The Importance of Salivary Flow
The etiology of xerostomia and how to help your patients who suffer from it.
Saliva is a tasteless, colorless, and somewhat viscous solution that is vital to health. This secretion helps with communication, digestion, lubrication, the softening and moistening of food, and the regulation of water balance.1 However, salivary secretion is sometimes reduced as we age. Do our salivary glands just stop working, do they dry up, or are there other reasons that may cause a reduction in our salivary flow?
In humans there are three major pairs of salivary glands (the parotid, submandibular, and sublingual) that differ in the type of secretions they produce.1 The parotid glands produce a serous, watery secretion rich in amylase, the submandibular glands produce more mucinous saliva that is a mixed serous and mucous secretion, and the sublingual gland produces more viscous saliva that is predominantly mucous.1,2 There are also hundreds of minor salivary glands, including the labial, lingual, palatal, buccal, glossopalatine, and retromolar glands.1 The activity of these glands is under the control of the autonomic nervous system, which controls both the volume and the type of saliva secreted.2,3 Saliva serves many important functions. It lubricates and binds, allowing food to move smoothly through the esophagus. Saliva dissolves dry food, which allows for taste to be transmitted. By carrying away food debris, saliva also keeps the oral cavity relatively clean.2 Impairment of salivary gland function has major implications for oral health—increasing susceptibility to caries, tooth demineralization, mucosal ulcerations, and fungal infections.4
XEROSTOMIA
Xerostomia is defined as, “dryness of the mouth caused by abnormal reduction in the amount of salivary secretion,” according to Taber’s Cyclopedic Medical Dictionary. It is subjective, depending on perception of reduced saliva, while salivary hypofunction leads to a lower than normal flow rate.4 Salivary hypofunction can be measured using sialometry, which assesses the flow rates to determine whether an individual has a low salivary flow rate below a given clinical threshold.5 Values for normal and abnormal salivary flow rate demonstrate large variations. Most studies tend to use the criteria of total stimulated salivary flow rate ranges from 1 to 3 mL/min, with low ranges from 0.7 to 1.0 mL/min; salivary hypofunction then is defined as a salivary flow of less than 0.7 mL/min. Unstimulated salivary flow rates range from 0.25 to 0.35 mL/min, with low ranges from 0.1 to 0.25 mL/min, while salivary hypofunction is characterized by an unstimulated flow rate of less than 0.1 mL/min.6 Xerostomia can impair a patient’s quality of life and create severe oral health problems.
Table 1. Common oral clinical signs of xerostomia9
- Saliva: Decreased amounts, may be thick and ropy
- Tongue: Dry, sore, and fissured; yeast infection can cause complications
