 FAMILYLIFESTYLE / ISTOCK / GETTY IMAGES PLUS
FAMILYLIFESTYLE / ISTOCK / GETTY IMAGES PLUS
Prescription Fluoride for Patients at High Caries Risk
Although it is not the most commonly used form of fluoride, the prescription option plays an important role in providing optimal levels of fluoride.
This course was published in the May 2023 issue and expires May 2026. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 010
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify oral health disparities experienced in the United States.
- Discuss the types of fluoride available.
- Explain the prescription fluoride recommendations for children and adults.
Dental caries is the most common preventable chronic disease and continues to be a significant public health problem.1,2 Fluoride is an important evidence-based therapy known to prevent dental caries.3 Oral health professionals should be knowledgeable on how each form of fluoride, especially prescription fluoride, affects caries prevention.
Oral Health Disparities
Individuals from low-income households, ethnic and racial minorities, and those with certain chronic health conditions are at increased caries risk.4 According to National Health and Nutrition Examination Survey data, caries continues to disproportionately impact low-income families in addition to ethnic and racial minorities.5
Children from low-income households are more than twice as likely to have untreated decay (27%) than children in wealthier households (13%).6 Additionally, the rates of untreated decay among Mexican-American (17.8%) and African-American (20.8%) children between the ages 3 and 5 are three times higher than white children (6.1%).7
These trends persist in adults, with low-income adults twice as likely to experience caries and have unmet oral health needs than their wealthier peers.8 A case-control study showed that adults with diabetes had twice the Decayed, Missing, or Filled Teeth score than controls.9 Furthermore, nearly 88% of adults with intellectual and developmental disabilities had caries experience approximately four times higher than typical adults.10,11
The etiology of caries is multifactorial. Risk factors include excess sugar consumption, poor access to dental care, poor oral hygiene, and inadequate fluoride use.12 Strategies aimed at caries prevention include the following:13–16
- Addressing oral health literacy through education
- Boosting self-efficacy of individuals to encourage healthier decisions
- Targeting social determinants of health that often constrain individual behaviors
- Ensuring access to comprehensive dental services (ie, restorative care when disease is present and preventive care to avoid recurrence)
Most interventions focus on improving access to dental care. Fewer strategies aim to improve oral health literacy, self-efficacy, and the social determinants of health. Efforts are currently underway to evaluate additional strategies.17–19
Forms of Fluoride
Fluoride comes in various forms including professionally applied topical fluoride varnish, fluoride toothpaste, fluoridated water, and prescription fluoride, each with a unique role in preventing caries. Professionally-applied topical fluoride varnish contains the strongest fluoride concentration (9,000 ppm to 22,600 ppm). It is applied to the teeth under the supervision of a healthcare professional during medical and dental visits and school-based oral health programs.20–25
Fluoride toothpaste provides moderate levels of fluoride once or twice a day and all over-the-counter fluoridated toothpastes in the United States contain 1,000 ppm to 1,500 ppm.23,26
Fluoridated water provides low levels of fluoride continuously throughout the day (optimally at 0.7 ppm) and is the most cost-effective way to deliver fluoride.27,28 Bottled water contains differing levels of fluoride depending on the water source. More than 70% of the US population has access to fluoridated water systems.29,30 Prescription fluoride is recommended for high-risk individuals living in areas without fluoridated water.
 Several resources are available to determine the fluoride level of drinking water. The US Centers for Disease Control and Prevention provides information regarding the fluoride level in drinking water for most state public water systems.28 For nonparticipating states, information on fluoride content can be obtained through local utility providers.
Several resources are available to determine the fluoride level of drinking water. The US Centers for Disease Control and Prevention provides information regarding the fluoride level in drinking water for most state public water systems.28 For nonparticipating states, information on fluoride content can be obtained through local utility providers.
For well water, the local public health department should be contacted to have the water tested.29 The US Environmental Protection Agency also emphasizes getting well water tested annually and only using state-certified laboratories.30 Dental professionals should be aware of these resources so they can direct patients to appropriate resources to determine the fluoride level in their drinking water.
