensions of Dental Hygiene. October 2013;11(10):78.
