
Power of Omega-3s
These essential fatty acids provide both systemic and oral health benefits.
This course was published in the November 2012 issue and expires November 2015. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define omega–3 polyunsaturated fatty acids.
- Discuss the health benefits of omega–3 polyunsaturated fatty acids.
- Identify how to choose a good omega–3 food source or supplement.
Omega–3 polyunsaturated fatty acids are the most commonly used nonvitamin, nonmineral nutritional supplement in the United States.1 The benefits of omega–3s are well known, particularly for their support of cardiovascular health. The American Heart Association (AHA) recommends consuming adequate amounts of omega–3s through food or supplementation,2 and the federal Food and Drug Administration (FDA) has sanctioned the promotion of omega–3s as helpful in reducing the risk of heart disease.3 Understanding the role that fats play in overall health, the different types of omega–3s available, and how to choose the best source of omega–3s is key to harnessing the health benefits of these fatty acids.
THE SKINNY ON FATS
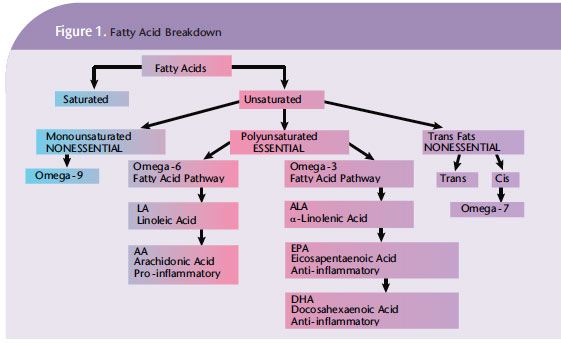
The consumption of fats or lipids is necessary for overall health. Fats are used as a primary energy source in cells, providing 9 calories of energy per gram. Chemically, fats are neutral organic compounds made of three fatty acid carbon chains attached to a glycerol molecule. Fatty acid chains vary in length based on the number of carbon atoms and the number of double bonds. A carbon atom can bond to four other atoms. A fatty acid chain that contains zero double bonds is saturated, a chain with one double bond is monosaturated, and a chain with two or more double bonds is polyunsaturated. The length of the fatty acid chain and degree of saturation give each lipid its unique properties. Edible fats from plants or animals are further categorized (Figure 1) as saturated, unsaturated, monosaturated, polyunsaturated, trans fats, natural trans fats, essential fats, and nonessential fats. The consumption of saturated fats contributes to atherosclerosis, raises cholesterol levels, and can lead to obesity. Sources include animal fats; dairy; coconut oil; palm kernel oil; chocolate; and some processed, prepared, and fast foods.
Monosaturated fats, also referred to as omega–9s, can improve blood cholesterol levels. They are found in cashews, olives, avocados, and canola oil. In lesser amounts, they are also found in macadamia nuts, sesame and sunflower seeds, peanuts, corn oil, wheat, and oatmeal.
Trans fats are commercially created by partially hydrogenating vegetable oils. It is thought that the body has difficulty digesting trans fats because lipase, the enzyme that breaks down fat, does not recognize them. Thus, excess trans fats end up circulating in the blood. They can increase the risk of cardiovascular disease, elevate low–density lipoprotein cholesterol, and lower the levels of high–density lipoprotein cholesterol or healthy fat.4 A study by Hu et al found that a 2% increase in trans fats consumption doubled the risk of coronary heart disease among women.5 The amount of trans fats contained in foods must be listed on the package. In the US, however, if the food contains less than 0.5 grams of trans fats, the label can state that the food is free of trans fats.6 To completely avoid trans fats, determine whether partially hydrogenated vegetable oil or shortening appear on the label. If either is present, the product contains trans fats.
BALANCING ACT
Omega–6 and omega–3 are the two main polyunsaturated fatty acids (PUFAs). They are called essential fatty acids because they are necessary parts of the human diet that must be consumed because the body cannot create them. These essential fats are needed for optimal function of cell membranes and are not used for energy.
Linoleic acid (LA) is the main form of omega–6 PUFA, and it chemically breaks down into arachidonic acid (AA). Foods containing omega–6s include safflower, corn, and soybean oil.
