 NALINEE SUPAPORNPASUPAD / ISTOCK / GETTY IMAGES PLUS
NALINEE SUPAPORNPASUPAD / ISTOCK / GETTY IMAGES PLUS
Prioritizing Oral Hygiene to Prevent Hospital-Acquired Pneumonias
Dental hygienists play an important role on multidisciplinary hospital care teams.
This course was published in the May 2023 issue and expires May 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 010
Educational Objectives
After reading this course, the participant should be able to:
- Describe the relationship between oral microorganisms and the development of hospital-acquired pneumonias.
- Recognize barriers related to providing oral hygiene in the hospital setting.
- Describe an evidence-based oral hygiene algorithm for ventilated and nonventilated hospitalized patients.
- Identify the benefits of a having a dental hygienist in the hospital to provide quality and consistent oral hygiene to critically ill patients.
Evidence suggests an inverse correlation exists between the routine completion of high-quality oral hygiene in hospitalized patients and the development of hospital-acquired pneumonias. Despite this correlation, 70% of hospitalized patients do not receive adequate oral hygiene.1
Oral hygiene is often neglected in hospital settings despite its positive effect on patients’ wellness. The oral health of critically ill patients deteriorates rapidly upon hospital admission due to several factors. The oral cavity dries out from the mouth being open for a prolonged period due to intubation or altered mental status. Medications administered during hospitalization may induce xerostomia. Lastly, the performance of oral hygiene may be inadequate because it depends on the healthcare team’s training and engagement as well as the prioritization of dental care. These factors raise the risk of hospital-acquired pneumonias.
Classification
Hospital-acquired pneumonia can be divided into two types:2
- Nonventilator hospital-acquired pneumonia is a lung infection confirmed by imaging, laboratory analysis, and clinical criteria that develops more than 48 hours after hospital admission and was not present at time of admission in nonventilated patients.3
- Ventilator-associated pneumonia (VAP) is a lung infection confirmed by imaging, laboratory analysis, and clinical criteria that develops more than 48 hours after patients have been mechanically ventilated.3
More than 1.7 million people are affected annually with hospital-acquired infections, resulting in heightened healthcare costs, longer duration of hospitalization, and increased mortality.4–6 The American Thoracic Society and the Infectious Diseases Society of America estimate the average cost of each VAP case to be more than $40,000 with hospitalization of 6 to 10 additional days.4,6
Microbiology of Hospital-Acquired Pneumoniasci
The development of hospital-acquired pneumonias is multifactorial, with the oral microbiome playing an important role. More than 600 varieties of microorganisms are present in the oral cavity, which evidence suggests are the contributing factors in the development of hospital-acquired pneumonias. Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, and Enterobacter genus are harmful bacteria that colonize the oral cavity.
Within 48 hours of hospital admission, changes in the oral microbiome can occur, in which virulent pneumonia-causing bacteria begin to proliferate.1 Critically ill patients can micro-aspirate these bacteria into their upper airway, where they migrate to the lungs, leading to pneumonia.5 This micro-aspiration can occur despite the protection of an endotracheal tube or tracheostomy tube with cuff inflated.
The most common nosocomial infection in intensive care units is VAP.4 In the absence of routine oral hygiene, bacterial biofilm in the oral cavity functions as a reservoir for respiratory pathogens. Disrupting the oral cavity’s bacterial biofilm via routine oral hygiene reduces the number of pathogenic oral microorganisms present. Evidence suggests oral hygiene is the most modifiable intervention that can prevent hospital-acquired pneumonias.4,5
Barriers to Providing Oral Hygiene in Hospital Setting
Despite the fact that oral hygiene should be considered an essential component of nursing care, several barriers exist that prevent high-quality, routine completion (Figure 1).
Lack of knowledge. Despite nursing education courses on how to perform oral hygiene, improved oral hygiene in the hospital setting is not occurring. A 2019 survey revealed 84% of healthcare professionals thought they did not have adequate oral hygiene training and would like to receive more education.7 There is a tendency for undereducated bedside critical care staff to brush or swab predominantly just the facial or buccal surfaces when providing oral hygiene.
Lack of time. A demanding workload, insufficient staffing, and high patient acuity are all factors affecting compliance with recommended oral hygiene. Evidence suggests that higher patient-to-nurse proportions resulted in an increased risk of VAP.1 A 2022 survey of hospital outpatient, ward, and operating room nurses found that just 9% were satisfied with the actual implementation of the oral care they provided.8
Low priority for patient care. In some cases, such as when stabilizing a new patient or attending to acute patient decompensation, oral hygiene must be deferred. However, a false perception that oral hygiene should be a lower priority than other tasks also exists. In a 2022 survey of nurses assessing oral hygiene awareness, 69% stated oral care was not a priority.8
Lack of oral hygiene supplies. Some hospitals may lack a formal oral care protocol, and without a protocol, staff are left wondering what supplies to use, when to use them, and how to use them. Warren et al5 discovered that oral hygiene products were lacking at their institution; for example, there were no pre-assembled kits or suction toothbrushes available. Additionally, the most common oral hygiene adjunct in the hospital setting is the foam swab. There is no evidence that a foam swab is effective in disrupting bacterial biofilm.
