Improving Your Patients’ Interdental Cleaning Regimen
Strategies for increasing patient compliance.
As dental hygienists are well aware, floss plays a key role in maintaining oral health. Introduced by Dr. Levi Spear Parmly,1 in the early 1800s, flossing has a great expanse of research to document its effectiveness in reducing the risk of interproximal caries and gingivitis.2,3 Dental professionals, particularly dental hygienists who are at the forefront of prevention, have long been educating and encouraging their patients to floss. Despite education and data that illustrate the importance of flossing, surveys show that only 10% to 21% of the American population practices daily flossing.4 At this juncture, dental professionals may need to become more creative in order to increase patient compliance with interdental cleaning.
ALTERNATIVES TO FLOSS
Flossing may not always be the most effective tool for removing interproximal biofilm for all patients. Flossing is most effective when the interdental papillae are intact and the teeth are in contact.5 Flossing becomes progressively less effective in interdental areas that have slight to moderate recession or complete loss of the interdental papillae.5 Patients with poor manual dexterity; physical disabilities, eg, arthritis, hand tremors, limited ability to extend the arms or close the hand, and limited mouth opening; large hands; or a strong gag reflex should be advised on alternative methods for flossing. These conditions may limit a patient’s ability to use floss correctly and could result in trauma and patient frustration. Alternative methods to floss include: interdental brushes, wooden devices, interdental tips, gauze strips, knitting yarn, and pipe cleaners.
MOTIVATING YOUR PATIENTS
 Clearly, interdental cleaning is important to the oral and the general health of patients. However, for pregnant women and patients with specific ailments like heart disease and malodor, the stakes are even higher. Dental hygienists can further their case for interdental cleaning—whether with floss or alternative methods—by explaining the research that is currently available. Patients with heart disease, diabetes, and/or respiratory diseases, should know about the research linking periodontal infections and systemic diseases.6 Patients with oral malodor need to hear about the connection between bad breath and periodontal pockets of 4 mm or greater.7 Pregnant women and caregivers of infants need to be aware of the research that demonstrates a relationship between periodontal infections and low birth weight and the transmitting of bacteria to infants from caregivers.8 This information supports the recommendation of interproximal biofilm removal and may help motivate patients to floss daily.
Clearly, interdental cleaning is important to the oral and the general health of patients. However, for pregnant women and patients with specific ailments like heart disease and malodor, the stakes are even higher. Dental hygienists can further their case for interdental cleaning—whether with floss or alternative methods—by explaining the research that is currently available. Patients with heart disease, diabetes, and/or respiratory diseases, should know about the research linking periodontal infections and systemic diseases.6 Patients with oral malodor need to hear about the connection between bad breath and periodontal pockets of 4 mm or greater.7 Pregnant women and caregivers of infants need to be aware of the research that demonstrates a relationship between periodontal infections and low birth weight and the transmitting of bacteria to infants from caregivers.8 This information supports the recommendation of interproximal biofilm removal and may help motivate patients to floss daily.
