Minimize Medication Risks in Pregnant Patients
Dental hygienists can help pregnant women limit those factors that may cause harm to the normal morphology of the developing fetus.
This course was published in the December 2014 issue and expires December 31, 2017. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define teratogens.
- Discuss the United States Food and Drug Administration drug categories for medication use in pregnant women.
- Explain the role of dental hygienists in treating pregnant patients.
Pregnancy is a time of specialized cellular movement, initiation of new tissue formation, differentiation of cell purpose, and maturation of cell groups into working vital organs and systems. Providing effective care to ensure the health and well-being of pregnant women means protecting these cellular changes.1 Understanding medication and drug use during pregnancy can be complicated due to a lack of scientific research on the subject.2 Currently, less than 10% of medications approved by the United States Food and Drug Administration (FDA) include teratogenicity or risk for birth defects on their labels.2 Teratogenicity is the capability of a chemical or infectious agent, deficiency, or environmental toxin to cause congenital malformation or birth defects. Many women of childbearing age are unaware of drug contraindications that may cause harm to the embryo during pregnancy.1,3,4 The Centers for Disease Control and Prevention’s (CDC) most recent data demonstrate that approximately one in every 33 babies (about 3%) are born with a birth defect.5 One of the leading causes of infant deaths, birth defects account for more than 20% of all infant mortality.5 In order to provide the best possible care to pregnant women, dental hygienists need to understand pregnancy and prenatal development, the impact of medication and/or social drug use on embryonic development, and causes of congenital malformations.
EFFECTS OF TERATOGENS
Teratogenic agents include, but are not limited to various maternal diseases, social drugs, prescription or over-the-counter (OTC) medications, stressors, and malnutrition.1,6,7 Exposure to a teratogen may increase the incidence of congenital malformations.1 Ideally, a woman who is pregnant or thinks she may be pregnant should ask her physician about the safe use of prescription and OTC medications and vitamin, mineral, and herbal supplements before taking them. Pregnant women should avoid the use of social drugs or illegal substances during pregnancy—especially during the first trimester, when the developing embryo is most vulnerable.
To prove that a specific agent is teratogenic means to show a high-frequency of congenital malformations in women exposed to a specific agent. This is difficult because of the limited ways in which teratogens can be studied. Research surrounding the study of teratogens is mainly conducted through animal and observational studies of human exposure.2 Observations from human exposure and recorded birth outcomes have prompted drug recalls and the development of identifying criteria for determining whether an agent is teratogenic in humans.2 Through both types of studies, medications and other agents known to cause birth defects are either removed from consumer markets and/or labeled with medical guidelines and warnings.2
An agent’s ability to produce a permanent fetal malformation depends on whether it can cross the placenta.1,4,7 Any drug or chemical substance given to a pregnant woman can cross the placenta to some degree, unless it is destroyed or changed in utero. Passage is also limited by decreased mobility from teratogens with a large molecular size and/or their lack of solubility.8 All teratogens increase the risk of harm to the developing embryo; however, some have a threshold level of exposure below which no harm is evident.9 The teratogenic effect is determined by several factors, including: timing or stage of embryonic development; the agent(s); dosage; and the genetic make-up of the embryo.10
MEDICATION USE
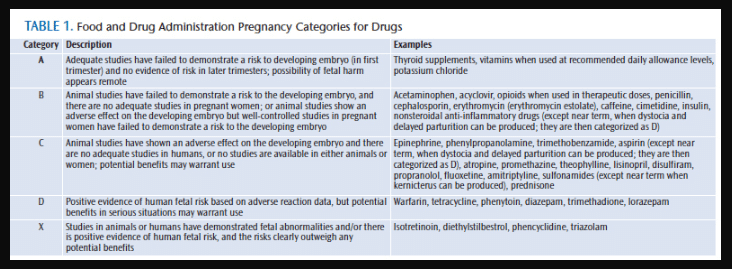
For some women, there are situations in which medication is necessary and appropriate to maintain health while under the care of a dentist or physician. In general, special consideration should be given when recommending or administering drugs—the benefit to the pregnant woman should outweigh the risk to the developing embryo, and a definite need should exist.3 In those situations, drug classifications defined by the FDA can be used to guide providers in prescribing medication. Prior to 1980, most medications included statements that use in pregnancy had not been approved. The FDA has since created five drug categories to better outline what is known about medication use during pregnancy (Table 1). A drug listed as Category A means that studies “failed to demonstrate risk to the developing embryo in any trimester.” Category B drugs have had no human studies reporting harm, but do have animal reproduction studies that “fail to demonstrate a risk to the developing embryo.”11 Dentists and dental hygienists should avoid administering or recommending drugs (eg, some local anesthetics, analgesics, and antibiotics) listed as category C, D, or X, as these pose a documented risk to a developing embryo.11 Category X drugs should not be used during pregnancy.3,11 Dental hygienists can consult the appropriate dental drug reference in order to determine FDA pregnancy drug categories while collecting medical histories or prior to the dentist prescribing a drug(s).
