 MILOSLJUBICIC / ISTOCK / THINKSTOCK
MILOSLJUBICIC / ISTOCK / THINKSTOCK
The Search for Consensus
Even though dental hygienists have been successfully administering local anesthesia for more than 40 years, consensus on national education standards and utilization guidelines has yet to be achieved.
The roles of dental hygienists continue to expand and comprise clinicians, educators, patient managers, and community oral health advocates.1 As more responsibilities are delegated to nondentists, skill sets and scopes of practice will be redefined. One such skill that is widely used by dental professionals is local anesthesia administration (LAA). Although dental hygienists have been providing LAA in the United States in a safe and effective manner for more than 40 years, there is no national scope of practice that includes LAA. A lack of consensus regarding educational requirements and optimal LAA methodologies also remains. This article will explore relevant aspects of LAA within the dental hygienist’s scope of practice.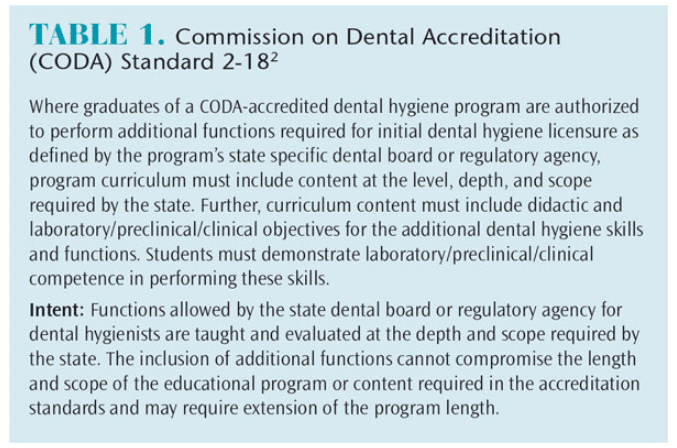
EDUCATION AND TRAINING
Education and training of LAA commonly occurs via one of two pathways: dental hygiene program/school curriculum or continuing education certification courses. Competence for permit or licensing is reflected within each state’s rules and regulations (dental practice act). In addition, Standard 2-18 of the Commission on Dental Accreditation (CODA) states that dental hygienists must be educated to perform all tasks in a state’s dental practice act (Table 1).2 How each program develops its local anesthesia curriculum within this standard is at the school’s discretion.
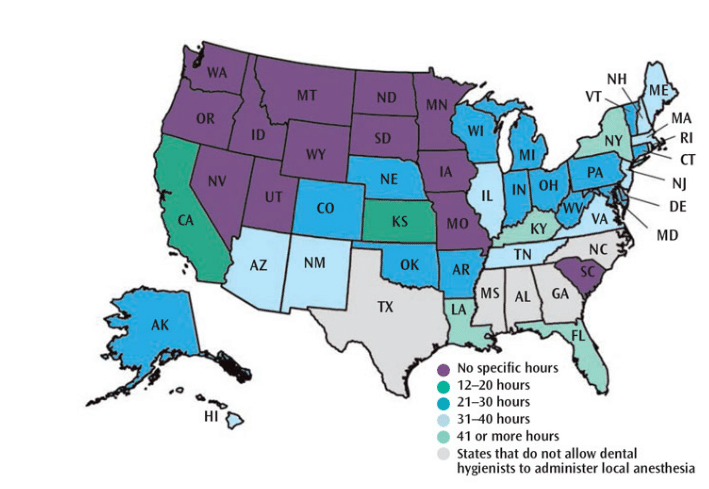
As seen in Figure 1, a great deal of variation exists between states in the number of instruction hours required before dental hygienists can become licensed in LAA. The hours required range from zero to 72. As such, it is no surprise that significant disparities in didactic and clinical requirements, supervision levels, and LAA methodologies exist.3
The American Dental Hygienists’ Association compiles data on LAA rules and regulations for each state. When comparing these data, it is clear that no national education standard exists. Thus, it may be helpful to consider the states with the longest history of dental hygienists providing LAA. Five states have allowed dental hygienists to provide LAA for 40-plus years: Washington, Oregon, Idaho, New Mexico, and Missouri. Of these five states, only New Mexico requires a minimum number of instruction hours (34 hours) while the other four have no requirements. The seven states with less than 10 years of LAA experience by dental hygienists—Indiana, Ohio, New Jersey, Maryland, Pennsylvania, Virginia, and Florida—require a minimum number of training hours, ranging from 28 to 60. Florida, the most recent state to permit dental hygienists to provide LAA, requires 60 hours of instruction. The average number of hours required for these seven states is 33. When comparing states that limit LAA to infiltration only, similar discrepancies are seen. For example, New York requires 45 hours of instruction, while South Carolina has no minimum requirement. In comparison, the national average for total required instruction (including both didactic and clinical hours when applicable) is 22 hours.