Prescription fluoride is available in drops, tablets, and extra-strength toothpaste.21,31 Fluoride drops may easily be mixed into nonfluoridated water and are useful for children or adults who have difficulty chewing tablets.32,33 Tablets are ideal for children older than age 3 who are able to chew them. Extra-strength fluoride toothpaste is easy to incorporate into oral self-care routines and is effective against root caries, xerostomia, and dentin hypersensitivity.34,35
These forms of fluoride—varnish, fluoride toothpaste, fluoridated water, and prescription fluoride supplements—complement each other to provide optimal fluoride exposure and are especially important for high-risk patients.
Prescription Fluoride Recommendations for Children
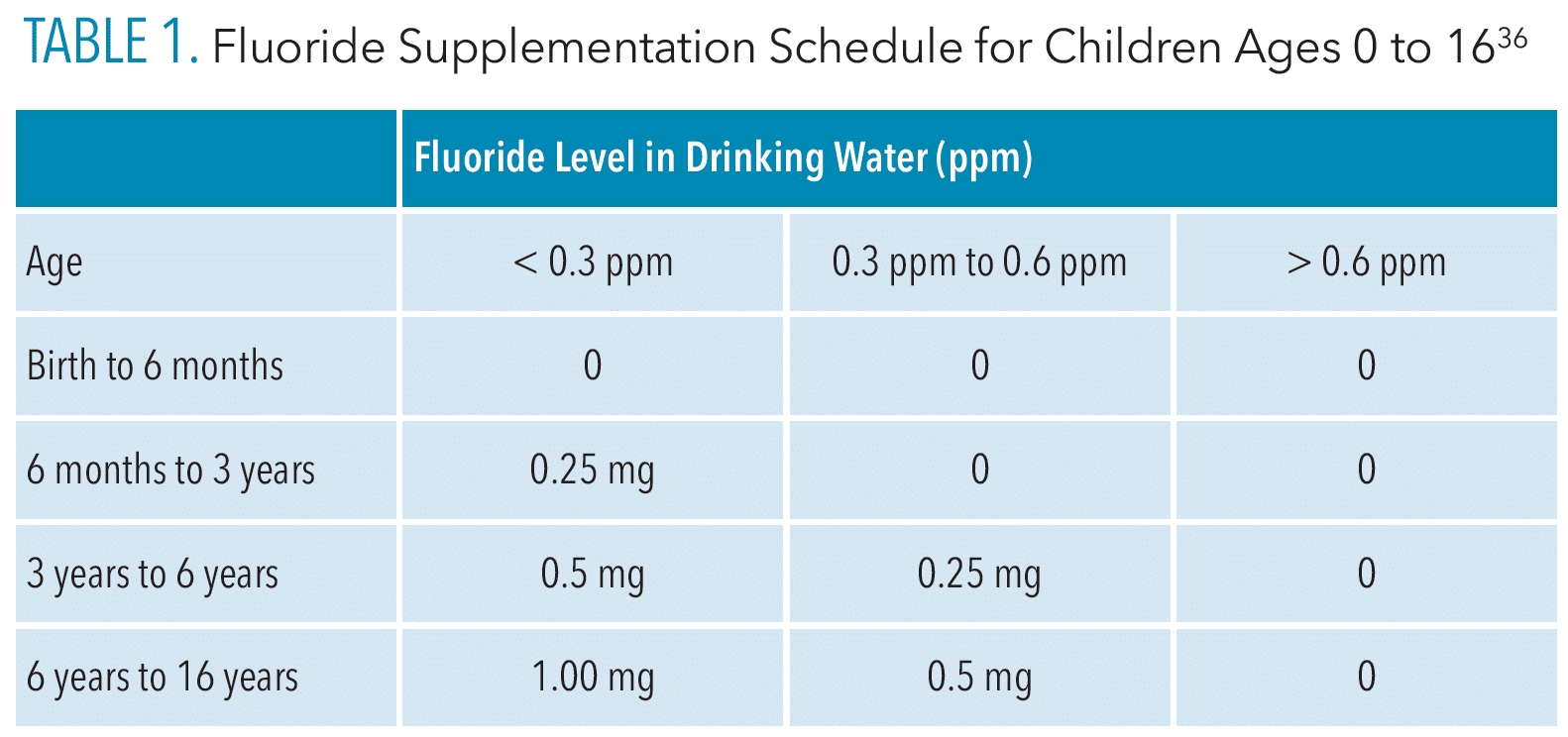
The American Academy of Pediatric Dentistry and the American Dental Association (ADA) recommend fluoride supplementation for children up to age 16 based on age and the fluoridation level of their main drinking water.36,37 Table 1 summarizes the ADA’s recommended fluoride supplement dosages.
