 DEXTORTH / ISTOCK / THINKSTOCK
DEXTORTH / ISTOCK / THINKSTOCK
Arresting Caries
The use of silver diamine fluoride offers many benefits in arresting caries lesions, especially among underserved and low-income populations.
This course was published in the July 2016 issue and expires July 31, 2019. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe silver diamine fluoride’s (SDF) mechanism of action.
- Identify possible uses for SDF in clinical practice.
- List the contraindications for SDF.
- Discuss the technique for using SDF.
Dental caries, a common chronic disease, remains a significant problem in all age groups.1 Researchers have long sought additional approaches to caries management.2 One of these, caries management by risk assessment (CAMBRA), is based on the unique risks faced by each patient.3 CAMBRA is an evidence-based approach to preventive and reparative treatment of early caries lesions that can be integrated into any dental office setting. Sample CAMBRA protocols have been published and updated for children4 and adults.5,6 These guidelines focus on modifying individuals’ risk factors via a combination of chemical therapeutic interventions, coupled with behavioral modifications targeted at altering microbiota while supporting tooth remineralization.
Recently, silver diamine fluoride (SDF) emerged as a new chemotherapeutic option for caries management in the United States. SDF has long been used in Japan, Australia, and Argentina in caries prevention, and the value of silver ions to treat dental caries has been known for more than a century. SDF currently is designated by the US Food and Drug Administration as a treatment for dentinal hypersensitivity in adults. The application of SDF to treat caries is considered an off-label use, similar to fluoride varnish. As with other forms of off-label use, however, clinicians should use their professional judgment when choosing SDF for caries prevention.7
A 2009 systematic review reported that SDF is a safe and effective caries-preventive agent that appears to meet both the World Health Organization’s Millennium Goals and the US Institute of Medicine’s criteria.8 The use of SDF to chemically arrest active caries eliminates the need for local anesthesia administration and dental drills, which can improve children’s experience in the dental office. This paper will review the scientific properties of SDF and its clinical applications for caries arrest that may be of particular interest to dental hygienists.
MECHANISM OF ACTION
SDF is an inexpensive and colorless topical agent used to treat and prevent dental caries.9 Silver is a substantive antimicrobial that limits the reinvasion of cariogenic bacteria after application.10 The fluoride ions promote remineralization. Upon application of SDF to a decayed surface, a silver-protein conjugate layer forms, which increases resistance to acid dissolution and enzymatic digestion.11 Treated lesions will increase in mineral density and hardness as lesion depth decreases.12
In 2014, SDF was cleared by the US Food and Drug Administration for marketing as a Class II medical device to treat tooth sensitivity. It became commercially available in the US in 2015. Recently, Horst et al9 recommended the widespread off-label use of SDF for treating and preventing caries in the US. In January 2016, the current dental terminology (CDT) billing code 1354 for interim caries arresting medicament application became active. It states: “Conservative treatment of an active, nonsymptomatic caries lesion by topical application of a caries-arresting or inhibiting medicament without mechanical removal of sound tooth structure.” With the introduction of CDT 1354, Medicaid began reimbursing for the application of SDF.
Several randomized clinical trials evaluated the efficacy of SDF in treating dental caries. Two studies in children demonstrated 91% to 93% caries arrest after 2 years to 3 years of biannual application.13,14 Two studies showed 65% to 79% arrest after 2 years to 2.5 years with an annual application.15,16 A dose-response relationship was seen, with better outcomes accompanying a higher frequency of application.14 Reapplication appears to provide additional benefits, as after 1 year, the caries arrest rate plummeted without reapplication16 and increased with reapplication.14 Thus, oral health professionals may want to observe the effects of SDF rather than prescribe conventional restorative dentistry prematurely. Studies have reported better caries prevention with an annual application of SDF compared with other topical medicament treatments, such as four times per year applications of fluoride varnish15,17 or chlorhexidine varnish.17
Two reports using silver compounds (SDF or silver nitrate plus fluoride varnish) have shown the potential to dramatically reduce the need to treat children with behavior issues for early childhood caries in a hospital setting. The first report was from a private practice setting where Medicaid-eligible children comprised a large percentage of the patient population.18 The second report was from a large Medicaid-managed care organization in Oregon with hundreds of thousands of enrollees.19
SDF has a highly impressive safety profile. Based on a large 500-fold LD-50 (lethal-dose for 50% of those who imbibe a particular dose) safety margin and a postulated 100% absorption, a single drop (25 ul) results in a reasonable dose limit of 1 drop/10 kg (~ 22 lbs) child per visit.9 Predictable side effects include blackening of the treated lesion, a short-lived bitter metallic taste, temporary staining of soft tissues, staining of clinic surfaces, and residual SDF stains left on treatment trays. Thus, reasonable caution should be taken to avoid touching patients’ soft tissues, as well as clinical surfaces. Patients should be alerted to expect the lesion to darken substantially over a week.