Unfortunately, variation in state dental anesthesiology regulation is also common.4 Discrepancies in state regulations may adversely affect portability of licensure, patient experience, and dental practices’ financial models. Additionally, variations in the initial licensure of dental hygienists with LAA training may be confusing for newly graduated dental hygienists.5 For many, especially those who take regional board exams, LAA competencies may not even be assessed.
Rules and regulations governing LAA are determined by state dental boards. States have their own requirements and they often necessitate different training and documentation such as proof of passing a regional board examination, signed affidavit by a supervising dentist, and/or graduation from an accredited dental hygiene school with a verified LAA curriculum. This not only poses challenges for dental hygiene professionals moving across state lines, but also for the credentialing bodies themselves.4 Thorough review of the dental practice act is imperative prior to engaging in practice.
PRACTICE CHARACTERISTICS
Currently, 44 states and the District of Columbia include LAA within their dental hygiene scopes of practice. A national survey completed in 2011 revealed that the majority of dental hygiene respondents (59.5% of 432 survey participants) administered local anesthesia.6 This study also demonstrated that the majority of respondents administered anesthesia for procedures to be performed by a dentist (58.4% of 257 survey participants). Practice settings can influence the number and types of injections administered by dental hygiene professionals. Clinicians working in periodontal practices and those in public health settings reported more frequent use of LAA.6 The small number of dental hygiene professionals employed by endodontists may perform LAA as their primary task.7,8
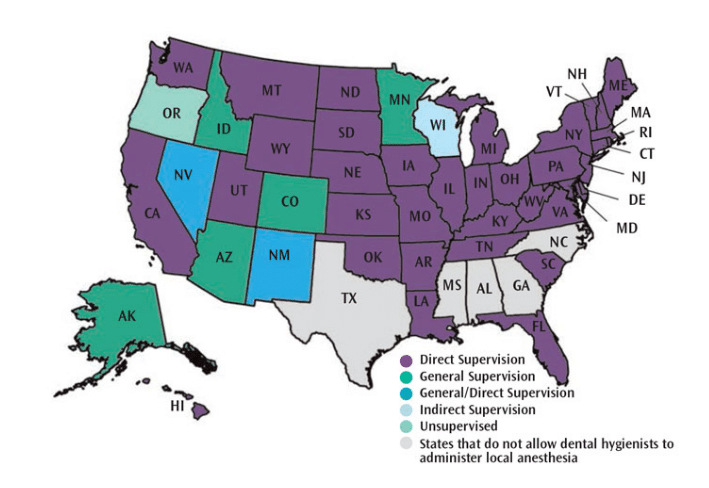
Figure 2 demonstrates the type of supervision required for dental hygienists during LAA by state. Supervision is usually described as:
Direct: a supervising dentist is on the premises, has diagnosed the condition, authorized the procedure, and evaluates the completion of the procedure [some states use the term “indirect” with a similar definition]
General: a supervising dentist has authorized the procedure and completed a diagnosis but does not physically need to be on the premises
Direct/general: This level of supervision varies depending on the practice activity or the type of licensure/certification of the dental hygiene professional9
In the six states where LAA is provided under general supervision (Alaska, Idaho, Nevada, Colorado, Arizona, and Minnesota), the procedures are delegated to dental hygienists as part of approved treatment plans. In these settings, dental hygiene professionals are held to the same standards of competency, safety, and appropriate responses to adverse reactions as set forth by state regulations and CODA standards (for training programs). For example, CODA Standard 2-17 mandates that dental hygiene professionals be competent in providing appropriate life support measures for medical emergencies that may be encountered in dental hygiene practice (Table 2).2 This directly applies to all sites where dental hygienists administer local anesthesia in accordance with state regulations.