There are three main types of omega–3 PUFAs: alpha–linolenic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). ALA is found in flaxseed; English walnuts; green leafy vegetables; nuts; beans; and vegetable, walnut, and linseed oil. The amount of ALA in these foods varies. For example, a tablespoon of English walnuts has 0.7 g of ALA per tablespoon whereas flaxseed oil contains 8.5 g per tablespoon. The body will break down only 0.2% to 4% of the ALA in foods, and convert it into the two other important forms of omega–3 EPA and DHA.7
The main source of EPA and DHA, outside of being broken down from ALA, is fatty fish such as salmon, mackerel, herring, and tuna. Only fish caught in the wild offer high levels of omega–3s. Farm–raised, grain–fed fish contain reduced levels. Frying fish adds trans fats and, thus, should be avoided. Omega–3s, in the form of EPA and DHA, serve as reservoirs for eicosanoids—antiinflammatory compounds and mediators including resolvin, protectin, and prostaglandins. They fight against inflammation.
On the other hand, omega–6s, in the form of AA, serve as reservoirs for compounds and mediators that promote the body’s inflammatory responses.8 Decades ago, diets were in balance between the ingestion of omega–3 and omega–6. The ratio was 1:1. In the typical American diet today, the ratio is 1:10 and as much as 1:30.9 This means there is more AA in the body promoting inflammation than there is eicosanoids reducing inflammation.
This imbalance is due, in part, to the increased use of vegetable oils high in linolenic acid, such as corn, soy, and safflower oils. Meats and eggs from animals that are grain fed instead of grazing on grass are also high in omega–6. Consuming high levels of omega–6 leads to AA production, the precursor to pro–inflammatory mediators. Without adequate amounts of omega–3 in the diet, the inflammatory effects of omega–6 cannot be countered.
EFFECTS OF OMEGA–3
An AHA review of randomized controlled trials demonstrates the health benefits of omega–3 fatty acids. The review found that men who consumed fish weekly were less likely to die from coronary heart disease than those who did not.2 Other cardiovascular risk factors, such as obesity and hypertension, were also diminished in the fish–eating group.2–4,7–9 As the amount of omega–3 in the blood increased, the risk of sudden death in men without a history of cardiovascular disease decreased. In a study conducted on women, Hu et al found that those who consumed wild, fatty fish also had a reduced risk of death due to coronary heart disease.10
 There are other health benefits to a diet rich in omega–3 fatty acids. Physicians have long prescribed the prescription–strength omega–3 (Lovaza®) to patients with triglyceride levels higher than 500 mg/dL.11 Studies have shownthat EPA and DHA also lower serum triglycerides.12 Eating fish during pregnancy may be controversial because of possible mercury exposure, yet omega–3s support fetal brain development.13 A study by Tan et al found a 40% reduction in the risk of age–related macular degeneration in individuals who consumed fish high in omega–3s on a weekly basis.14
There are other health benefits to a diet rich in omega–3 fatty acids. Physicians have long prescribed the prescription–strength omega–3 (Lovaza®) to patients with triglyceride levels higher than 500 mg/dL.11 Studies have shownthat EPA and DHA also lower serum triglycerides.12 Eating fish during pregnancy may be controversial because of possible mercury exposure, yet omega–3s support fetal brain development.13 A study by Tan et al found a 40% reduction in the risk of age–related macular degeneration in individuals who consumed fish high in omega–3s on a weekly basis.14
Omega–3s may also benefit people with rheumatoid arthritis (RA), an autoimmune disease where the synovial joints are chronically inflamed. Patients with RA who supplemented with omega–3s not only experienced a reduction in pain and inflammation, but their use of nonsteroidal anti–inflammatory medication also decreased.15
Omega–3 consumption is beneficial for those with osteoarthritis, a musculoskeletal disorder that causes the breakdown or loss of cartilage in the joints. A study by James found that nutritional intervention with omega–3 led to a decrease in pain and an increase in joint function among patients with osteoarthritis.16
OMEGA–3 AND ORAL HEALTH
Periodontal health is related to omega–3 consumption. The National Health and Nutrition Examination Survey examined more 9,000 adults, of which 1,024 were diagnosed with periodontitis. The study found that the prevalence of periodontitis was higher among those with a lower dietary intake of omega–3 DHA and, to a lesser extent, EPA.17 Another study found that omega–3 consumption also decreased osteoclast activity, which leads to bone loss.18
The bacteria and biofilm that initiate periodontal disease cause the body to produce a variety of pro–inflammatory mediators, including interleukin–1, tumor necrosis factor–alpha, reactive oxygen species, and C–reactive protein, as well as lipid mediators. These mediators contribute to the collagen destruction and bone resorption associated with periodontal diseases. Lipid mediators derived from omega–3 EPA and DHA—resolvin and protectin—stimulate anti–inflammatory pathways and fight inflammation in various ways, including: promoting tissue regeneration,19 increasing antioxidant capacity,20 producing anti–inflammatory mediators that decrease the creation of pro–inflammatory cytokines,21 and reducing osteoclastic activity.22 Consuming EPA and DHA may help resolve the inflammation associated with resolvin and protectin function.19 Research suggests that a dietary intervention with omega–3s and antioxidants could target the patient’s inflammatory response, therefore, enhancing the biological or molecular pathways that resolve inflammation, rather than just treating the symptoms of the disease.23
REAPING THE BENEFITS
Canada, Sweden, the United Kingdom, Australia, Japan, and the World Health Organization provide dietary recommendations for omega–3 fatty acids: 0.3 g to 0.5 g per day of EPA and DHA, and 0.8 g to 1.1 g per day of ALA.2 The US Institute of Medicine’s recommendations for ALA are set higher at 2.7 g per day. The AHA advises individuals to eat fatty fish twice a week and use vegetable oils containing ALA to meet these guidelines.2 For those with coronary heart disease, the AHA recommends increasing the EPA and DHA level to 1 g per day. Patients with high triglycerides or high blood pressure should take 2 g to 4 g of EPA and DHA.2 At this point, supplementation may be indicated because it could be difficult to sustain this level of fish consumption consistently.