- Cheeks: Dry, dull in color
- Mastication: Difficulty in eating certain foods; persistent denture problems
- Taste: Alterations in taste
- Swallowing: Trouble with forming and swallowing bolus of food; acid reflux disease
- Teeth: Extensive, rampant dental decay that usually affects the roots of most teeth
There are many known causes for xerostomia and salivary hypofunction, including medication, certain diseases, hyposecretory conditions, dehydration, psychogenic causes, certain activities, trauma, and cancer therapy.7 In the absence of any major illnesses or medications, age does not seem to play a factor in salivary function.8 See Table 1 for a list of common oral clinical signs of xerostomia.9
MEDICATIONS
One of the most prevalent causes of xerostomia is medication.10 More than 1,800 drugs can cause xerostomia. These negative effects can be found in drugs from more than 60 classes and 100 subclasses.11 These include drugs for allergies, anxiety, depression, high blood pressure, pain, Parkinson’s disease, and weight loss.9 Patients who complain of dry mouth should be interviewed and their medications reviewed. In some cases, it may be possible to have the medication or dosage changed.10 The presence of xerostomia is most common in the elderly because they take more drugs than any other sector of the population.9
DISEASES
Several diseases are associated with a decrease in saliva and dry mouth,9 including high blood pressure, diabetes, anemia, cystic fibrosis, HIV infection, rheumatoid arthritis, and Sjögren’s Syndrome.9,12 Sjögren’s Syndrome is an autoimmune disease in which an individual’s own white blood cells attack the moisture-producing glands, causing generalized dryness.13 This disease can be divided into primary and secondary Sjögren’s Syndrome.13 Primary Sjögren’s Syndrome is associated with glandular inflammation (causing dry eyes, mouth, etc). In secondary Sjögren’s Syndrome, salivary hypofunction is associated with a connective tissue disease such as rheumatoid arthritis, systemic lupus, or systemic sclerosis (Scleroderma).13 Sjögren’s Syndrome affects as many as 4 million Americans, and nine out of 10 of these patients are women.12 The average age of onset is usually between 40 and 60 years of age in both sexes.12
 There are still other causes of xerostomia. One such contributor is an excessive loss of body fluids causing dehydration.12 Fever, excessive sweating, vomiting, diarrhea, blood loss, and severe burns can cause dehydration leading to dry mouth.12 However, when fluid balance is restored, such symptoms are usually reversed. A sometimes irreversible xerostomia commonly occurs as a side effect of radiation treatment for certain head and neck cancers9,12 and by chemotherapy for other cancers. Depression, anxiety, stress, or fear are also causes.7,9,12
