
Radiography and the Mixed Dentition
The mixed dentition can cause a variety of dental concerns, and radiography— from the traditional to three-dimensional imaging—is integral to effective treatment planning.
The 20 teeth of the primary dentition begin to erupt and start functioning when children are between 2 and 6 years old. Once the first permanent tooth erupts, the oral cavity undergoes significant change over the next 6 years. The mixed dentition period can produce a variety of dental concerns, including malocclusion, crowding and space problems, temporomandibular joint dysfunction, and impaired chewing ability, as well as an increased plaque level and gingivitis due to difficulty in brushing loose or malpositioned teeth. Impacted teeth may also occur during the mixed dentition. After the maxillary third molar, the second most commonly impacted tooth is the maxillary canine.1 The majority (85%) of impacted canines are located on the palatal (or lingual) surface. The remaining 15% are usually found on the buccal surface.2 Since some conditions of the jaws may not be visible clinically, a radiographic examination is necessary for proper treatment planning.
For the primary, mixed, or permanent dentitions, the familiar imaging modalities used include the periapical, bite-wing, occlusal images, and the panoramic views. Exposing intraoral radiographs on patients during the mixed dentition is not always the easiest clinical procedure to achieve with great success. Patient movement, size of the oral cavity, as well as stimulation of the gag reflex may all be road blocks to the production of clear, diagnostic images. In addition, magnification, distortion, and overlap of anatomy commonly occur on conventional radiographs. The development of cone-beam computer tomography and its three-dimensional imaging provide an alternate option in dental imaging.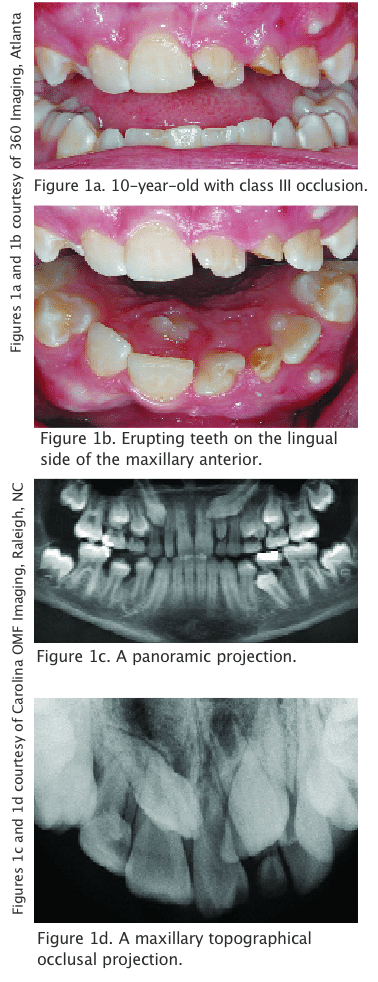
CASE STUDIES
The first case reveals a clinical photograph of a 10-year-old patient with class III occlusion (Figure 1a). More disconcerting than the malocclusion is the position of teeth nine and 10 and the possible dental anomalies associated with their location. Through the use of intraoral photography and a mirror, Figure 1b shows what is erupting on the lingual side of the maxillary anterior teeth, yet many questions about the erupting teeth remain. Is tooth 11 erupting on the buccal side of the maxilla? A panoramic and maxillary topographical occlusal projection were ordered (Figures 1c, 1d). Occlusal radiographs are recommended for localization but have limitations with their field of view.3 These two images do not adequately show what is occurring in the maxillary anterior region in regards to number of teeth present, location, or presence of supernumerary teeth.
Cone-beam imaging or cone-beam computed tomography (CBCT) refers to the use of a cone-shaped x-ray beam to acquire an image. This technology uses a 360° rotation field of view around the patient’s head. The divergent rays capture the region of interest without difficulty. The volume of data acquired during the scanning process is similar to medical computed tomography (CT), but uses much less radiation. Because cone-beam imaging is capable of providing visualization of hard and soft tissues in any plane, computer software allows the oral and maxillofacial radiologist to visualize the region of interest in three dimensions.4
 Three-dimensional imaging is advantageous in evaluating and managing mixed dentition dilemmas, such as impacted canines.5 CBCT images can provide more precise and detailed information than traditional radiographs alone. For example, the position of the teeth and condition of the roots are easily viewed from the facial and lingual aspects. Also, proximity of the impacted tooth to adjacent teeth and possible resorption or anklyosis of roots can also be evaluated.
Three-dimensional imaging is advantageous in evaluating and managing mixed dentition dilemmas, such as impacted canines.5 CBCT images can provide more precise and detailed information than traditional radiographs alone. For example, the position of the teeth and condition of the roots are easily viewed from the facial and lingual aspects. Also, proximity of the impacted tooth to adjacent teeth and possible resorption or anklyosis of roots can also be evaluated.