Ongoing monitoring can ensure optimal intake of fluoride according to the recommended guidelines.
![]() Prescription Fluoride Recommendations for Adults
Prescription Fluoride Recommendations for Adults
Prescription fluoride recommendations for adults are based on caries risk factors such as low salivary flow or the inability to use certain forms of fluoride (eg, fluoride mouthrinses because of difficulties swishing and expectorating).41 The US Department of Agriculture’s Food and Nutrition Board recommends a total daily fluoride intake of 4 mg for men and 3 mg for women.42
For adults, dental professionals should consider caries risk along with total fluoride intake from sources including water, diet, and other forms to assess whether fluoride supplementation is needed. Prescription toothpaste is most often recommended because of its ease of incorporation into a patient’s oral hygiene routine and its effectiveness in preventing root caries and xerostomia.43,44 The protocol for using prescription toothpaste is as follows:35
- Use a thin ribbon of prescription fluoride toothpaste instead of regular toothpaste at night
- Brush thoroughly for 2 minutes after flossing
- Avoid rinsing, drinking, or eating afterward to allow for maximal fluoride uptake overnight
Comprehensive Healthcare
The dental home is a locus for preventive oral health supervision, anticipatory guidance, specialty referrals, and emergency care. Establishment of a dental home early can lead to more meaningful patient-provider rapport, improved access to regular preventive care, earlier restorative intervention to prevent problems, and specialist referrals when needed. Rapport is an important facilitator for preventive strategies, such as prescription fluoride, whose effectiveness depends on patient compliance.45–48
The medical home is also an important source of prescription fluoride. In a recent study, physicians were three times as likely to prescribe fluoride to high-risk children than dentists.49
Medical and dental integration can provide families with care that promotes optimal oral health. Medical and dental professionals should communicate closely with patients regarding fluoride treatment to ensure they are not exceeding recommended intake. These professionals must also stay up-to-date on fluoride recommendation guidelines and provide consistent information to high-risk individuals.50–54
Fluoride Hesitancy
Previous literature has reported fluoride hesitancy as a growing clinical problem.55 About 13% of caregivers refused topical fluoride treatments during dental or medical visits.56 A recent study reported that caregivers espouse differential decision-making regarding various forms of fluoride for their children, with caregivers preferring fluoride toothpaste over fluoridated water, even when hesitant about topical fluoride.57
These results suggest that high-risk individuals hesitant about some forms of fluoride may be open to prescription fluoride, which could be offered during recare visits and accessed through pharmacies. Oral health professionals need to be informed about each form of fluoride in order to tailor fluoride strategies so they are consistent with the individual’s beliefs and treatment needs.
Beyond Fluoride
Fluoride alone is insufficient in preventing dental caries in high-risk patients.36,58 Preventive therapies, such as dental sealants or silver diamine fluoride, can help prevent dental caries. Perhaps more important is a consistent and comprehensive oral hygiene regimen. As such, behavioral changes and modifications to health decision-making by individuals or caregivers in the home are essential for high-risk patients.
The consumption of sugar sweetened beverages (SSBs) contributes to dental caries risk. Substituting SSBs with sugar-free beverages or water can help lower sugar intake and reduce caries risk. Other strategies include routine self-care motivation, reducing the consumption of fermentable carbohydrates, and tailoring communication strategies to motivate oral hygiene practices. When determining communication strategies, social determinants of health—such as low oral health literacy and limited access to employment opportunities, oral healthcare, oral health resources, healthy foods, and social support—must be considered. 58–61
Conclusion
Various forms of fluoride are available to help prevent dental caries. While prescription fluoride is not utilized as often as other forms, it plays an important role in providing optimal levels of fluoride. Dental professionals should be aware of all of these forms to optimize fluoride exposure in high-risk patients. Other preventive strategies, such as reducing added sugar intake, should be discussed in conjunction with fluoride supplementation to ensure that high-risk patients have the resources needed to prevent dental caries.