![]() Oral Hygiene in Hospitalized Patients
Oral Hygiene in Hospitalized Patients
According to the United States Centers for Disease Control and Prevention, the best strategy to prevent hospital-acquired pneumonias is to improve oral hygiene.4,5,9
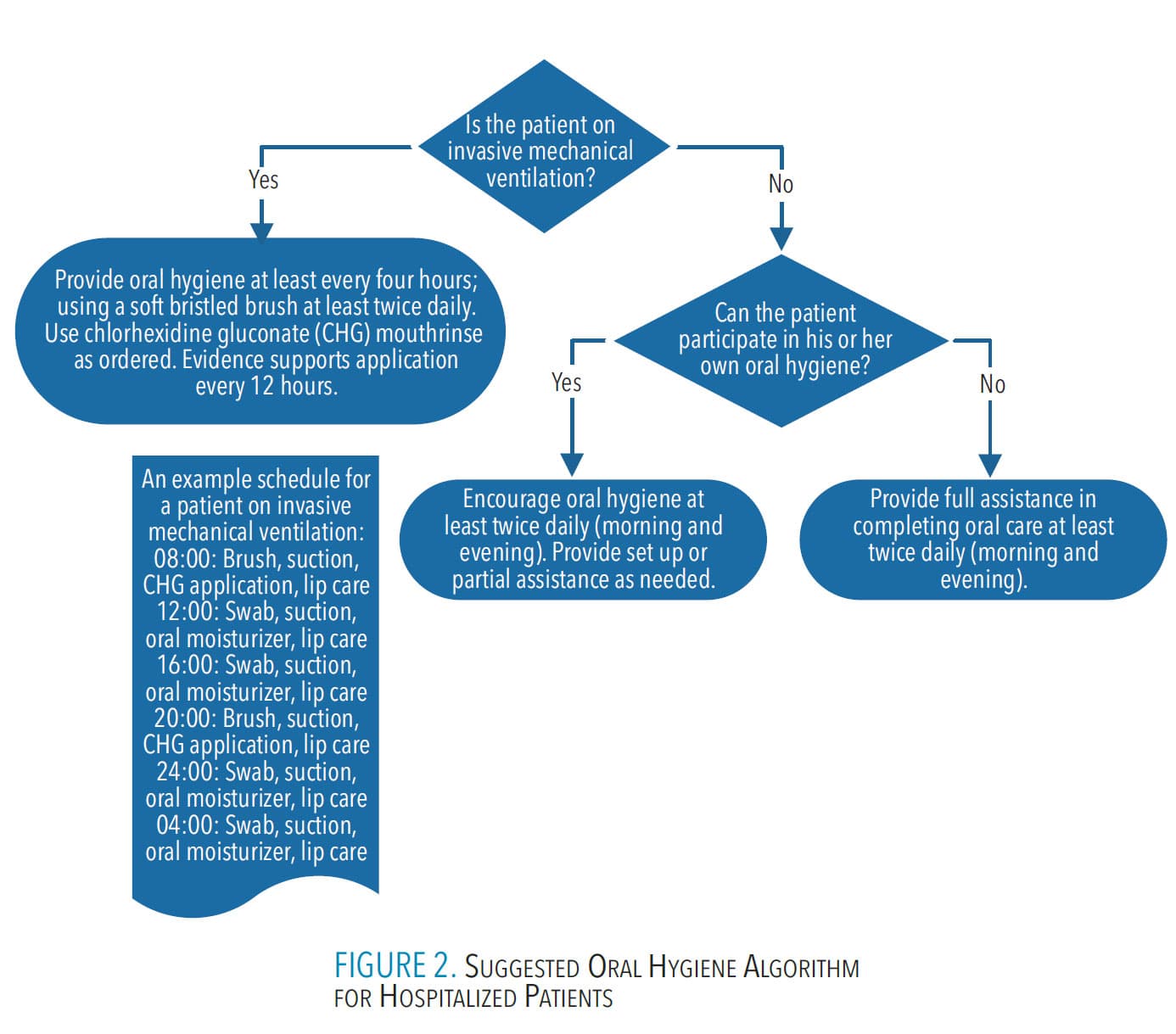
Prior to initiating oral hygiene, an oral health assessment must be completed to identify any oral complications. In addition, the condition of the hospitalized patient needs to be observed so the frequency of oral hygiene and the type of oral hygiene needed can be determined (Figure 2).