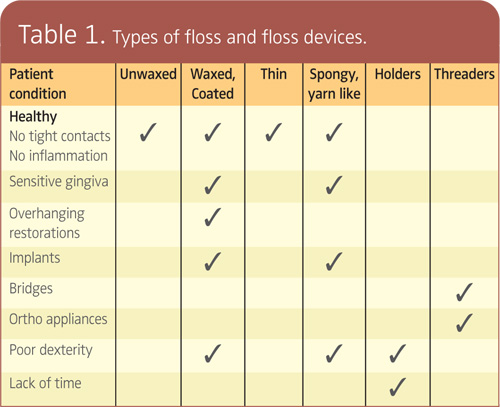
Patient compliance with interdental cleaning is an immense challenge. Manufacturers continue to invent new types of floss and devices to increase patient compliance. Research does not currently show a statistical difference in the plaque removing ability of waxed vs unwaxed floss9 nor between manual flossing and automated flossing devices.10 Therefore, patients’ oral health, dexterity, and preference should be used in determining the most effective flossing tools (see Table 1 for guidelines). 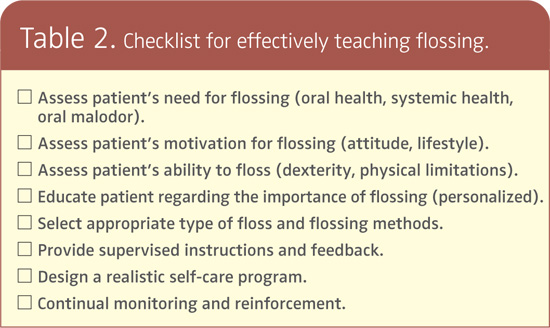
Dental hygienists provide more oral health education services than all other dental professionals.11 Interdental cleaning is one of the main focuses of oral education. A thorough discussion of how to floss or use other interdental cleaning aids is necessary with each patient. After supervised instruction and feedback, a realistic self-care program should be designed. Allowing patients to participate in setting their own goals may increase compliance.12 A recent study found that compliance increased when patients created a written plan that addressed an action and coping components.13 The action component includes: when, where, and how the patient is going to complete interdental cleaning. For example, the patient might write, “Every evening after dinner I will floss my teeth while watching television.” The coping component encompasses two strategies to overcome external barriers to action, such as lack of time, and internal barriers to action, like lack of motivation.
 Motivation often increases when another person monitors compliance.14 For example, most patients clean their teeth more thoroughly than usual before a clinical assessment.15 Dental hygienists need to provide continual assessment and reinforcement of interdental cleaning habits at each patient visit. If possible, providing follow-up phone calls, email messages, or enlisting the support of a patient’s family member to help monitor progress can also improve compliance. Providing feedback devices for home use, such as disclosing agents and saliva test strips, may improve plaque removal and increase motivation.16
Motivation often increases when another person monitors compliance.14 For example, most patients clean their teeth more thoroughly than usual before a clinical assessment.15 Dental hygienists need to provide continual assessment and reinforcement of interdental cleaning habits at each patient visit. If possible, providing follow-up phone calls, email messages, or enlisting the support of a patient’s family member to help monitor progress can also improve compliance. Providing feedback devices for home use, such as disclosing agents and saliva test strips, may improve plaque removal and increase motivation.16
Counseling style can also make a difference. Philip Weinstein, PhD, advocates motivational interviewing as an effective counseling technique. He used it while working with mothers to reduce their children’s rate of tooth decay.17 The approach involves asking the patient questions instead of dictating instructions. The dental professional and the patient devise strategies together to overcome possible objections and beliefs. Follow-up phone calls are also used. It is a time consuming process but also effective, as demonstrated in Weinstein’s study where the children’s caries rate decreased by two thirds.
FACING THE OBSTACLES
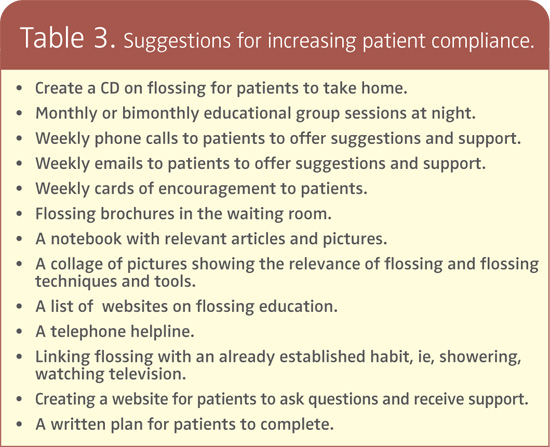
The lack of time allotted in a dental appointment for education decreases the ability of the dental health professional to improve patient compliance.18 Solutions include to dedicate one staff member for a half day or 1 day per week to provide oral health education or to provide monthly group education sessions for patients in the evening. A checklist intervention may also improve the delivery of preventive health services19 (Table 2 provides a checklist that can be used while teaching flossing). Table 3 provides additional ideas for increasing the effectiveness of interdental cleaning education.