References
- Marcenes W, Kassebaum NJ, Bernabé E, et al. Global burden of oral conditions in 1990-2010: a systemic analysisJ J Dent Res. 2013;92:592–597.
- GBD 2017 Oral Disorders Collaborators, Bernabe E, Marcenes W, et al. Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017: a systematic analysis for the Global Burden of Disease 2017 Study. J Dent Res. 2020;99:362–373.
- Weyant RJ, Tracy SL, Anselmo T, et al. Topical fluoride for caries prevention: executive summary of the updated clinical recommendations and supporting systematic review. J Am Dent Assoc. 2013;144:1279–1291.
- Fleming E, Afful J. Prevalence of total and untreated dental caries among youth: United States, 2015–2016. NCHS Data Brief. 2018;307:1–8.
- Duffy EL, Kranz AM, Dick AW, et al. Association between type of health insurance and children’s oral health, NHANES 2011-2014. J Public Health Dent. 2018;78:337–34.
- Griffin SO, Wei L, Gooch BF, et al. Vital signs: dental sealant use and untreated tooth decay among U.S. school-aged children. MMWR Morb Mortal Wkly Rep. 2016;65:1141–1145.
- Rozier RG, White BA, Slade GD. Trends in oral diseases in the U.S. population. J Dent Educ. 2017;81:eS97–eS109.
- Latti BR, Kalburge JV, Birajda SB, Latti RG. Evaluation of relationship between dental caries, diabetes mellitus and oral microbiota in diabetics. J Oral Maxillofac Pathol. 2018;22:282.
- Tiwari T, Franstve-Hawley J. Addressing oral health of low-income populations – a call to action. JAMA Netw Open. 2021;4:e2125263.
- Morgan JP, Minihan PM, Stark PC, et al. The oral health status of 4,732 adults with intellectual and developmental disabilities. J Am Dent Assoc. 2012;143:838–846.
- United States Department of Health and Human Services. Healthy People 2030. Available at: health.g/v/healthypeople/objectives-and-data/browse-objectives/oral-conditions/reduce-proportion-adults-active-or-untreated-tooth-decay-oh-03. Accessed April 17, 2023.
- American Academy of Pediatric Dentistry. Policy on early childhood caries (ECC): Unique challenges and treatment options. The Reference Manual of Pediatric Dentistry. Chicago: American Academy of Pediatric Dentistry; 2021:85–86.
- Northridge ME, Kumar A, Kaur R. Disparities in access to oral health care. Annu Rev Public Health. 2020;41:513–535.
- Assuncao LRDS, Fagundes FAU, Kuklik HH, et al. Different dimensions of oral health literacy are associated with social determinants of health in Brazilian adults. Braz Oral Res. 2022;36:e0122.
- Rezaei S, Yara AHR. Oral health behvarios among schoolchildren in western Iran: determinants and inequality. Clin Cosmet Investig Dent. 2020;12:319–326.
- Horowitz AM, Kleinman DV. Oral health literacy: a pathway to reducing oral health disparities in Maryland. J Public Health Dent. 2012;72:S26–S30.
- Ramos-Gomez F, Kinsler JJ. Addressing social determinants of oral health, structural racism and discrimination and intersectionality among immigrant and non-English speaking Hispanics in the United States. J Public Health Dent. 2022;82(Suppl 1):133–139.
- Tseng W, Pleasants E, Ivey SL, et al. Barriers and facilitators to promoting oral health literacy and patient communication among dental providers in California. Int J Environ Res Public Health. 2021;18:216.
- Chi DL, Hopkins S, O’Brien D, et al. Association between added sugar intake and dental caries in Yup’ik children using a novel hair biomarker. BMC Oral Health. 2015;15:121.