POSSIBLE USES IN CLINICAL DENTAL PRACTICE
Before placing SDF, oral health professionals should consider whether a patient is appropriate for this treatment. As mentioned earlier, SDF is used “off label” for arresting caries, especially among those in certain populations. SDF will likely benefit patients diagnosed with salivary dysfunctions, those with special health care needs, the underserved, medically compromised individuals, and those with severe early childhood caries. SDF may also be useful for treating lesions that would otherwise be difficult or impossible to treat using traditional methods.9 Furthermore, SDF is likely useful in the enamel pits and fissures surfaces of patients at high caries risk who may not be able to tolerate conventional sealants. SDF can also be used in conjunction with sealants when a lesion is suspected but has not been visualized.
Once it is determined that a patient is a candidate for SDF treatment, oral health professionals must receive informed consent from patients or parents/caregivers regarding the risks, benefits, and alternatives to SDF therapy.
Clinicians should also consider if repeated SDF application is appropriate. For example, when treating a patient who is not likely to return for a follow-up evaluation and treatment, clinicians need to consider the following options:
- No SDF placement.
- Place SDF only once with the understanding the patient may not return for subsequent applications.
- Place SDF and glass ionomer cement (GIC) sealant/restoration during the same appointment.
CONTRAINDICATIONS
While SDF is safe, clinicians should exercise caution in some situations. For a tooth that is symptomatic, partially necrotic, or otherwise pulpally involved, SDF may not be beneficial and immediate traditional treatment may be a better approach. With careful application, SDF will not go beyond treated sites, but patients and providers should be aware that SDF will cause stinging if it contacts soft tissue ulcerations or lacerations.
Patients who refuse the use of fluoride may require extended discussions to obtain informed consent. Clinicians may mention that SDF is twice as concentrated as fluoride varnish, thereby lowering the volume used.
Using conventional GIC restorative materials for light curing is not needed and may help reduce SDF’s discoloration effects upon light curing, which is required for resin modified glass ionomer and composite. A meta-analysis of long-term clinical trials reported that heavy body (low viscosity) GICs are at least as effective in preventing caries in permanent molars as are resin sealants.20 With conventional GICs, maximal remineralization occurs at the tooth interface.21 Future research is needed to investigate the long-term effects of SDF on dental materials with which it may contact.
In situations when patient behavior necessitates short treatment times, a light-cured resin modified glass ionomer may be more appropriate instead of a pure conventional glass ionomer because setting with a light may be faster. Light curing after SDF placement can increase the darkening of the lesion and resin-based restorative materials, but it will not make it as dark as amalgam. The chemical mechanism of such darkening is not well understood.
REGULATIONS ON PROVIDERS WHO CAN PLACE SILVER DIAMINE FLUORIDE
Potential providers are encouraged to examine their states’ dental board regulations to determine who can lawfully place SDF, sealants, and nonsurgical restorations. Clinicians permitted to place fluoride varnish will most likely be able to place SDF. However, in some states, it is unclear who, other than dentists, are credentialed to perform caries arrest by medicament (CDT 1354). Where nondentists are permitted to perform caries arrest procedures, these should be performed in collaboration with the dentist of record and/or as dictated by state laws. In summary, before implementing SDF therapy, clinicians should clarify with their state dental boards the rules regarding who may perform caries arrest by medicament (CDT 1354).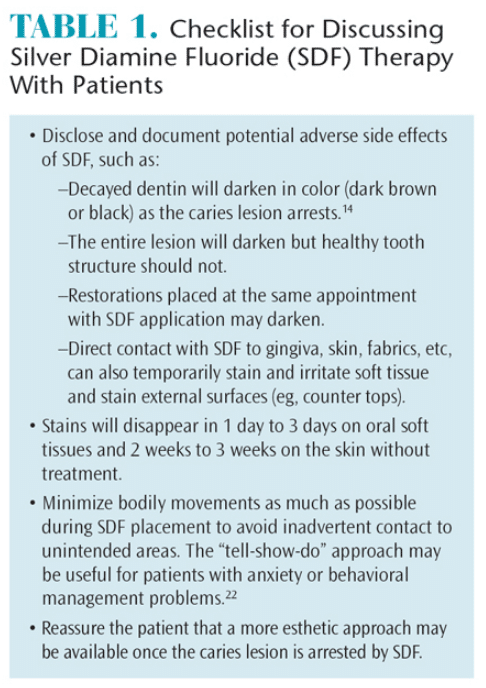
ENSURING EFFECTIVE PATIENT COMMUNICATION
After completion of a thorough exam, charting, and caries risk assessment, treatment plan options should be discussed with the patient.5 With guidance from an appropriate oral health professional, patients should ultimately choose the best SDF option as determined by their wants, needs, financial status, and abilities to cooperate with proposed treatment. Appropriate discussions with a patient or parent/caregiver can motivate and encourage preventive treatment aimed at halting and preventing future disease, thereby limiting or eliminating the need for more invasive procedures in the future. Table 1 provides a checklist for use when discussing SDF therapy with patients.