Fortunately, there are only a few medication types that are commonly used in dentistry and dental hygiene—analgesics and anti-inflammatories, antibiotics, local anesthetics, and sedatives. These medications are indicated when there is pain or high-risk infection exists in the mother. Analgesics and some anti-inflammatories can either be prescribed or purchased OTC. Animal studies of aspirin have shown defects involving the eyes, central nervous system, gastrointestinal tract, and skeletal system—while human studies have not been able to demonstrate an increase in congenital malformations.3,12
Aspirin is a category C/D drug, and, during the third trimester, can cause prolonged gestational time periods, complications during labor and delivery, decreased placental function, or increased risk of maternal or fetal hemorrhage.1,13 Nonsteroidal anti-inflammatory drugs have warnings to avoid use during pregnancy because, like aspirin, they have similar effects on the developing embryo—and, when given during the third trimester, can cause delayed delivery and other complications.3,12 Ibuprofen and naproxen animal studies have not shown adverse effects on the developing embryo and are pregnancy category B drugs; however, in a review of human studies by Burdan and Belzec,13 several related problems, including embryonic implantation disturbances, inhibition of parturition, and contraction of the ductus arteriosis leading to maternal pulmonary hypertension, were found.6 Gastroschisis (fetal organs developing outside of the abdominal wall) also is a congenital malformation often related to ibuprofen use.12 Acetaminophen is a pregnancy drug category B and is considered to be safe during pregnancy in low dosages, though excessive doses have been associated with fetal renal changes.3,12
Local anesthetics can cross the placenta.6 When given in high doses and during the last trimester, local anesthetic amides have been linked to fetal bradycardia, neonatal depression, and changes in fetal heart rates.3 Lidocaine, prilocaine, and etidocaine are listed as category B drugs because they have been tested in animals and had no teratogenic effects. The preferred local anesthetic for pregnant patients is lidocaine, as it is not associated with methemoglobinemia, as is prilocaine, and does not have a high lipid solubility like etidocaine.3 Bupivacaine is a category C local anesthetic, and has been shown to be teratogenic in animal studies using rats and rabbits.3,14 Mepivacaine is also a category C drug, but has not been tested.3
Antibiotics also are widely used to treat dental disease and some can cross the placenta. All tetracyclines can cross the placental membrane and deposit in the embryo’s bones and teeth. Fetal tetracycline exposure can result in yellow or grey staining of the primary and secondary dentition, and diminish growth of bones.3,15 Doxycycline has also been shown to cause tooth staining.15 Amoxicillin, azithromycin, cephalexin, clindamycin, erythromycin, metronidazole, and penicillin are listed under pregnancy drug category B. Side effects can be passed through breast milk (diarrhea, candidiasis, and allergic reaction).3
Sedatives—specifically, benzodiazepines used to treat anxiety—may lead to fetal abortion, malformations, intrauterine growth delays, functional deficits, carcinogenesis, and mutagenesis, and should not be used during pregnancy.3 Alprazolam, diazepam, lorazepam, midazolam, and triazolam are all pregnancy category D/X drugs.3 Use of nitrous oxide-oxygen analgesia in dental offices is important to consider for both pregnant patients and employees. Medical and dental health care workers who were exposed to even trace amounts of nitrous oxide had a significantly higher incidence of spontaneous abortion, congenital anomalies, altered immune responses, and birth defects in their children.16
SOCIAL DRUG USE
Social drug use, including tobacco and alcohol consumption, adversely affects the growth and development of the embryo. Psychoactive drugs or chemical substances that cross through blood-brain barriers and alter brain function can be used socially or by prescription.17–20