- Spencer AJ, Do LG, Ha DH. Contemporary evidence on the effectiveness of water fluoridation in the prevention of childhood caries. Community Dent Oral Epidemiol. 2018;46:407–415.
- Clark MB, Slayton RL. Fluoride use in caries prevention in the primary care setting. Pediatrics. 2014;134:626–633.
- Mishra P, Fareed N, Battur H, Khanagar S, Bhat MA, Palaniswamy J. Role of fluoride varnish in preventing early childhood caries: a systematic review. Dent Res J. 2017;14:169–176.
- United States Centers for Disease Control and Prevention. Other Fluoride Products. Available at: cdc.gov/fluoridation/basics/fluoride-products.html. Accessed April 17, 2023.
- Rozier RG, Sutton BK, Bawden JW, Haupt K, Slade GD, King RS. Prevention of early childhood caries in North Carolina medical practices: implications for research and practice. J Dent Educ. 2003;67:876–885.
- Bakhurji E, Cooper LH. School-based fluoride varnish programs: a national survey. J Public Health Dent. 2019;79:279–285.
- Thornton-Evans G, Junger ML, Lin M, Wei L, Espinoza L, Beltran-Aguilar E. Use of toothpaste and toothbrushing patterns among children and adolescents—United States, 2013-2016. MMWR Morb Mortal Wkly Rep. 2019;68:87–90.
- Slade GD, Grider WB, Maas WR, Sanders AE. Water fluoridation and dental caries in U.S. children and adolescents. J Dent Res. 2018;97:1122–1128.
- United States Centers for Disease Control and Prevention. My Water’s Fluoride. Available at: nccd.cdc.gov/d_h_mwf/default/default.aspx. Accessed April 17, 2023.
- United States Centers for Disease Control and Prevention. Surgeons Generals Statements on Community Water Fluoridation. 2001. Available at: cdc.gov/fluoridation/guidelines/surgeons-general-statements.html#:~:text=As%20noted%20in%20Oral%20Health,tooth%20decay%20in%20a%20community. Accessed April 17, 2023.
- United States Centers for Disease Control and Prevention. 2018 Fluoridation Statistics. Available at: cdc.gov/fluoridation/statistics/떒s tats.htm. Accessed April 17, 2023.
- Rozier RG, Adair S, Graham F, et al. Evidence-based clinical recommendations on the prescription of dietary fluoride supplements for caries prevention: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2010;141:1480–1489.
- Georgetown University National Maternal and Child Oral Health Resource Center. Fluorides. Available at: mchoralhealth.org/SpecialCare/䁲-prevention/䁲-1.php. Accessed April 17, 2023.
- ESPIRE Dental. Can I give my infant fluoride drops? Available at: espiredental.com/can-i-give-my-infant-fluoride-drops/. Accessed April 17, 2023.
- Drugs.com. Sodium Fluoride Chewable Tablets. Available at: drugs.com/pro/sodium-fluoride-chewable-tablets.html. Accessed Accessed April 17, 2023.
- Dentaquest. Prescription Fluoride Toothpaste. Available at: dentaquest.com/oral-health-resources/oral-health-library/general-oral-health/prescription-fluoride-toothpaste/#:~:text=Prescription%20strength%20fluoride%20toothpaste%20should,two%20minutes%2C%20preferably%20at%20bedtime. Accessed April 17, 2023.
- American Academy of Pediatric Dentistry. Fluoride therapy. The Reference Manual of Pediatric Dentistry. Chicago: American Academy of Pediatric Dentistry; 2021:302–305.
- United States Preventive Services Task Force. Prevention of Dental Caries in Children Younger Than Age 5 Years: Screening and Interventions. Available at: uspreventiveservicestaskforce.org/uspstf/draft-update-summary/prevention-of-dental-caries-in- children-younger-than-age-5-years-screening-and-interventions1. Accessed April 17, 2023.
- Warren JJ, Levy SM, Broffitt B, et al. Considerations on optimal fluoride intake using dental fluorosis and dental caries outcomes—a longitudinal study. J Public Health Dent. 2009;69:111–115.