 Evidence is limited in identifying the optimal schedule for oral hygiene in hospitalized patients, however following are some generally accepted recommendations:
Evidence is limited in identifying the optimal schedule for oral hygiene in hospitalized patients, however following are some generally accepted recommendations:
- For patients undergoing invasive mechanical ventilation, a systematic review revealed that toothbrushing and chlorhexidine gluconate (CHG) application reduced the incidence of VAP, and oral hygiene—including toothbrushing—is more effective than CHG application alone.10 Toothbrushing was performed twice daily in most studies included in this systematic review, though it was done three times daily in several studies.
To avoid gingival trauma and bleeding in critically ill patients, use a soft-bristled standard toothbrush and have suction available or use a combination suction-toothbrush. If an endotracheal tube is present, it should also be brushed to reduce microbial biofilm. During oral hygiene, provide thorough suctioning of oral secretions to prevent aspiration.
Toothbrushing may need to be deferred in some patients, including those with such profound coagulopathies that toothbrushing may cause clinically relevant blood loss and patients undergoing cancer treatment who have chemo- or radiotherapy-induced oral mucositis.
The application of CHG is recommended. Zhao et al10 reported that the twice-daily application of CHG is the most common schedule, though a few studies used CHG application every 8 hours. Oral hygiene with CHG has been shown to prevent post-operative respiratory tract infections.11
At least every 4 hours and in between toothbrushing, use a swab (with suction catheter available) or a suction-swab soaked in antiseptic solution (cetylpyridinium chloride or other facility-approved oral antiseptic) to clear the gingival tissue, teeth, and oral cavity of debris and secretions. Strong evidence shows that cetylpyridinium chloride is an effective antiseptic against oral flora.12
Less evidence is available to support a specific frequency of use of antiseptic solution. The Association for Professionals in Infection Control and Epidemiology’s 2009 recommendations suggest that antiseptic should be applied alongside the completion of oral care every 2 hours.13 Oral and lip moisturizers should also be applied every 2 hours to 4 hours to reduce inflammation and improve overall oral health.9
Note that patients on mechanical ventilators should not have any removable oral prostheses present.
Reductions of 85% and 56% (medical intervention/control and surgical intervention/control, respectively) in the prevalence of nonventilated hospital-acquired pnuemonia were accomplished by using the following evidence-based guidelines:14
- Perform oral hygiene four times daily while awake, ideally after each meal and once before hour of sleep with a soft-bristled toothbrush or suction-toothbrush. The use of mouthrinse or antiseptic solution is also recommended depending on the patient’s ability to swallow. However, there is insufficient evidence to make recommendations regarding CHG use for patients who are not undergoing invasive mechanical ventilation.9
- Nonventilated patients who can provide their own oral hygiene should be given the necessary oral hygiene supplies and encouraged to complete oral hygiene four times daily while awake, ideally after each meal and once before hour of sleep with a soft-bristled toothbrush and toothpaste. The patient should also be encouraged to use mouthrinse and lip moisturizer to prevent or alleviate dry, sore lips with each oral hygiene episode. Mouth moisturizer may also be appropriate.14
Giuliano et al14 gave oral hygiene recommendations for edentulous patients and denture hygiene. At hour of sleep, the palate, buccal surfaces, gingival tissue, and tongue are brushed with a soft toothbrush or swab. If able, the patient can swish and expectorate antiseptic mouthrinse, or antiseptic solution can be applied to all oral surfaces using a swab/suction-swab. Oral and lip moisturizer should then be applied by the patient or staff. Last, the patient’s dentures should be cleaned using a facility-approved denture cleaning paste, then placed in a denture cup with water and a facility-approved denture cleaning tablet overnight.
Potential Role of the Dental Hygienist in the Hospital Setting
Dental hygienists are becoming part of multidisciplinary hospital care teams.15,16 A small, emerging body of evidence suggests oral hygiene provided by a dental hygienist can reduce the incidence of hospital-acquired pneumonias, healthcare costs, morbidity, and length of hospital stay. A recent systematic review demonstrated that dental hygienists providing oral hygiene reduced the risk of nonventilator associated pneumonia by 35% compared to routine oral hygiene provided by other healthcare professionals.17
Sjogren et al17 revealed that oral hygiene provided by dental professionals reduced mortality from hospital-acquired pneumonia. Oral hygiene provided by nursing personnel, however, did not result in a statistically significant difference in mortality in elderly adults in hospitals or nursing homes.
