Sunstar Spotlight: Gender Gap
Differences in the way chronic craniofacial-oral-dental pain presents in men and women may affect diagnosis, management, and treatment.
Introduction

Manager, Professional Relations Sunstar Americas Inc
According to the National Institute of Dental and Craniofacial Research, temporomandibular joint and muscle disorders are the most common causes of chronic facial pain. Study into craniofacial-oral-dental pain has provided clues on the etiology of the problem and offered suggestions as to how oral health professionals can better help patients manage the numerous complications that accompany recurrent pain.
This month’s edition of Sunstar Spotlight features Harold C. Slavkin, DDS, who has spent his career focused on the study of craniofacial pain and molecular
biology. With his vast understanding of these areas, Slavkin sheds new light on the difficulties involved in diagnosing and treating patients with craniofacial-
oral-dental pain. Through this fascinating look at encoding genes and the function of cranial nerves, oral health professionals will be left with a greater understanding of this challenging subject.
Margaret Jacob, PhD, a professor of history at the University of California, Los Angeles, wrote, “When one is in chronic pain, the future becomes dim, best left without fantasy, or possibly to be dreaded. The past becomes a story about when the pain began, when it got worse, how bad it is today.”1 Her words eloquently refer to chronic pain’s damaging effects on a variety of human functions, emotions, and financial resources. Pain is one of the most common reasons patients seek medical treatment.
Gender plays a role in chronic pain, coloring pain perception, treatment utilization, and metabolism, and responses to sedatives, analgesics, and nonsteroidal anti-inflammatory medications. In 2011, the Institute of Medicine published a report on the public impact of chronic pain titled “Relieving Pain in America.” This study discovered that not only did women appear to experience pain more often, but their accounts of pain were more likely to be dismissed by male health care professionals.2
About 25% of American adults experience chronic pain, and a disproportionate number are women.2 Pain conditions—including migraine and tension-type headaches, craniofacial-oral-dental pain, and abdominal pain—are common for many, and population-based studies indicate higher prevalence rates among adult women than adult men. More often than not, women who present with severe chronic oral-facial pains are considered “emotional” and, therefore, treated with sedatives rather than appropriate analgesics.
The gender gap is particularly relative when considering chronic craniofacial pain, such as oral facial myalgia. Because women experience hormonal cycles and have smaller organs and higher body fat composition than men, drugs are metabolized differently in their bodies. There are also subtle changes in deoxyribonucleic acid (DNA), so-called genetic variances or single nucleotide polymorphisms, between men and women, which in turn reflect differences in drug utilization, pharmacokinetics, and metabolism. Various genes and genetic variants encoding opioid receptors are now known to function in the sensitivity, perception, and expression of chronic oral facial pain. This article will focus on a number of key issues central to the diagnosis, management, and understanding of chronic craniofacial-oral-dental pain.3–9
PAIN PERCEPTION

FIGURE 1. ERAXIO: ISTOCKPHOTO / GETTY IMAGES
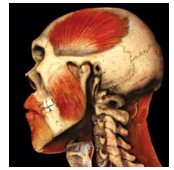
The craniofacial-oral-dental complex is the sensory capitol of the human condition. Twelve pairs of cranial nerves extend from various regions of the brain, through foramina (holes) in the skull, to provide sensory and/or motor functions (Figure 1). This architecture enables smell, vision, eye movements (emotions), eating and swallowing, taste, speech, touch and pain, facial expression, and hearing. Most of these cranial nerves innervate structures in the craniofacial-oral-dental complex. The vagus nerve has functions that extend to innervating organs in the thorax and the abdomen. The peripheral nervous system, in turn, consists of the 12 pairs of cranial nerves plus the 31 pairs of spinal nerves that extend from the spinal cord.