TECHNIQUE
Arresting a caries lesion with SDF may be beneficial when traditional methods are not likely to be successful. In the case of a patient with multiple caries lesions that cannot be immediately restored, SDF can slow the disease process and decrease sensitivity until definitive restorative care can be performed. Repeated application of SDF may help preserve tooth structure. In such cases, reapplication has been recommended at least biannually until a tooth exfoliates, is extracted, or the tooth is restored.9 In situations where restorations are not an option, repeated applications of SDF may be the best option.
The mechanics of how practitioners are currently coding and billing for SDF application with restoration is still evolving. Clinical applications in which SDF is combined with GIC sealant/restoration include:

CINDY Y. LEE, DMD
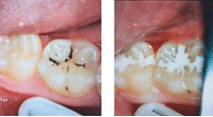
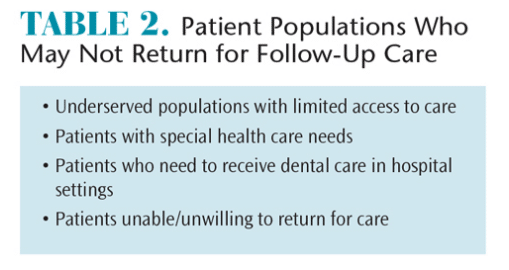
- Multiple applications of SDF followed by GIC sealant/restoration after lesion arrest (Figure 1).Ideally, an approach relying on multiple applications of SDF followed by placement of a restoration (if needed) is preferred.9 However, there may be situations where a practitioner will only be able to see the patient once (Table 2).
- Single application of SDF with immediate GIC sealant/restoration (Figure 2).If there is concern that a patient may not return for multiple SDF applications or if a patient has large numbers of active lesions or particularly large lesions, making it impractical to restore all teeth at one appointment, less time-consuming techniques such as SDF in combination with immediate GIC sealant/restoration placements may be considered.23
- Arrest and repair secondary caries with SDF.
![]()
At an existing restorative margin, SDF can be applied to arrest secondary caries followed by repair of the restoration if appropriate and consistent with tooth preservation strategies.24 Placement of SDF and GIC sealant/restoration is considered a restorative CDT code. It is not appropriate to bill CDT 1354 along with immediate placement of GIC sealant/restoration.
CONCLUSION
The science and versatility of SDF make a strong case for widespread adoption. The use of SDF does not preclude the option of subsequent placement of traditional restorations for purposes of restoring esthetics, comfort, and function. SDF offers unique disinfection and remineralization properties that can reduce the need for traditional invasive operative procedures. Combining the synergistic compatibilities of SDF and conventional GIC offers new ways to empower and motivate oral health professionals and patients to transform disease to health.
ACKNOWLEDGMENT
Jeremy Alan Horst, DDS, MS, PhD, was supported by National Institutes of Health/National Institute of Dental and Craniofacial Research grant T32-De007306.
References
-
- Beltran-Aguilar E, Barker L, Canto M, et al. Surveillance for dental caries, dental sealants, tooth retention, edentulism, and enamel fluorosis–United States, 1988-1994 and 1999-2002. MMWR Surveill Summ. 2005;26:1–43.