Dental hygienists embedded into critical care settings will likely address the most common barriers to the provision of oral healthcare in hospital settings due to the following:
- Dental hygienists have detailed knowledge of oral anatomy, physiology, pathophysiology, and strategies for oral hygiene and disease prevention. The oral health knowledge of a dental hygienist far surpasses the education registered nurses or patient care assistants receive.
- Dental hygienists are intentionally focused on oral hygiene.
- Dental hygienists know which supplies to use for each oral hygiene situation, as well as the relative benefits, drawbacks, indications, and contraindications for each. It follows, then, that they are also the best advocate for such supplies if there is a gap in use or availability identified in each institution or setting.
Conclusion
The oral health of hospitalized patients is often neglected despite its positive effect on overall health outcomes. Even though oral hygiene should be considered an essential component of nursing care, barriers prevent high-quality, routine completion of oral hygiene care. The best strategy to prevent hospital-acquired pneumonias is to improve oral hygiene. Dental hygienists are beginning to emerge as necessary additions to multidisciplinary hospital care teams. They are potentially a catalyst for improving oral hygiene across healthcare organizations. Dental hygienists are highly qualified to complete oral health assessments, provide oral hygiene, and educate staff, patients, and family members. While challenges still exist regarding reimbursement of dental hygiene services provided in the hospital and limitations based on state dental hygiene scope of practices, the benefit to patients’ overall health and recovery warrants an innovative jump into the possibilities of hospital-based dental hygienist practice.
References
- Scannapieco FA, Giuliano KK, Baker D. Oral health status and the etiology and prevention of nonventilator hospital-associated pneumonia. Periodontol 2000. 2022;89:51–58.
- National Healthcare Safety Network. Pneumonia (Ventilator-Associated [VAP] and non-ventilator-associated [PNEU]) Event. Available at: cdc.gov/nhsn/pdfs/pscmanual/6pscvapcurrent.pdf. Accessed April 17, 2023.
- Hua F, Worthington HV, Furness S, Zhang Q, Li C. Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia. Cochrane Database Syst Rev. 2016;10:CD008367.
- Ory J, Mourgues C, Raybaud E, et al. Cost assessment of a new oral care program in the intensive care unit to prevent ventilator-assoicated pneumonia. Clin Oral Investig. 2018;22:1945–1951.
- Warren C, Medei MK, Wood B, Schutte D. A nurse driven oral care protocol to reduce hospital acquired pneumonia. Am J Nurs. 2019;119:44–51.
- Talley L, Lamb J, Harl J, Lorenz H, Green L. HAP prevention for nonventilated adults in acute care – can a structured oral care program reduce infection incidence. Nursing Management. 2016;47(12):42–48.
- Davis I, Laybourne T, Cronin C. Improving the provision of mouth care in an acute hospital trust. Nursing Times. 2019;115(5):33–36.
- Koike T, Ohta R, Matsuda Y, Sano C, Kanno T. Oral care awareness and factors related to the burden of nurses at a community hospital in Japan. Healthcare (Basel). 2022;10:1073–1083.
- American Association of Critical Care Nurses. Oral care for acutely and critically ill patients. Crit Care Nurse. 2017;37(3):e19–e2.
- Zhao T, Wu X, Zhang Q, Worthington HV, Hua F. Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia. Cochrane Database Syst Rev. 2020;12:CD008367.
- Klompas M, Branson R, Eichenwald EC, et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35:915–936.
- Langa GPJ, Muniz FWMG, Costa RDSA, da Silveira TM, Rosing CK. The effect of cetylpyridinium chloride mouthrinse as adjunct to toothbrushing compared to placebo on interproximal plaque and gingival inflammation—a systematic review with meta-analyses. Clin Oral Investig. 2021;25:745–757.
- Association for Professionals in Infection Control and Epidemiology. Guide to the Elimination of Ventilator-Associated Pneumonia. Available at: apic.org/resources/topic-specific-infection-prevention/pneumonia. Accessed April 17, 2023.
- Giuliano KK, Penoyer D, Middleton A, Baker D. Oral care as prevention for nonventilator hospital-acquired pneumonia: a four-unit cluster randomized study. Am J Nurs. 2021;121:24–33.
- Barnes CM. Dental hygiene intervention to prevent nosocomial pneumonias. J Evid Base Dent Pract. 2014;I4S:103–114.
- Kelly N, Karim I. Professional dental care may reduce the incidence of non-ventilator-associated pneumonia in hospitals and chronic care settings. J Evid Base Dent Pract. 2021;21:1532–3382.
- Sjogren P, Wardh I, Zimmerman M, Almstahl A, Wikstrom M. Oral care and mortality in older adults with pneumonia in hospitals or nursing homes: systematic review and meta-Analysis. J Am Geriatr Soc. 2016;64:2109–2115.
From Dimensions of Dental Hygiene. May 2023; 21(5):26-29.