Several of these paired cranial nerves are important to understanding the etiology, diagnosis, and management of chronic craniofacial pain. The fifth or trigeminal cranial nerve transmits sensations from the face to the brain. The extension of the fifth cranial nerve is the trigeminal ganglia from which three branches extend: ophthalmic, maxillary, and mandibular. These branches connect nerves from the brain to various locations of the face, such as the eye region (forehead, eyebrows, eyelids), midface (maxilla), and lower face (mandible). The trigeminal is responsible for transmitting sensations to the mouth, teeth, face, and nasal cavity. It also controls the muscles of mastication (Figure 2).
Trigeminal neuralgia occurs when a blood vessel, vein, artery, or tumor places pressure at the base of the brain. In rare circumstances, trigeminal neuralgia can be caused by a brain tumor that compresses the fifth nerve. Symptoms include bouts of severe stabbing facial pain, often described as a sudden burst, that is triggered by touching, chewing, swallowing, or talking. Treatments may include anti-convulsion medications, muscle relaxants, sedatives, analgesics, opioids, and nonsteroidal anti-inflammatory medications. Surgery and alcohol injections are additional clinical strategies.
Trigeminal myalgia affects the maxillary branch of the trigeminal nerve, most often in middle-aged and older women. In young women, trigeminal myalgia is often associated with multiple sclerosis. In general, imaging of the craniofacial complex is necessary to rule out the possibility of a brain tumor. Trigeminal neuralgia signs and symptoms vary in intensity, duration, and frequency. The condition is not life-threatening, but some patients may become suicidal due to the resultant signs and symptoms.
The seventh or facial cranial nerve provides motor innervation for the muscles of facial expression. It also carries autonomic nerve fibers to the mucous glands of the nose and paranasal sinuses, the lacrimal gland (tear production), and two of the three salivary glands (submandibular and sublingual glands). The seventh cranial nerve also conveys the sense of taste from the anterior two-thirds of the tongue while supplying preganglionic parasympathetic fibers to several head and neck ganglia.
Acute facial nerve paralysis, which is manifested by facial paralysis, can occur when the facial cranial nerve is damaged. Bell’s palsy is one type of idiopathic acute facial nerve paralysis and often results from a viral infection or Lyme disease. Iatrogenic Bell’s palsy can also be caused by an incorrectly placed inferior alveolar nerve block during dental anesthesia.10
Oral health professionals are keenly interested in the regional distribution of cranial nerves five (trigeminal) and seven (facial), along with patterns of patient narratives describing the timing, duration, and magnitude of their chronic craniofacial-oral-dental pain. The neuroscience mechanisms of chronic pain are important, as is selecting the most effective treatment plan to manage discomfort. One approach is to utilize clinical assays, based on either heat or electrical detection thresholds, which discriminate between pain originating from temporomandibular joint (TMJ arthralgia) vs pain originating from craniofacial muscles (myalgia).
NEUROSCIENCE MECHANISMS
Mechanical, thermal, and chemical stimuli to the craniofacial-oral-dental complex are detected by nerve endings called nociceptors, which are located in the skin and on the internal surfaces, including the periosteum; joint surfaces, such as the TMJ; and muscles of mastication and facial expression.
Nociception is the neuronal process of encoding and processing noxious stimuli. The concentration of nociceptors varies throughout the body and between men and women. Nociceptors are free nerve endings with cell bodies outside the brain or spinal cord. Each nociceptor has a threshold of minimum stimulation intensity before it will trigger a signal. Once the threshold is reached, a signal is passed along the axon of the neuron cell into the brain or spinal cord. In some conditions, excitation of pain fibers becomes greater as the pain stimulus continues, leading to hyperalgesia or increased sensitivity to pain. Nociceptive neurons generate trains of action potentials in response to painful stimuli, and the frequency of firing signals the intensity and duration of the pain.4,5
Men and women possess an endogenous analgesia system consisting of scattered neurons that produce three opioids: beta-endorphin, met- and leu-enkephalins, and dynorphins. These opioids can be supplemented with analgesic drugs to regulate nociception and pain. They act as neurotransmitters and neuromodulators at three major classes of receptors and produce analgesia. Like the endogenous opioids, the opioid drugs or opiates act at these same receptors to produce analgesia as well as undesirable side effects. The effectiveness of the endogenous analgesia system is influenced by environmental factors, such as hormone levels, and genetic variations between men and women. Curiously, the endogenous opioid system is significant in mediating the complex social behaviors that form the basis of stable, emotionally committed relationships. These factoids help health care professionals effectively diagnosis and manage pain.