- Young DA, Novy BB, Zeller GG, et al. The American Dental Association Caries Classification System for Clinical Practice: A report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2015;146:79–86.
- Featherstone JD. The caries balance: the basis for caries management by risk assessment. Oral Health Prev Dent. 2004;1(2 Suppl):259–264.
- Ramos-Gomez F, Ng MW. Into the future: keeping healthy teeth caries free: pediatric CAMBRA protocols. J Calif Dent Assoc. 2011;39:723–733.
- Hurlbutt M, Young DA. A best practices approach to caries management. J Evid Based Dent Pract. 2014;14(Suppl):77–86.
- Jenson L, Budenz AW, Featherstone JD, Ramos-Gomez FJ, Spolsky VW, Young DA. Clinical protocols for caries management by risk assessment. J Calif Dent Assoc. 2007;35:714–723.
- Featherstone JDB, Horst JA. Fresh approach to caries arrest in adults. Decisions in Dentistry. 2015;1(1):36–44.
- Rosenblatt A, Stamford TC, Niederman R. Silver diamine fluoride: a caries “silver-fluoride bullet.” J Dent Res. 2009;88:116–125.
- Horst JA, Ellenikiotis, H., Milgrom, PM. UCSF Protocol for Caries Arrest Using Silver Diamine Fluoride: Rationale, Indications, and Consent. J Calif Dent Assoc. 2016;44:17–28.
- Knight GM, McIntyre JM, Craig GG, Mulyani, Zilm PS, Gully NJ. Inability to form a biofilm of Streptococcus mutans on silver fluoride- and potassium iodide-treated demineralized dentin. Quintessence Int. 2009;40:155–161.
- Mei ML, Li QL, Chu CH, Yiu CK, Lo EC. The inhibitory effects of silver diamine fluoride at different concentrations on matrix metalloproteinases. Dent Mater. 2012;28:903–908.
- Mei ML, Ito L, Cao Y, Li QL, Lo EC, Chu CH. Inhibitory effect of silver diamine fluoride on dentine demineralisation and collagen degradation. J Dent. 2013;41:809–817.
- Llodra JC, Rodriguez A, Ferrer B, Menardia V, Ramos T, Morato M. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36-month clinical trial. J Dent Res. 2005;84:721–724.
- Zhi QH, Lo EC, Lin HC. Randomized clinical trial on effectiveness of silver diamine fluoride and glass ionomer in arresting dentine caries in preschool children. J Dent. 2012;40:962–967.
- Chu CH, Lo EC, Lin HC. Effectiveness of silver diamine fluoride and sodium fluoride varnish in arresting dentin caries in Chinese pre-school children. J Dent Res. 2002;81:767–770.
- Yee R, Holmgren C, Mulder J, Lama D, Walker D, van Palenstein Helderman W. Efficacy of silver diamine fluoride for Arresting Caries Treatment. J Dent Res. 2009;88:644–647.
- Tan HP, Lo EC, Dyson JE, Luo Y, Corbet EF. A randomized trial on root caries prevention in elders. J Dent Res. 2010;89:1086–1090.
- Duffin S. Back to the future: the medical management of caries introduction. J Calif Dent Assoc. 2012;40:852–858.
- Shirtcliff M. Testimony given to the Oregon state legislature. Available at: olis.leg.state.or.us/liz/2013R1/Downloads/CommitteeMeetingDocument/7702. Accessed June 8, 2016.
- Mickenautsch S, Yengopal V. Caries-preventive effect of high-viscosity glass ionomer and resin-based fissure sealants on permanent teeth: a systematic review of clinical trials. PLoS One. 2016;11:e0146512.
- Ngo H, Ruben J, Arends J, et al. Electron probe microanalysis and transverse microradiography studies of artificial lesions in enamel and dentin: a comparative study. Adv Dent Res. 1997;11:426–432.
- Strom K, Ronneberg A, Skaare AB, Espelid I, Willumsen T. Dentists’ use of behavioural management techniques and their attitudes towards treating paediatric patients with dental anxiety. Eur Arch Paediatr Dent. 2015;16:349–355.
- Frachella JC. Stainless steel crowns. J Am Dent Assoc. 2015;146:495–496.
- Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimal intervention dentistry—a review. FDI Commission Project 1-97. Int Dent J. 2000;50:1–12.
From Dimensions of Dental Hygiene. July 2016;14(07):61–64.