There are still other causes of xerostomia. One such contributor is an excessive loss of body fluids causing dehydration.12 Fever, excessive sweating, vomiting, diarrhea, blood loss, and severe burns can cause dehydration leading to dry mouth.12 However, when fluid balance is restored, such symptoms are usually reversed. A sometimes irreversible xerostomia commonly occurs as a side effect of radiation treatment for certain head and neck cancers9,12 and by chemotherapy for other cancers. Depression, anxiety, stress, or fear are also causes.7,9,12
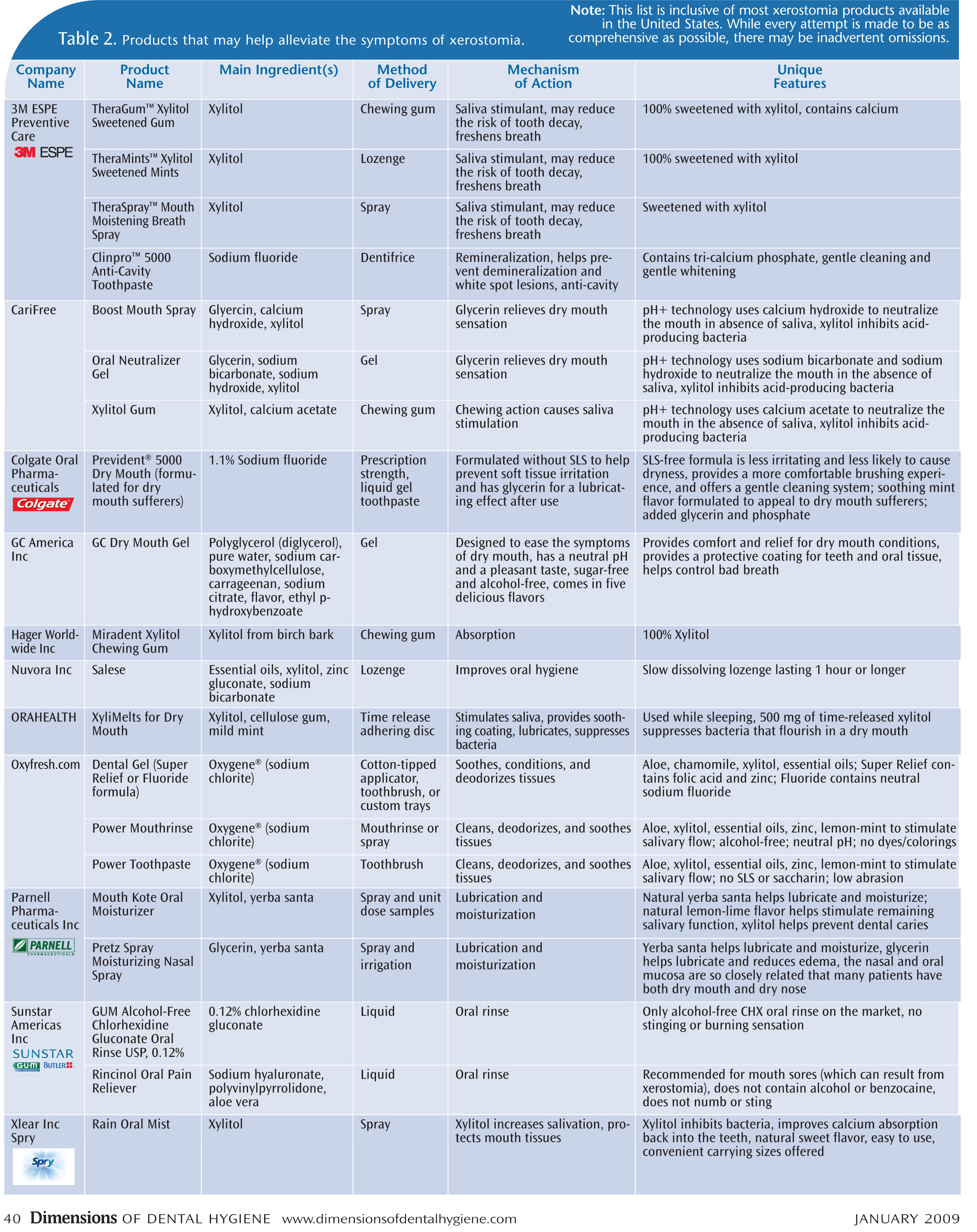
Uncovering the exact cause of xerostomia can prove difficult. However, every effort should be made to identify the source(s) of the problem, since the quality of life can be dramatically affected by xerostomia, and improved by its resolution. While the underlying cause of xerostomia must be determined to address systemic treatment, a variety of products are available that can help treat the symptoms of xerostomia, increasing patient comfort. Table 2 lists some of these products.
REFERENCES
- Ten Cate R. Salivary glands. In: Oral Histology Development, Structure, and Function. St. Louis: Mosby Inc; 1998:315-344.
- Bowen R. Salivary Glands and Saliva. Available at: http://arbl.cvmbs.colostate.edu/hbooks/pathphys/digestion/pregastric/salivary.html. Accessed December 27, 2008.
- Garrett J. The proper role of nerves in salivary secretion: a review. J Dent Res. 1987;66:387-397.
- Hugo FN, Hilgert JB, Corso S, et al. Association of chronic stress, depression symptoms and cortisol with low saliva flow in a sample of south-Brazilians aged 50 years and older. Gerodontology. 2008;25:18-25.
- Thomson W. Issues in the epidemiological investigation of dry mouth. Gerodontology. 2005;22:65-76.
- de Almeida Pdel V, Grégio AM, Machado MA, de Lima AA, Azevedo LR. Saliva composition and functions: a comprehensive review. J Contemp Dent Pract. 2008;9:72-80.
- Johnston N. Oral Health Fact Sheet: Xerostomia. Centre for Rural and Remote Oral Health 2005. Available at: www.crroh.uwa.edu.au/docs/drymouth.pdf. Accessed December 27, 2008.
- Ship JA, Puckett SA. Longitudinal analysis of parotid and submandibular salivary flow rates in healthy, different-aged adults. J Gerontol A Biol Sci Med Sci. 1995;50:M285-M289.
- Sreebny LM, Schwartz SS. A reference guide to drugs and dry mouth—2nd edition. Gerodontology. 1997;14:33-47.
- Bartels C. Xerostomia Information for Dentists. The Oral Cancer Foundation. Available at: www.oralcancerfoundation.org/dental/xerostomia.htm. Accessed December 18, 2008.
- Sreebny L. A useful source for the drug-dry mouth relationship. J Dent Educ. 2004;68:6-7.
- Faculty C. Xerostomia. Aetna Dental Plans, February 12, 2008. Available at: http://www.simplestepsdental.com/SS/ihtSS/r.WSIHW000/st.31937/t.25022/pr.3.html. Accessed December 27, 2008.
- Shiel W. Sjogren’s Syndrome. Available at: www.medicinenet.com/sjogrens_syndrome/article.htm. Accessed December 18, 2008.
From Dimensions of Dental Hygiene. January 2009; 7(1):38-40.

{kind=link}