 WEBPHOTOGRAPHEER/ISTOCK/GETTY IMAGES PLUS
WEBPHOTOGRAPHEER/ISTOCK/GETTY IMAGES PLUS
The Intersection of Periodontal Maintenance and Ultrasonic Instrumentation
Site-specific ultrasonic instrumentation is key to achieving effective periodontal maintenance and supporting periodontal health.
Periodontal maintenance (PM) typically occurs at 2-, 3-, or 4 – month intervals for the life of the dentition and implant replacements for individuals with periodontitis.1 Evidence reveals that PM improves outcomes over time in relation to tooth loss and disease advancement.2–7 Integral to PM is selective removal of plaque biofilm and calculus, as well as root planing and implant debridement.1 It is important to complete PM appointments efficiently and effectively; therefore, ultrasonic instrumentation is often employed.
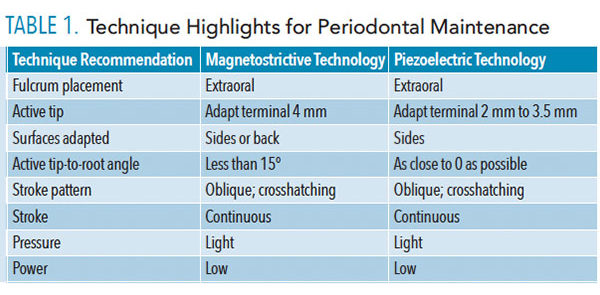
Effectiveness is dependent on assessing the periodontal conditions accurately, having adequate time for PM, and selecting appropriate therapy. Effective PM is achieved with the reduction of clinician signs of inflammation, such as the absence of erythema, edema, and bleeding on probing. Furthermore, reduced clinical attachment loss and a halt in advancing bone loss indicates effective treatment of the periodontium.8 Choosing multiple ultrasonic inserts or tips (UITs) for varying periodontal conditions and applying appropriate technique are critical to effectiveness (Table 1).
Periodontal evaluation includes recording sites of gingival inflammation (erythema and edema), bleeding on probing, periodontal pocket depth (PPD), clinical attachment level (CAL), furcation involvement, and mobility.1,9 An important consideration is the location of plaque biofilm and calculus type and texture within these conditions.

The presence of localized gingival inflammation, triggered by deposit reaccumulation and host response, indicates a need for site-specific debridement. In these areas, place the active tip of a curved UIT at the epithelial attachment and debride with oblique strokes toward the gingival margin (Figure 1). This method of removing lighter deposits supports the use of the side of the active tip instead of the point. Moving from the gingival margin apically encourages using the point on the root or the epithelial attachment, both of which should be avoided unless heavier calculus is being removed or narrow pocketing exists.

diameter and long ultrasonic insert/tip for
larger burnished/residual calculus.Figure provided by WILL CLEARY
The lack of bleeding on probing is positive in assessing health.8,10,11 If bleeding on probing is identified, inflammation is present; therefore, it is wise to instrument these areas with extra diligence.12 A careful examination of the bleeding on probing site(s) is indicated to determine if residual calculus or newly formed deposits are present. For either type, a site-specific UIT is needed. For example, bleeding in a deep and narrow 7 mm pocket signals that a very long UIT is indicated to reach the base of the pocket and its corresponding walls. If the calculus is burnished or residual, a wider diameter and long UIT is needed (Figure 2). A “top down” approach with a higher power setting is indicated due to the tenacious and larger deposit (Figure 2), followed by a thinner UIT. However, if light deposit is detected, a very thin diameter and long UIT suffices with the technique described above (Figure 3).
A deep PPD is defined as 5 mm or greater and warrants special attention. Deep pockets should be debrided with long, thin UITs to reach the epithelial attachment and adjacent topography. Depending on the surface of the deep pocket and its shape, either a long and thin curved or straight UIT will be indicated. Bathtub-shaped or curved and wide pockets are treated with a curved UIT to match the topography (Figure 4). A long and very narrow pocket will be best cared for with a straight design (Figure 5).
The CAL is critical to visualize during PM. Its path across the dentition relates to the type and shape of the pockets defined by the periodontal probing. The location of the CAL itself does not indicate a certain UIT; however, it does correlate to the UIT and technique needed for sites with PPD, furcation involvement, and mobility.

thin diameter and long ultrasonic insert/tip
for light deposit.Figure provided by WILL CLEARY
Furcation invasions result in curved root anatomy; therefore, a curved UIT is the best alternative for debridement. Focusing on adapting the sides of the working end that render the best results is important, especially in furcation anatomy. With magnetostrictive technology, the side or back of the tip is adapted (Figure 6). If the concave surface were to be adapted, the least productive surface would be utilized. With piezoelectric technology, the sides of the tip are adapted for efficacy. Mobility in itself does not necessitate a specialized UIT. Its existence, however, during PM might warrant stabilizing the tooth during ultrasonic instrumentation.