Because fish can contain mercury, dioxins, and polychlorinated biphenyls, there is concern about the health risks of consuming fatty fish and taking omega–3 supplements. Salmon and canned light tuna are labeled as low–mercury seafoods by the FDA. At this time, the FDA asserts that consuming fish does not pose any health risks, except among pregnant women and young children who should limit their consumption to no more than two meals per week.24 There are government standards for the maximum allowable levels of mercury, dioxins, and polychlorinated biphenyls in omega–3 supplements, although they are not always heeded.25 In the more highly refined and concentrated omega–3 fatty acid supplements, there is virtually no mercury and very low levels of the other contaminants.
When purchasing an omega–3 supplement, it is critical to read the label carefully to understand precisely what is contained in each dose. Omega–3 supplements differ in: the number of tablets needed to achieve one serving; the size of each individual capsule; and the amount of EPA, DHA, and other omega–3s, as well as the amount of fish oil contained in the supplement. For example, the prescription omega–3 Lovaza states that a single dose is one 1,000 mg tablet that contains 465 mg of EPA, 375 mg of DHA, and 60 mg of other omega–3s (most likely ALA), for a total of 900 mg. Since the dose is one 1,000 mg capsule, this supplement offers a 90% concentration all of omega–3s. In comparison, an over–the–counter (OTC) supplement states that one capsule is one serving and contains 1,000 mg of fish oil concentrate, 180 mg of EPA, and 120 mg of DHA. The concentration of this capsule is calculated by adding the 180 mg of EPA to the 120 mg of DHA for a total of 300 mg of omega–3. Since the dose is one 1,000 mg capsule, this is only a 30% concentration. Taking more capsules of a lower concentration is not advised as this may lead to ingesting substances the body does not need, which could negate the efficacy of the contained omega–3s.
Knowing what is contained in the rest of the supplement is also very important. Supplements may include fish oil; cholesterol; saturated fats; omega–6; canola oil; glycerin; tocopherols; astaxanthin; and, if not highly purified, mercury, polychlorinated biphenyls, and dioxins. With the exception of tocopherols and astaxanthin, the remaining ingredients do not contribute positively to overall health, and some may have negative effects. Patients are aware of the health benefits of omega–3 and may be taking a supplement. When reviewing patients’ medical histories, dental professionals should review, not only prescription and OTC medications, but nutritional supplements, as well. It should be noted if a patient is taking a prescription omega–3 formulation or an OTC brand. Patients should be advised to take the purest concentration of omega–3 available.
CONCLUSION
As the evidence continues to grow regarding the role of nutrition and nutritional supplementation in oral and systemic health, dental professionals will need to integrate these concepts into treatment protocols. Nutritional counseling can include a discussion on the importance of omega–3s and their effects on both oral and systemic health. Dental hygienists spend the most time with patients and are well poised to offer nutritional guidance. By providing current and accurate information, dental hygienists can guide patients in making wise choices concerning omega–3 supplementation, in consultation with their physicians, so they can reap the maximum benefits of this essential nutrient.
PROF. KENNETH SEDDON & DR. TIMOTHY EVANS, QUEEN’S UNIV BELFAST/PHOTO RESEARCHERS INC
REFERENCES
- Omega–3 Supplements: An Introduction. Available at: nccam.nih.gov/health/ omega3/introduction.htm. Accessed October 12, 2012.
- Kris–Etherton PM, Harris WS, Appel LJ. Fish consumption, fish oil, omega–3 fatty acids and cardiovascular disease. Circulation. 2002; 106: 2747–2757.