Accurately assessing a patient’s flossing needs and providing quality patient education are paramount to best serving patients and improving their oral health. As leaders in prevention, dental hygienists will continue to strive to improve the percentage of patients who perform daily interdental cleaning.
REFERENCES
- . Sanoudos M, Christen AG. Levi Spear Parmly: the apostle of dental hygiene. J Hist Dent. 1999;47:3-6.
- Kinane DF. The role of interdental cleaning in effective plaque control: need for interdental cleaning in primary and secondary prevention. In: Lang NP, Loe H, Armstrong R. Proceedings of the European Workshop on Mechanial Plaque Control. Berlin: Quintessence; 1998:156-168.
- Loe H. Oral hygiene in the prevention of caries and periodontal disease. Int Dent J. 2000:50:129-139.
- Rimondini, L, Zolfanelli B, Bernardi F, Bez C. Self-preventive oral behavior in an Italian university student population. J Clin Periodontol. 2001:28:207-211.
- Consensus report: discussion, section II. Proceedings of the World Workshop on Clinical Periodontics. Chicago: American Academy of Periodontology; 1989:13-17.
- Fowler EB, Breault LG, Cuenin MF. Periodontal disease and its associations with systemic disease. Mil Med. 2001;166:85-89.
- Clark GT, Nachani S, Messagi DV. Detecting and treating oral and nonoral malodors. J Calif Dent Assoc. 1997;25:133-44.
- Asikainen S, Chen C, Alaluusua S, Slots J. Can one acquire periodontal bacteria and periodontitis from a family member? J Am Dent Assoc. 1997;128:1263-1271.
- Ciancio SG, Shibly O, Farber GA. Clinical evaluation of the effect of two types of dental floss on plaque and gingival health. Clin Pre Dent. 1992;14:14-18.
- Shibly O, Ciancio SG, Shostad S, Mather M, Boardman TJ. Clinical evaluation of an automatic flossing device vs manual flossing. J Clin Dent. 2001;12:63-66.
- McConaughy FL, Toevs SE, Lukken KM. Adult clients’ recall of oral health education services received in private practice. J Dent Hyg. 1995;69:202-211.
- Ramsay DS. Patient compliance with oral hygiene regimens: a behavioural self-regulation analysis with implications for technology. Int Dent J. 2000; (Supp) 304-311.
- Schuz B, Sniehotta FF, Wiedemann A, Seemann R. Adherence to a daily flossing regimen in university students: effects of planning when, where, how and what to do in the face of barriers. J Clin Periodontol. 2006;33:612-619.
- Kiyak HA, Persson RE, Persson RG. Influences on the perceptions of and responses to periodontal disease among older adults. Periodontol 2000. 1998;16:34-43.
- Renvert S, Glavlinid L. Individualized instructions and compliance in oral hygiene practices: recommendations and means of delivery. Proceedings of the European Workshop on Mechanical Plaque Control. Chicago: Quintessence;1998.
- Schafer F, Nicholson JA, Gerritsen N, Wright RL, Gillam DG, Hall C. The effect of oral care feed-back devices on plaque removal and attitudes towards oral care. Int Dent J. 2003;53(Suppl):404-408.
- Weinstein P. Promoting prevention. Dimensions of Dental Hygiene. 2004;2(2):24-25, 27-28.
- Basson WJ. Oral health education provided by oral hygienists in private practice. SADJ. 1999;54:53-57.
- Dubey V, Mathew R, Iglar K, Moinnedin R, Glazier R. Improving preventive service delivery at adult complete health check-ups: the Preventive health Evidence-based Recommendation Form (PERFORM) cluster randomized controlled trial. BMC Fam Pract. 2006;7:44.
From Dimensions of Dental Hygiene. September 2006;4(9): 20, 22-23.

{kind=link}