SAFETY AND EFFECTIVENESS
A significant record of safety of LAA by dental hygiene professionals is documented in the published scientific literature.5,10,11 Based on 1990 and 2005 surveys, no formal complaints were reported regarding dental hygienists engaged in LAA.12,13 Few significant adverse issues have been reported during the 300 million plus dental-related local anesthetic injections administered each year. Both dentists and dental hygienists have a remarkable record of safety.14,15
Data on effectiveness demonstrate that dental hygienists obtain the training to administer local anesthesia with high levels of success.5,10,11 Reported anesthesia success rates following the administration of an intraoral anesthetic agent range from 86% to 97%, with variations for injection type and technique similar to those seen throughout the dental profession.5,13,15 In a study of Arkansas dentist employers, investigators reported 92% of respondents were satisfied with dental hygienists’ abilities to administer local anesthesia.16 In a study evaluating school-based dental care, no significant differences in complication rates were found when dentists and dental hygienists were compared.17
DEVELOPING A NATIONAL CONSENSUS
While seven states (Alaska, Colorado, Idaho, Minnesota, Nevada, New Mexico, and Oregon) permit dental hygienists to engage in LAA at some level of general supervision, six states (Delaware, North Carolina, Mississippi, Alabama, Georgia, and Texas) continue to exclude local anesthesia as part of the dental hygiene scope of practice. In 2015, legislation was introduced in Texas to change the scope of practice; however, the bill did not gain enough support to advance through the legislature.18
Hyperbole, concern for patient safety, and politics are at play whenever regulatory officials consider expanding dental hygienists’ scopes of practice. Moreover, underutilization of expanded function auxiliaries occurs more often in dentistry than in other health care disciplines.19,20 Previous investigators have cited insufficient experience and education regarding team-based patient care models as reasons for their underutilization in dentistry.19,21,22
PRACTICE IMPLICATIONS
Dental hygiene professionals engaged in LAA may improve their dental practices’ financial viability and sustainability. Surveys have demonstrated that a majority of dentists reported that delegating LAA to dental hygienists provides benefits such as enhanced patient satisfaction and increased productivity.5,10,16 A better understanding of these effects requires additional research.21–25
CONCLUSION
Dental hygienists have demonstrated they can proficiently and safely administer local anesthesia. While much progress has occurred over the past 40 years, there remains no national education standard or utilization consensus regarding LAA. The entire profession of dentistry would likely benefit from a consensus monogram endorsed by both organized dentistry and dental hygiene that provided guidelines regarding education requirements and the use of LAA. In an era of health care paradigm shifts, the ability to increase practice efficiencies and improve treatment outcomes and patient experience by allowing dental hygiene professionals to provide LAA suggests that the time is right for national consensus.
References
- Darby ML, Walsh M. Dental Hygiene Theory and Practice. 3rd ed. Philadelphia: Saunders; 2009.
- Commission on Dental Accreditation. Accreditation Standards for Dental Hygiene Education Programs. Available at: ada.org/~/media/CODA/ Files/dh.pdf?la=en. Accessed February 16, 2016.
- American Dental Hygienists’ Association. Local Anesthesia by Dental Hygienists: State Chart. Available at: adha.org/resources-docs/7514_Local_Anesthesia_Requirements_by_State.pdf. Accessed February 16, 2016.
- Boynes SG. Dental Anesthesiology: A Guide to the Rules and Regulations of the United States. Chicago: American Dental Society of Anesthesiology; 2013.