- FDA Announces Qualified Health Claims for Omega–3 Fatty Acids. Available at: www.fda.gov/siteindex/ucm108351.htm.Accessed October 12, 2012.
- Marchand V. Trans fats: What physicians should know. Paediatr Child Health. 2010; 15:373–378.
- Hu FB, Stampfer MJ, Mason JE, et al. Dietary fat intake and risk of coronary heart disease in women. N Engl J Med. 1997;337:1491–1499.
- Nutrition Labeling; Questions L1 through L153. Available at: www.fda.gov/ Food/ GuidanceComplianceRegulatoryInformation/ GuidanceDocuments/ FoodLabeling Nutrition/ FoodLabelingGuide/ ucm064904.htm#transfat. Accessed October 12, 2012.
- Pawlosky RJ, Hibbeln JR, Novotny JA, Salem N Jr. Physiological compartmental analysis of alphalinolenic acid metabolism in adult humans.J Lipid Res. 2001;42:1257–1265.
- Serhan CN, Hong S, Gronert K, Colgan SP, Devchand PR, Mirick G, Loussignac RL. Resolvins: a family of bioactive products of omega–3 fatty acid transformation circuits initiated by aspirin treatment that counter proinflammation signals. J Exp Med. 2002;196:1025–1037.
- Hu FB, Bronner L, Willett WC, et al. Fish and omega–3 fatty acid intake and risk of coronary heart disease in women. JAMA. 2002; 287:1815–1821.
- Simopoulos AP. Essential fatty acids in health and chronic disease. Am J Clin Nutr. 1991: 70(Suppl):560S 569S.
- Rupp H. Omacor (prescription omega–3–acid ethyl esters 90): From severe rhythm disorders to hypertriglyceridemia. Adv Ther. 2009;26:675–690.
- Grimsgaard S, Bonaa KH, Hansen JB, Nordoy A. Highly purified eicosapentaenoic acid and docosahexaenoic acid in humans have similar triacylglycerol–lowering effects but divergenteffects on serum fatty acids. Am J Clin Nutr.1997;66:649–659.
- Swanson D, Block R, Mousa SA. Omega–3 fatty acids EPA and DHA: health benefits throughout life. Adv Nutr. 2012;3:1–7
- Tan JS, Wang JJ, Flood V, Mitchell P. Dietary fatty acids and the 10–year incidence of age-related macular degeneration: the Blue Mountains Eye Study. Arc Ophthalmol. 2009; 5:657–665.
- Goldberg RJ, Katz J. A meta–analysis of the analgesic effects of omega–3 polyunsaturated fatty acid supplementation for inflammatory joint pain. Pain. 2007;129:210–223.
- James MJ. Dietary omega–3 fats for treatment of inflammatory joint diseases: efficacy and utility. Rheum Dis Clin N Am. 2008;34:469–479.
- Asghar Z, Naqvi AZ, Buettner C, Phillips RS, Davis RB, Mukamal KJ. N–3 fatty acids and periodontitis in US adults. J Amer Diet Assoc.2010;110:1669–1675.
- Kesavalu l, Vasudevan b, Raghu B, et al. Omega–3 fatty acid effect on alveolar bone loss in rats. J Dent Res. 2006;85:648–652.
- Van Dyke TE. The management of inflammation in periodontal diseases.J Periodontal. 2008;79:1601–1608.
- Chapple ILC. Potential mechanisms underpinning the nutritional modulation of periodontal inflammation. J Am Dent Assoc.2009;140:178–184.
- Enwonwu CO, Ritchie CS. Nutrition and inflammatory markers. J Am Dent Assoc.2007;138:70–73.
- Campan P, Planchand PO, Duran D. Piot study of n–3 polyunsaturated fatty acids in the treatment of human experimental gingivitis.J Clin Periodontol. 1997;224:901–913
- Van Dyke TE. Proresolving lipid mediators: potential for prevention and treatment of periodontitis. J Clin Periodontal. 2011; 388(Suppl):119–125.
- Food and Drug Administration. 2004 EPA and FDA Advice For: Women Who Might Become Pregnant, Women Who are Pregnant, Nursing Mothers, and Young Children. Available at: www.fda.gov/Food/FoodSafety/Product-SpecificInformation/ Seafood/ Foodborne PathogensContaminants/ Methyl mercury/ ucm115662.htm. Accessed October 12, 2012.
- Beamish R. Wading into fish oil supplement safety. San Francisco Chronicle: Datebook. Available at: www.sfgate.com/ health/ article/Wading-into-fish-oil-supplement-safety-3195238.php#page-1. Accessed October 12,2012.
From Dimensions of Dental Hygiene. November 2012; 10(11): 60–63.