The nicotine in tobacco affects fetal growth, with maternal smoking being a well-established cause of intrauterine growth restriction and premature delivery.17–20 Nicotine constricts blood vessels in the uterus, restricting blood flow to the developing embryo and decreasing a healthy supply of oxygen and nutrients.19 Nicotine can also adversely affect the cell growth needed for development of the brain and mental capacity. Smoking during pregnancy also increases the incidence of prenatal mortality and morbidity.19
Infants born to mothers who consume alcohol are at risk for fetal alcohol syndrome (FAS). Streissguth and LaDue20 found that structural and functional impairments occurred in up to one half of infants born to alcoholic women. Chronic alcohol use (six drinks or more per day) and binge drinking (five or more drinks in succession) cause birth defects and problems with growth and brain development.17–20 Classic facial features of infants born with FAS include a smaller head circumference, short palpebral fissures, maxillary hypoplasia, and a smooth philtrum.6,17–20
ROLE OF DENTAL HYGIENISTS
Because oral health professionals treat a diverse patient population, including pregnant women, they need to understand the development of the fetal face, neck, and oral cavity in order to better communicate the underlying impact of teratogens on the development of these structures. While there are some elective or preventive therapies that can be postponed until after pregnancy, treatment of oral pain, periodontal diseases, caries, or other oral pathologic conditions may not be delayed.6
When at all possible, clinicians should wait to prescribe medication and prevent patient exposure to other environmental teratogens until after pregnancy. Sometimes a pregnant patient may present with dental disease, and medication is warranted. Whether prescribed or OTC, dental professionals need to stress the importance of seeking medical advice before taking any drugs (including herbal or vitamin supplements) during pregnancy. Clinicians can use the FDA-approved pregnancy drug categories when inquiring about medication usage.3,6
Some pregnant women must take medications to treat health conditions or maintain health during pregnancy, such as drugs to control asthma, epilepsy, high blood pressure, diabetes, or depression. These conditions, when untreated, could harm the woman and/or her developing embryo. Dental hygienists need to take a thorough medical history and discuss current medication usage, including OTC medications and dietary and herbal products.
During the treatment of pregnant women or women in their childbearing years, if doubt exists about the safety of a drug or procedure, dental hygienists should avoid administering or recommending drugs listed as category C, D, or X until the patient’s obstetrician is consulted.15,16 When drugs are administered in the dental office, clinicians should always check and monitor patient’s vital signs, including blood pressure, respiration, and pulse.
Dental hygienists can also ask open-ended questions, eliciting responses and creating dialog about social drug use, proper nutrition, and when to seek medical advice. Dental hygiene care should include providing oral health instruction and patient education on the harmful effects of smoking and alcohol intake on oral tissues and general and prenatal health. Dental hygienists can develop smoking cessation programs and support mothers who may be struggling to quit this habit during pregnancy. Substance abuse referrals should be given when pregnant patients list social drug use on their medical history.
CONCLUSION
Dental hygienists need to take thorough health histories with all patients, but especially women who are expecting or could be expecting, in order to minimize risks to the developing embryo. Understanding the cellular changes that occur during the stages of prenatal development can enable effective treatment in maternal dental disease so that minimal risk is placed on the patient and the developing embryo.
The CDC is working on improving the quality of information on medication use during pregnancy with a program called “Treating for Two: Safer Medication Use in Pregnancy.”21 The purpose of this program is to prevent birth defects and improve the health of pregnant women. The CDC’s partnership with the Organization of Teratology Information Specialists provides information, both in English and Spanish, for women and health care providers on the risks and safety of taking medication during pregnancy and breastfeeding.