- Boynes SG, Zovko J, Peskin RM. Local anesthesia administration by dental hygienists. Dent Clin N Am. 2010:54;769–778.
- Boynes SG, Zovko J, Bastin MR, et al. Dental hygienists’ evaluation of local anesthesia education and administration in the United States. J Dent Hyg. 2011;85:67–74.
- Gutman ME, Gutmann JL. The dental hygienist as a co-therapist in endodontic practice. J Endodon. 1999;25:272–274.
- Waldman HB, Feigen ME. Endodontists in a period of improving dental economics and changing realities of practice. J Endodon. 1990;16:179–181.
- American Dental Association, Department of State Government Affairs. Expanded Functions for Dental Assistants. Available at: aapd.org/assets/1/7/StateLawsonDAs.pdf. Accessed February 16, 2016.
- Anderson JM. Use of local anesthesia by dental hygienists who completed a Minnesota CE course. J Dent Hyg. 2002;76:35-46.
- Lobene RR. The Forsyth Experiment. Boston: Harvard University Press; 1979.
- Scofield JC, Gutmann ME, DeQald JP, et al. Disciplinary actions associated with the administration of local anesthetics against dentists and dental hygienists. J Dent Hyg. 2005;79:8.
- Sisty-Lepeau N, Boyer EM, Lutjen D. Dental hygiene licensure specifications on pain control procedures. J Dent Hyg. 1990;64:179–185.
- Malamed SF. Handbook of Local Anesthesia. 5th ed. St Louis: Mosby; 2004.
- Bassett K, DiMarco A, Naughton D. Local Anesthesia for Dental Professionals. ed. 2nd ed. Saddle River, New Jersey: Prentice Hall; 2014.
- DeAngelis S, Goral V. Utilization of local anesthesia by Arkansas dental hygienists, and dentists’ delegation/satisfaction relative to this function. J Dent Hyg. 2000;74:196–204.
- Boynes SG, Riley AE, Milbee S, et al. Evaluating complications of local anesthesia administration and reversal with phentolamine mesylate in a portable pediatric dental clinic. Gen Dent. 2013;61:70–76.
- Richardson AM. Dental hygiene and anesthesia: Even government is perplexed by doublespeak. Available at: dentistryiq.com/articles/2015/03/ dental-hygiene-and-anesthesia-even-government-is-perplexed-by-doublespeak.html. Accessed February 16, 2016.
- Blue CM, Funkhouser E, Riggs S, et al. Utilization of non-dentist providers and attitudes toward new provider models: Findings from the national dental practice-based research network. J Public Health Dent. 2013;73:237–244.
- National Rural Health Association. Recruitment and Retention of a Quality Health Workforce. Available at: ruralhealthweb.org/index.cfm? objectid=4076C0CD-1185-6B66-885EFC4618BEF23F. Accessed February 16, 2016.
- Leske GS, Leverett DH. Variables affecting attitudes of dentists toward the use of expanded function auxiliaries. J Dent Educ. 1976;40:79–85.
- Blue C, Phillips R, Born D, Lopez N. Beginning the socialization to a new workforce model: dental students’ preliminary knowledge of and attitudes about the role of the dental therapist. J Dent Educ. 2011;75:1465–1475.
- Edelstein BL. Examining whether dental therapists constitute a disruptive innovation in US dentistry. Am J Public Health. 2011;101:1831–1835.
- Widstrom E, Linna M, Niskanen T. Productive efficiency and its determinants in Finnish Public Dental Service. Comm Dent Oral Epidemiology. 2004;32:31–40.
- Wright JT, Graham F, Hayes C, et al. A systematic review of oral health outcomes produced by dental teams incorporating midlevel providers. J Am Dent Assoc. 2013;144:75–91.
From Dimensions of Dental Hygiene. March 2016;14(03):18,20–23.

{kind=link}
Please review states and update
Greetings! Very helpful advice in this particular article!
It’s the little changes that produce the largest changes.
Many thanks for sharing!