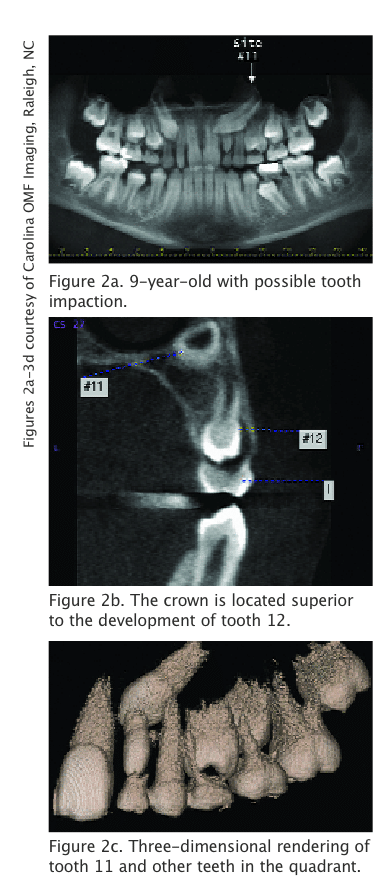
Case two involves a 9-year-old. The panoramic radiograph reveals many primary and permanent teeth present, as well as a possible impaction of tooth 11 (Figure 2a). From this image alone, it is difficult to tell the relationship between the position of tooth 11 to teeth nine, 10, 12, and 13, as well as primary teeth G, H, I and J. Using CBCT, a coronal view of tooth 11 shows that the crown is located superior to the developing root of tooth 12 and approximating the inferior cortical border of the nasal cavity (Figure 2b). The illustrated three-dimensional rendering of the maxillary left posterior teeth shows the exact location of tooth 11 as it relates to the other teeth in the quadrant is the most helpful (Figure 2c).
Case three is a 16-year-old patient who did not develop any third molars, however, a supernumerary tooth exists in the region of teeth 14-15 (Figure 3a). The presence of the extra tooth was a surprise because no clinical signs or symptoms were apparent. A three-dimensional rendering of the left maxilla illustrates what appears to be a normal dentition. However, a surface segmentation from the facial and lingual views clearly demonstrates the presence of the supernumerary tooth and its relationship to teeth 13, 14, and 15 (Figures 3b and 3c). In addition, a sagittal view reveals a dilaceration on the supernumerary tooth (Figure 3d).
In the variety of dental concerns produced by the mixed dentition, impacted teeth are important to consider. One of the biggest hazards that may occur is the resorption of roots of neighboring teeth. In the case of a crowded arch, teeth may be deflected from their normal path of eruption and remain impacted either by bone, teeth, or tissue.2 Radiographic evaluation of the mixed dentition is necessary to assess impacted teeth, and early diagnosis may make a significant difference to the treatment plan for the patient. CBCT may play a vital role in the treatment and assessment of dental patients.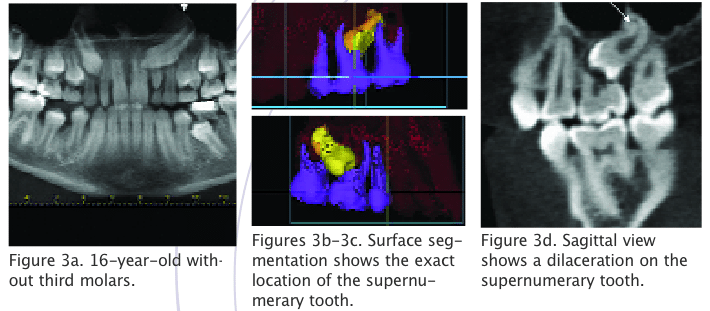
REFERENCES
- Cooke J, Wang HL. Canine impactions: incidence and management. Int J Periodontics Restorative Dent. 2006;26:483-491.
- Roberts-Harry D, Sandy J. Orthodontics. Part 10: Impacted teeth. Br Dent J. 2004;196:319-327.
- Jacobs SG. The impacted maxillary canine. Further observations on aetiology, radiographic localization, prevention/interception of impaction, and when to suspect impaction. Aust Dent J. 1996;41:310-316.
- Haring JI, Howerton LJ. Dental Radiography: Principles and Techniques. 3rd ed. New York: Elsevier Inc; 2006.
- Walker L, Enciso R, Mah J. Three-dimensional localization of maxillary canines with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2005;128:418-423.
From Dimensions of Dental Hygiene. February 2007;5(2): 24-25.

{kind=link}
{kind=link}