Pregnant women are part of a unique patient population that requires dental hygienists to use critical thinking to identify risk of teratogens and medication use, and strategies for minimizing risk.
REFERENCES
- Bath-Balogh M, Fehrenback M. Illustrated Dental Embryology, Histology, and Anatomy. 3rd ed. St. Louis: Elsevier Saunders; 2011:19–48.
- Adam MP, Polifka JE, Friedman JM. Evolving knowledge of the teratogenicity of medications in human pregnancy. Am J Med Genet C Semin Med Genet. 2011;157C:175–182.
- Haveles EB. Applied Pharmacology for the Dental Hygienist. 6th ed. Maryland Heights, Missouri: Mosby Elsevier; 2011:300–307.
- Brent RL. Definition of a teratogen and the relationship of teratogenicity to carcinogenicity. Teratology. 1986;34:359–360.
- Centers for Disease Control and Prevention. Pregnancy. Available at: cdc.gov/ pregnancy /meds. Accessed November 22, 2014.
- Donaldson M, Goodchild JH. Pregnancy, breast-feeding and drugs used in dentistry. J Am Dent Assoc. 2012;143:858–871.
- Gilbert SF. Developmental Biology. 7th ed. Sunderland, Massachusetts: Sinauer Associates; 2003:694–696.
- Illsley NP, Hall S, Penfold P, Stacey TE. Diffusional permeability of the human placenta. Contrib Gynecol Obstet.1985; 13:92–97.
- Brent RL. The cause and prevention of human birth defects: what have we learned in the past 50 years? Congenital Anomalies. 2001;41(1):3–21.
- Larsson KS. Teratological aspects of dental amalgam. Adv Dent Res. 1992;6: 114–119.
- Jeske A. Mosby’s Dental Drug Reference. 11th ed. St. Louis: Elsevier Health Sciences; 2013:839.
- Torfs CP, Katz EA, Bateson TF, Lam PK, Curry CJ. Maternal mediations and environmental exposures as risk factors for gastroschisis. Teratology. 1996;54:84–92.
- Burdan F, Belzek A. Current opinions on embryotic and teratogenic effects of ibuprofen. Pol Merkur Lekarski. 2001;11:266–270.
- Wei JS, Jin ZB, Yin ZQ. Effects of local anesthetics on contractions of pregnant and non-pregnant rat myometrium in vitro. Acta Physiol Hung. 2014;101:228–235.
- Tredwin CJ, Scully C, Bagan-Sebastian JV. Drug-induced disorders of teeth. J Dent Res. 2005;84:596–602.
- Rowland AS, Baird DD, Shore DL, Weinberg CR, Savitz DA, Wilcox AJ. Nitrous oxide and spontaneous abortion in female dental assistants. Am J Epidemiol.1995;141:531–538.
- Alvik A, Heyerdahl S, Haldorsen T, Lindemann R. Alcohol use before and during pregnancy: a population-based study. Acta Obstet Gynecol Scand. 2006;85:1292–1298.
- O’Leary CM, Heuzenroeder L, Elliott EJ, Bower C. A review of policies on alcohol use during pregnancy in Australia and other English-speaking countries, 2006. Med J Aust. 2007;186:466–471.
- Powers J, McDermott L, Loxton D, Chojenta C. A prospective study of prevalence and predictors of concurrent alcohol and tobacco use during pregnancy. Matern Child Health J. 2013;17:76–84.
- Streissguth AP, LaDue RA. Fetal alcohol. Teratogenic causes of developmental disabilities. Monogr Am Assoc Ment Defic. 1987;8:1–32.
- Centers for Disease Control and Prevention. Treating for Two. Available at: cdc.gov/ pregnancy/ meds/treatingfortwo/index.html. Accessed November 22, 2014.
From Dimensions of Dental Hygiene. December 2014;12(12):47–50.