PHARMACOGENOMICS AND PAIN MANAGEMENT
 The double-helix form for DNA was discovered 61 years ago by scientists who found that it regulated significant biological processes. The United States government initiated the Human Genome Project 26 years ago to discover and map each of the functioning genes within human somatic cells. Ten years ago, the human genome was completed, and, in 2013, the complete genome of an individual could be entirely sequenced and annotated within 24 hours at a cost of approximately $1,000 per person.
The double-helix form for DNA was discovered 61 years ago by scientists who found that it regulated significant biological processes. The United States government initiated the Human Genome Project 26 years ago to discover and map each of the functioning genes within human somatic cells. Ten years ago, the human genome was completed, and, in 2013, the complete genome of an individual could be entirely sequenced and annotated within 24 hours at a cost of approximately $1,000 per person.
Today, it is known that the average adult consists of 10 trillion somatic cells. Each of these cells contains the human genome in the nucleus—23 pairs of chromosomes containing 21,000 (plus) functional genes and 19,000 pseudogenes encoded within DNA. In addition, each contains organelles called mitochondria that also contain DNA. This DNA encodes a number of functional genes inherited exclusively from mothers. In addition, individuals have a human microbiome, which is 100 times larger than the number of somatic cells.
The double helix macromolecule called DNA consists of four nucleotides or bases (A, adenosine; T, thymidine; C, cytosine; and G, guanosine). These four letters—A, T, C, and G—are arranged in a number of combinations to spell the correct base sequence that characterizes each gene and each gene’s products (messenger ribonucleic acid [RNA], transfer RNA, ribosomal RNA, and proteins). These units of three letters are termed a codon, which specifies each amino acid that is found in precise positions within proteins. Patterns of four letters are found within the upstream regions that contain enhancers and promoters, within exons that represent the coding region of a gene, and within introns that are found between exons. There also is a stop codon (AAA) that signifies the end of a functional gene.
It was once asserted that one gene was transcribed into one mRNA, which in turn was translated into one protein. If this were the case, the number of functional genes would equal the total number of proteins (proteome) made by an individual. More recent evidence has shown that genes use a process called alternative splicing, whereby a single gene produces multiple mRNAs, which in turn are translated into multiple proteins (often eight to 10 different isotypes from a single gene).11
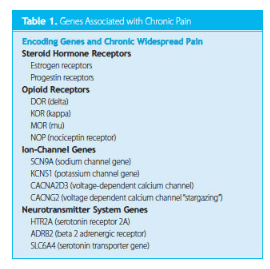
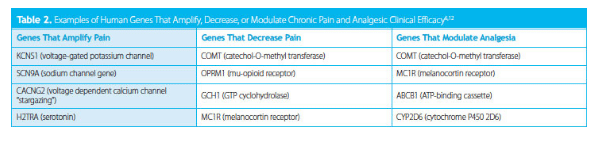
The nucleus of every somatic cell contains 23 pairs of chromosomes, which are made from DNA, histone proteins, and nonhistone proteins (called chromosomal proteins). There are four major subtypes of opioid receptors located on chromosomes 1, 6, 8, and 20. These transmembrane nociceptors and nociception receptors are located with peripheral sensory neurons and provide endogenous analgesia, as well as bind to pharmaceutical ligands to achieve analgesia. In addition, a number of other gene types are also associated with chronic pain, including adrenergic receptors, serotonin receptors, voltage-gated sodium, and potassium channel receptors (Table 1 and Table 2).6,12
![]() GENOMICS AND PAIN MANAGEMENT
GENOMICS AND PAIN MANAGEMENT
In September 2006, members of the Sex, Gender and Pain Special Interest Group of the International Association for the Study of Pain13 met to discuss and reach consensus on the following issues:
- What is known about sex and gender differences in pain and analgesia?
