Protecting Your Health
The personnel health principles in an infection control program are integral to keeping dental health care workers healthy.
A major goal of infection control is to prevent health care-associated infections among patients and dental health care personnel (DHCP).1,2 The Centers for Disease Control and Prevention (CDC) published updated guidelines and recommendations for infection control in dental health care settings in December of 2003.1 The first section of the guideline discusses elements of a personnel health program. First among the principles of infection control is to stay healthy. 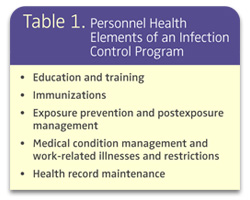
DEVELOPING A PERSONNEL HEALTH PROGRAM
Following are the key elements of a personnel health program recommended by the CDC:1Medical evaluation. Before beginning work, a new dental health care professional should undergo a medical evaluation to ensure that he or she does not pose a risk of infection. This includes a vaccination history.
Health and safety education. The rationale for a personnel health program should be thoroughly explained in order to promote compliance. Clear, concise, written policies and procedures should be in place and communicated to staff. The training should be in accordance with state, federal, and local regulations. All employees should receive training that includes CDC recommendations, Occupational Safety and Health Administration (OSHA) regulations, and practice-specific policies. The training should occur at the time of work assignment and, at least, annually.
Immunization. DHCP immunization records need to be maintained and updated regularly.
Management of work-related illness and post-exposure management. Prompt diagnosis and management of occupationally-related illness, access to appropriate post-exposure management, and polices for work restriction should be promoted.
Counseling. Individually targeted information on risks and prevention of occupationally-acquired infection, risks associated with exposures, exposure management, and potential consequences of exposure should be discussed.
Record keeping. Employee health records must be accessible to OSHA and available in the case of an occupational exposure.
DHCP who take appropriate infection control measures will reduce both risk of personal exposure to infectious pathogens and the risk of transmitting these pathogens to others. Protection against vaccine-preventable diseases is one method to decrease disease transmission.1-3
THE IMPORTANCE OF IMMUNIZATION
DHCP are exposed to a variety of pathogens in dental facilities. The most common are the bloodborne pathogens such as hepatitis B virus (HBV), hepatitis C virus, and HIV.1-3 DHCP are also potentially exposed to airborne and waterborne pathogens. Some of these pathogens may become insignificant relative to transmission if they are vaccine-preventable, such as HBV, varicella, influenza, rubella, and measles. Therefore, keeping track of their vaccination history, titer test results where indicated, and disease history is important. 
In 1997, the Advisory Committee on Immunization Practices (ACIP) of the CDC reviewed immunizations for health care workers. The 2003 guidelines also discuss this issue as a fundamental component of an infection control program.1,2 To be most effective, immunization should be accomplished before there is a risk of exposure. OSHA requires that employers make the HBV vaccination available to any health care worker with potential risk of exposure or to sign a waiver that the offer was declined.4
HBV is a well-recognized occupational risk. It is transmitted by percutaneous or mucosal exposure to blood or body fluids of a person known to be infected with HBV. The risk of infection is related to the hepatitis B e-antigen status of the source individual. The risk is highest for someone both positive for surface and e antigens (HbsAg+ and HbeAg+). CDC estimates an approximate 22% to 31% risk of transmission with a 37% to 62% risk of developing serologic evidence of infection.1 In contrast, if the source individual is HbsAg positive but negative for HbeAg, then the risk is 1% to 6% for transmission and 23% to 37% for developing serologic evidence of infection.1 This applies to DHCP who are not protected by immunization or past infection.1
The most efficient mode of transmission is by percutaneous exposure. While other means of protection against HBV exist, such as engineering controls (devices and technology to isolate or remove a hazard, eg, a safety needle), work practice controls, and personal protective equipment (masks, gloves protective eyewear, protective attire/gowns), the best protection is immunity. Over the past 2 decades, the number of occupationally transmitted infections has dramatically decreased as has the potential for DHCP to transmit HBV to patients or other staff. Prior to 1987, nine clusters of patients were thought to be infected with HBV by DHCP but since then, no reports of such transmission have occurred.1 This is likely the result of HBV vaccination, universal precautions, routine gloving, and OSHA regulations.
TITER TESTING
Prevaccination testing is not indicated but post-vaccination titer testing is recommended to ensure immunity has been conferred. Post-immunization titer testing should be done 1-2 months after the completion of the three dose series. People who do not develop an adequate antibody response should complete a second three dose series or be evaluated to determine if they are HbsAg positive. Post-titer testing should be repeated and if someone remains a nonresponder without detectable antibodies to HBV, he or she should be considered susceptible to infection and follow appropriate measures to avoid exposure and take recommended actions if an exposure does occur to infected blood. If a person is HbsAg positive, then medical follow-up is indicated including advice on preventing transmission to others. At this time, there are no recommendations for boosters.