- United States Centers for Disease Control and Prevention. Private Wells. Available at: cdc.gov/fluoridation/faqs/wellwater.htm. Accessed April 17, 2023.
- United States Environmental Protection Agency. Private Drinking Water Wells. Available at: epa.gov/privatewells. Accessed April 17, 2023.
- United States Centers for Disease Control and Prevention. Recommendations for Using fluoride to Prevent and Control Dental Caries in the United States. Available at: cdc.gov/mmwr/pdf/rr/rr5014.pdf. Accessed April 17, 2023.
- National Institutes of Health. Office of Dietary Supplements: Fluoride. Available at: ods.od.nih.gov/factsheets/Fluoride-HealthProfessional. Accessed April 17, 2023.
- Glick A, Sista V, Johnson C. Oral manifestations of commonly prescribed drugs. Am Fam Physician. 2020;102:613–621.
- Tellez M, Wolff MS. The public health reach of high fluoride vehicles: examples of innovative approaches. Caries Res. 2016;50(Suppl 1):61–67.
- Nowak AJ, Casamassimo PS. The dental home: a primary care oral health concept. J Am Dent Assoc. 2002;133:93–98.
- Babu KLG, Doddamani GM. Dental home: patient centered dentistry. J Int Soc Prev Community Dent. 2012;2:8–12.
- Nowak AJ, Casamassimo PS. The dental home. In: Early Childhood Oral Health. 2nd ed. Hoboken, New Jersey: Wiley-Blackwell; 2015:134–152.
- Chen HF, Tsai YF, Lin YP, et al. The relationships among medicine symptom distress, self-efficacy, patient-provider relationship, and medication compliance in patients with epilepsy. Epilepsy Behav. 2010;19:43–49.
- Ko A, Banks JT, Hill CM, Chi DL. Fluoride prescribing behaviors for Medicaid-enrolled children in Oregon. Am J Prev Med. 2022;62:e69–e76.
- Cruz S, Kerr D, Nguyen DP, Carlyle A, Chi DL. Qualitative evaluation of the pre-implmentation phase of a rural dental clinic co-located within a health center in the Pacific Northwest of the United States. Community Dent Oral Epidemiol. 2023;51:256–264.
- Reynolds JC, Damiano PC, Herndon JB. Patient centered dental home: building a framework for dental quality measurement and improvement. J Public Health Dent. 2021;82:445–452.
- Sengupta N, Nanavati S, Cericola M, Simon L. Oral health integration into a pediatric practice and coordination of referrals to a colocated dental home at a federally qualified health center. Am J Pub Health. 2017;107:1627–1629.
- Silk H, Mccallum W. Fluoride: the family physician’s role. Am Fam Physician. 2015;92:174–179.
- Chi DL. Parent refusal of topical fluoride for their children: clinical strategies and future research priorities to improve evidence-based pediatric dental practice. Dent Clin North Am. 2017;61:607–617.
- Chi DL, Basson A. Surveying dentists’ perceptions of caregiver refusal of topical fluoride. JDR Clin Trans Res. 2018;3:314–320.
- Chi DL. Caregivers who refuse preventive care for their children: the relationship between immunization and topical fluoride refusal. Am J Pub Health. 2014;104:1327–1333.
- Ko A, Chi DL. Fluoride hesitancy: a mixed methods study on decision-making about forms of fluoride. Community Dent Oral Epidemiol. October 11, 2022. Online ahead of print.
- Chi DL, Scott JM. Added sugar and dental caries in children: a scientific update and future steps. Dent Clin North Am. 2019;63:17‐33.
- Bernabe E, Vehkalahti MM, Sheiham A, et al. Sugar-sweetened beverages and dental caries in adults: a 4-year prospective study. J Dent. 2014;42:952–958.
- Mutluay M, Mutluay AT. The importance of oral health care strategies and home care motivation. JMDCR. 2017;4:10–13.
- Elwell K, Camplain C, Kirby C, et al. A formative assessment of social determinants of health related to early childhood caries in two American Indian communities. Int J Environ Res Public Health. 2021;18:9838.
From Dimensions of Dental Hygiene. May 2023; 21(5):40-43.