- What are the best practice guidelines for pain research with respect to sex and gender?
- What are the crucial questions to address in the near future?
The patterns of pain prevalence by age and sex vary for different pain conditions. The most significant differences by age and sex follow puberty, with women experiencing significantly more pain issues than men. Some pain conditions in women, such as migraine headaches and TMJ, decline in prevalence after the age of 40, whereas others, such as joint pain and fibromyalgia, appear to persist into old age.
The consensus report highlighted that there is a significant sex-dependent genetic association with opioid analgesia in women. Specifically, women who possess two variant MC1R alleles display greater analgesia responses to pentazocine on thermal and ischemic pain stimuli compared to men and women with one or two or no variant MC1R alleles. Other studies have discovered that mixed action (kappa and mu) opioid drugs produce greater analgesia after third molar extraction in women than in men. A number of studies provide evidence that hormones affect pain perception, pain threshold, and responses to analgesia. Further, studies also demonstrate that pain chronicity contributes to increased sex differences in pain and analgesia.13
Although significant progress is being made in the diagnosis and management of chronic craniofacial pain, a number of areas still need to be addressed. Clinical trial methods, analysis, and reporting must report positive as well as negative findings as a function of age, sex, and ethnicity. In medication clinical trials, sufficient numbers of men and women must be included. Federal, state, and local governments, as well as the pharmaceutical industry and nonprofit biomedical organizations, should serve as advocates for advancing the knowledge of gender biology.
REFERENCES
- Jacob M. Historians with pain. Perspectives on History. Available at: historians.org/publications-and-directories/perspectives-on-history/november-2005/historians-with-pain. Accessed April 14, 2014.
- Institute of Medicine United States Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: a Blueprint for Transforming Prevention, Care, Education, and Research. Washington, DC: National Academies Press; 2011.
- Dao TT, LeResche L. Gender differences in pain. J Orofac Pain. 2000;14:169–184.
- Sato H, Droney J, Ross J, et al. Gender, variation in opioid receptor genes and sensitivity to experimental pain. Mol Pain. 2013;9:48–57.
- Cairns BE. The influence of gender and sex steroids on craniofacial nociception. Headache. 2007;47:319–324.
- James S. Human pain and genetics: some basics. British Journal of Pain. 2013;7(4):171–178.
- Slavkin HC. Distinguishing Mars from Venus: emergence of gender biology in health and disease. J Am Dent Assoc. 1998;129:357–361.
- Steglitz J1, Buscemi J, Ferguson MJ. The future of pain research, education, and treatment: a summary of the IOM report “Relieving pain in America: a blueprint for transforming prevention, care, education, and research.” Transl Behav Med. 2012;2:6–8.
- Shinal RM, Fillingim RB. Overview of orofacial pain: epidemiology and gender differences in orofacial pain. Dent Clin North Am. 2007;51:1–18.
- Tzermpos FH, Cocos A, Kleftogiannis M, Zarakas M, Iatrou I. Transient delayed facial nerve palsy after inferior alveolar nerve block anesthesia. Anesth Prog. 2012;59: 22–27.
- Brown TA. Understanding a genome sequence. In: Genomes. 2nd ed. Oxford, England: Wiley-Liss; 2002.
- Binder A1, May D, Baron R, et al. Transient receptor potential channel polymorphisms are associated with the somatosensory function in neuropathic pain patients. PLoS One. 201129;6:e17387.
- Greenspan JD1, Craft RM, LeResche L, et al. Studying sex and gender differences in pain and analgesia: a consensus report. Pain. 2007;132(Suppl 1):S2–S45.
From Dimensions of Dental Hygiene. May 2014;12(5):19–22.

{kind=link}