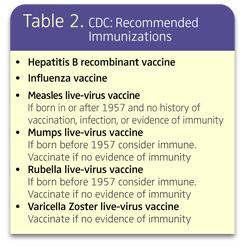
ACIP recommends updating childhood vaccinations and considering others depending on patient population and community levels of disease. Some of these include vaccinations against influenza, measles, rubella, varicella, hepatitis A, pertussis, and tetanus. For some vaccinations, such as measles and rubella, those born before 1957 may be considered immune. Other vaccinations such as hepatitis A are not necessarily indicated for DHCP unless other risks are present and should be provided in accordance to current ACIP recommendations for adults from the CDC.1-3
WORK-RELATED ILLNESS
DHCP need to monitor and maintain their own health. People with acute or chronic medical conditions that may make them susceptible to infections should consult their primary health care provider. The consultation should include a discussion of the possible effects the condition may have on their ability to provide oral health care services and any indicated work restrictions or exclusions.1,3
A written policy should be in place in the exposure control plan, that identifies when restrictions or exclusion from practice/direct patient care are recommended. This information should be reviewed with all staff through education and training. Other aspects of infection prevention and control that should be included in education and training are: handwashing/hand hygiene protocols; respiratory etiquette procedures, eg, covering the mouth and nose with your arm rather than your hand to cough or sneeze, washing hands if you do cough or sneeze into your hand; and other methods to minimize the risk of transmission of pathogens.
All policies and procedures should be in accordance with state, federal, and local regulations and not be punitive to personnel if compliance is expected.1,3 The plan should also designate/assign responsibility for determination of reportable illnesses, restriction of duties, and clearance to return to work.1
Women should not be excluded from direct patient care solely based on pregnancy. However, they should be counseled as to the risk of transmission of specific infections that may have an adverse effect on the developing fetus, such as cytomegalovirus (CMV), hepatitis, herpes simplex, parovirus, and rubella. Education should include information on standard- and transmission-based precautions. Women of child-bearing age should be encouraged to receive immunizations for vaccine-preventable diseases prior to a pregnancy.3
POST-EXPOSURE MANAGEMENT
The primary principle of post-exposure management is to prevent exposure through infection control practices. However, if this is not successful and an exposure occurs, taking immediate action to contain the exposure is essential. In 2001, the CDC updated the post-exposure management guidelines.6 This update is based on epidemiologic surveillance data of exposure incidents among health care personnel and current research findings related to the risks of exposures and effective post-exposure management methods.
Treatment and management of nonbloodborne disease are also integral parts of a personnel health program. The CDC also recommends post-exposure management protocols and training that address exposure to tuberculosis and screening for tuberculosis in facilities where DHCP have contact with infectious patients.1,6 Training and education elements include risk determination, reporting exposures, and anticipated medical follow-up. This training should be provided to all potentially exposed DHCP.6
An infection prevention and control program should include personnel health elements as recommended by CDC. The challenge is to establish a program that is consistent with recommendations and one that personnel can and will follow.
REFERENCES
- Kohn WG, Collins AS , Cleveland JL, Harte JA, Eklund KJ, Malvitz DM, Centers for Disease Control and Prevention (CDC). Guidelines for infection control in dental health-care settings—2003. MMWR Recomm Rep. 2003;19;52(RR-17):1-61.
- Immunization of health-care workers: recommendations of the Advisory Committee on Immunization Practices (ACIP) and the Hospital Infection Control Practices Advisory Committee (HICPAC). MMWR Recomm Rep. 1997;46(RR-18):1-42.
- Bolyard EA, Tablan OC, Williams WW, Pearson ML, Shapiro CN, Deitchman SD. Guideline for infection control in health care personnel, 1998. Hospital Infection Control Practices Advisory Committee. Am J Infect Control. 1998;26:289-354.
- US Department of Labor, Occupational Safety and Health Administration. Occupational exposure to bloodborne pathogens; needlesticks and other sharps injuries; final rule. Fed Regist. 2001;66:5317-5325. .
- United States. Public Health Service. Updated US Public Health Service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2001;50(RR-11):1-52.
- Jensen PA, Lambert LA, Iademarco MF, Ridzon R, Centers for Disease Control and Prevention. Guidelines for preventing the transmission of mycobacterium tuberculosis in health-care settings. MMWR Recomm Rep. 2005;54:1-141.
From Dimensions of Dental Hygiene. September 2006;4(9): 16, 18.

{kind=link}