treated with a curved design.figure provided by WILL CLEARLY
SEQUENCING STRATEGIES
Planning the sequence of ultrasonic instrumentation aids in efficiency and effectiveness. For full-mouth debridement, select a set of three UITs for the entire dentition: either traditional curved right, left, and straight designs, or the ultrathin and longer version of these same three UITs. Complete the areas that adapt to a single right or left UIT. Change the UIT to the opposite curved design and complete the remainder of the posterior sextants. Last, use the straight UIT to complete the anterior teeth and any specific sites (Figure 2). If multiple periodontal parameters are present, further localized debridement is indicated. In these advanced cases, employ a long microultrasonic curved UIT and engage in site-specific therapy for deep pockets over 5 mm, furcation involvements, bleeding on probing sites, or such. For example, consider debridement of teeth #14, #15, #19, and #31 with 6 mm PPD and Class II furcations. If deep PPD exists at line angles, adjacent to a furcation entrance, or on the mesial of a premolar or molar, then change to the long microultrasonic straight UIT and debride. With this strategy of sequencing, local anesthesia, if indicated, can be delivered at site-specific areas prior to the first step of generalized debridement, allowing time for the teeth to be profoundly anesthetized. An alternative strategy is to perform the site-specific instrumentation first and lastly instrument the entire mouth. A periodontal endoscope would be a valuable tool for assessing site-specific areas during PM.

treated with a straight design.Figure provide by WILL CLEARY

A. The side adapted in a furcation invasion.
B.The back adapted in the furcation invasion.Figure provided by WILL CLEARY
CONCLUSION
Effective PM is critical in supporting periodontal health. The greater the number and complexity of periodontal conditions, the more time and skill needed for PM. Identifying the periodontal conditions and local, oral risk factors allows for site-specific instrumentation. Although the biofilm and calculus re-accumulation should be mostly nontenacious and light to moderate in nature, it is challenging to provide quality PM within a reasonable amount of time. Planning a sequence based on patient periodontal conditions is essential to achieving efficacy in ultrasonic debridement during PM.
REFERENCES
- Cohen RE; Research, Science and Therapy Committee. Position paper: periodontal maintenance. J Periodontol. 2003;74:1395–1401.
- Manresa C, Sanz-Miralles EC, Twigg J, Bravo M. Supportive periodontal therapy for maintaining the dentition in adults treated for periodontitis. Cochrane Database Syst Rev. 2018;1:CD009376.
- Gay IC, Tran DT, Weltman R, et al. Role of supportive maintenance therapy on implant survival: a university-based 17 years retrospective analysis. Int J Dent Hyg. 2016;14:267–271.
- Lee CT, Huang HY Sun TC, Karimbux N. Impact of patient compliance on tooth loss during supportive periodontal therapy: a systematic review and meta-analysis. J Dent Res. 2015;94:777–786.
- Ramseier CA, Nydegger M, Walter C, et al. Time between recall visits and residual probing depths predict long term stability in patients enrolled in supportive periodontal therapy. J Clin Periodontol. 2019;46:218–230.
- De Wet LM, Slot DE, Van der Weijden GA. Supportive periodontal treatment: Pocket depth changes and tooth loss. Int J Dent Hyg. 2018;16:210–218.
- Zangrando MS, Damante CA, Sant’ Ana AC, et al. Long-term evaluation of periodontal parameters and implant outcomes in periodontally compromised patients: a systematic review. J Periodontol. 2015;86:201–221.
- Chapple ILC, Mealey BL, Van Dyke TF, et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri‐Implant Diseases and Conditions. J Periodontol. 2018;89:S74–S84.
- American Academy of Periodontology. Comprehensive periodontal therapy: A statement by the American Academy of Periodontology. J Periodontol. 2011;82:943–949.
- Lang N, Adler R, Andreas, Joss Nyman S. Absence of bleeding on probing: An indicator of periodontal stability. J Clin Periodontol. 1990;17: 714–721.
- Lang NP, Joss A, Tonetti M. Monitoring disease during supportive periodontal treatment by bleeding on probing. Periodontol 2000. 1996;12:44–48.
- Checchi L, Montevecchi M, Checchi V, Zappulla F. The relationship between bleeding on probing and subgingival deposits. An endoscopical evaluation. Open Dent J. 2009;28:154–60.
From Dimensions of Dental Hygiene. April 2019;17(4):14,16.

{kind=link}