Activate Alternative Fulcrums
The use of alternative fulcrums enables dental hygienists to apply the multidirectional strokes necessary to remove deposits from deep periodontal pockets.
Multidirectional strokes are activated in deep periodontal pockets using both traditional and alternative fulcrums, including opposite arch and extraoral fulcrums. Scaling techniques strictly limited to intraoral same-arch fulcrums originated in an era when dental hygienists scaled only supragingivally. These techniques alone are not adequate for thorough debridement or root planing of surfaces in deep pockets laden with heavy calculus and biofilm.
Over time, the responsibilities of dental hygienists have expanded to include the treatment of patients with attachment loss and deep periodontal pockets. As such, advanced techniques must be incorporated to meet current patient needs. The use of multidirectional, short, overlapping strokes for deep pockets requires that clinicians use a variety of instruments with alternative fulcrums. Mastery of these alternative fulcrums is important for both practitioners and students. Schools that teach advanced instrumentation techniques earlier in the curriculum are better able to prepare their graduates for the rigors and realities of clinical practice.
EXTRAORAL FULCRUMS
Extraoral or alternative fulcrums are essential for effective debridement or root planing in pockets deeper than 4 mm because they facilitate optimal access and correct blade adaptation and angulation. The use of extraoral fulcrums enables clinicians to consistently maintain the blade on the tooth, with ideal angulation and adaptation throughout each overlapping stroke, which is activated from the base of the pocket toward the gingival margin. Advanced fulcrums allow clinicians to reach up or down into deep pockets that are difficult to access with conventional, close intraoral fulcrums. Standard intraoral fulcrums offer stable power for shallow, healthier areas; however, when periodontal pockets become deeper, traditional fulcrums and positions can limit the reach and length of the stroke.1
By extending the grasp on the instrument handle and using an opposite arch or extraoral handrest farther away from the working area, the instrument blade can be more easily inserted to the pocket depth and properly adapted to the root surface before a series of strokes is begun. Ideal blade angulation is noted when the lower shank of a Gracey curet is parallel to the tooth surface being scaled and the lower shank of a universal curet is tilted slightly toward the surface being scaled. At this point, the blade is closed to 70° to 80° for proper angulation.2
PAIN CONTROL
An important prerequisite for deep scaling of periodontal pockets with multidirectional strokes is adequate pain control. Choose block anesthesia whenever necessary to achieve profound pulpal and soft tissue anesthesia before proceeding with initial ultrasonic and/or hand instrumentation. Most patients with periodontitis experience discomfort when hand instruments are inserted deeply and firm strokes are used, or when medium to high power is applied during ultrasonic scaling to remove tenacious calculus.
SEQUENCE
In the presence of large calculus deposits, multidirectional strokes should be implemented with an ultrasonic device tuned to medium-high to high power. Break up ledges or large pieces of calculus with vertical probe-like strokes first, followed by a combination of very short, overlapping, vertical, oblique, and horizontal strokes by carefully adapting the terminal 1 mm to 3 mm of the ultrasonic insert/tip to all surfaces. Remove as much calculus as possible with multidirectional strokes over every square millimeter of the tooth or root surfaces before progressing to either firm scaling strokes and/or lighter finishing strokes with hand instrumentation.
To illustrate complex fulcrums and the correct positioning for advanced instrumentation, the following descriptions concentrate on the mandibular right posterior teeth. The first step is to place the patient in a semi-supine position with the mandible at approximately 45° to the floor. Second, a right-handed clinician should be standing on the left side of the chair to gain optimal access, sight, and leverage for scaling deep mandibular pockets. These fulcrums can be used with universal curets, Gracey curets, or mini-bladed Gracey curets.
MESIAL SURFACES
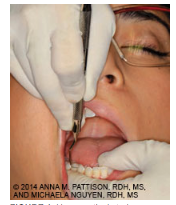
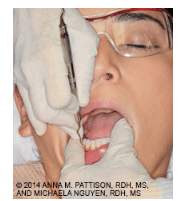
To activate vertical or oblique strokes on the mesial surfaces of the right mandibular posterior teeth from the buccal aspect, approach by standing at 1 o’clock with the patient in a semi-supine position (Figure 1). The mandible is approximately 45° to the floor and the patient is positioned at waist level to the clinician. Fulcrum using an intraoral, opposite arch rest on the buccal-occlusal surfaces of the maxillary right premolars or the maxillary right first molar just above the right mandibular molars. Extend the instrument toward the mesial surfaces of the mandibular right molars for access to the base of deep pockets. Initiate the strokes by applying pressure with the index finger while simultaneously pulling up with the entire hand. This fulcrum will maintain correct blade angulation and adaptation as the instrument is positioned at the base of the pocket and then pulled up with overlapping strokes to the contact.
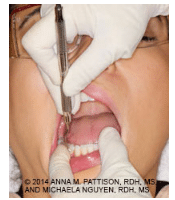
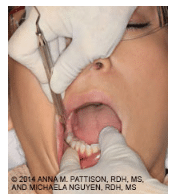
The fulcrum seen in Figure 2 is the same as in Figure 1—but in this case, the clinician stands on the left side of the patient with the hand approaching from 3 o’clock and the clinician’s body facing the patient at 5 o’clock. Use an intraoral, opposite arch fulcrum resting on the buccal surfaces of the maxillary teeth. This position permits the thumb to apply firm lateral pressure directly against the mesial surfaces of the mandibular right posterior teeth. This also enables more powerful strokes with constant correct angulation and adaptation from the base of a deep pocket up to the contact. Initiate the strokes by pulling up with the entire hand while simultaneously applying pressure with the thumb to keep the blade from closing down and burnishing calculus.3
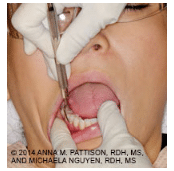
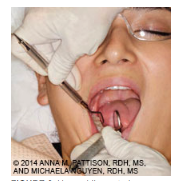
Figure 3 demonstrates the same approach as the 5 o’clock position described above, but the fulcrum rests extraorally on the skin of the patient’s cheek overlying the zygoma for a firm, stable fulcrum. This maxillary extraoral rest enables the blade to extend into the deep mesial pockets on the mandibular right posterior teeth.3
To use the finger-on-finger fulcrum as seen in Figure 4, position the patient in a semi-supine position and sit or stand in a 1 o’clock position. Place the nondominant (left) index finger into the right mandibular vestibule and fulcrum on the index finger. Align the instrument with the long axis of the tooth, insert the blade on the mesial surface, and establish correct angulation before scaling upward in a coronal direction.
OTHER SURFACES
Each of the aforementioned fulcrums can also be used when approaching the same mesial surfaces from the lingual aspect, with the exception of the finger-on-finger fulcrum. Also, all of the fulcrums described for the mesial surfaces are exactly the same for the distal, buccal, and lingual surfaces, except for the finger-on-finger fulcrum. Whether approaching from the buccal aspect (Figure 5) or the lingual aspect (Figure 6), the positions and the fulcrums are similar.
The alternative opposite arch intraoral fulcrum on the maxillary right premolar or maxillary right first molar that was shown for the mesial surfaces may also be used for the buccal and lingual surfaces, except for the finger-on-finger fulcrum.
SUMMARY
Clinicians need not be afraid of incorporating alternative fulcrums into practice. With these fulcrums, multidirectional, overlapping strokes can reach easily and effectively into deep periodontal pockets.
REFERENCES
- Pattison AM. Trends in instrumentation. Dimensions of Dental Hygiene. 2005;3(7):26–27.
- Pattison AM, Matsuda S, Pattison G. Extraoral fulcrums. Dimensions of Dental Hygiene. 2004;2(10):20–23.
- Kiehl N. Instrumenting periodontally involved anterior teeth. Dimensions of Dental Hygiene. 2012;10(11):26–29.
From Dimensions of Dental Hygiene. May 2014;12(5):24,26,28.

{kind=link}