
Incorporating the Use of Silver Diamine Fluoride
Following are strategies for implementing this minimally invasive option into the caries management armamentarium.
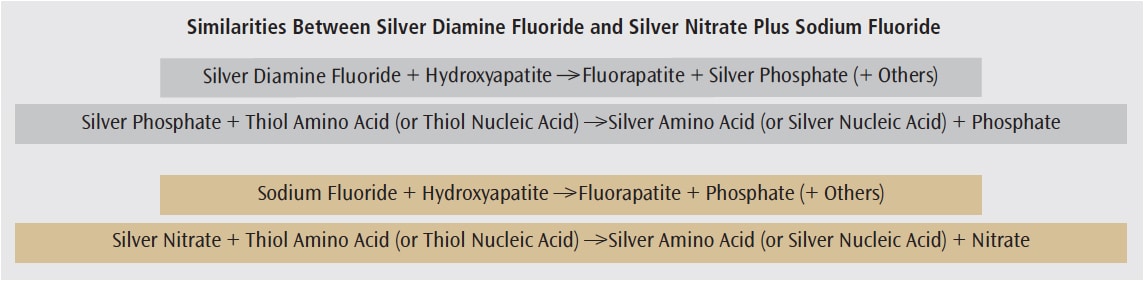
Silver diamine fluoride (SDF) has been used internationally for years to treat dentinal hypersensitivity and caries lesions.1–3 In 2014, it was cleared for use in the United States by the Food and Drug Administration (FDA) for treating sensitivity, and was granted the FDA’s breakthrough therapy designation for the arrest of dental caries in 2016.4,5 SDF is a cost effective, minimally invasive, and clinically simple treatment option for all patients. Moreover, it has the potential to more easily treat vulnerable populations, such as adults with special health-care needs.1 This article will provide an overview of its use in clinical practice.In its 38% formulation, SDF is composed of 25% silver ions (Ag+1) and 5% fluoride ions (F-1) dissolved in 8% amine (2NH3).1,2 Similar in structure to silver nitrate, plus fluoride,1 SDF’s biochemical interaction with tooth structure and cariogenic bacteria is also similar (Figure 1).1,2 Oral health professionals are knowledgeable about the major interaction of fluoride with tooth structure to form fluorapatite, but may be less aware of the antimicrobial role of silver.1,2,6–11 Silver reacts with thiol groups in the amino acids and nucleic acids to prevent the formation of disulfide bonds. These bonds are essential in forming and maintaining proper structure and function of proteins and nucleic acids. Improper structure and function of these molecules lead to bacterial cell death.1,2,6,7,8–10
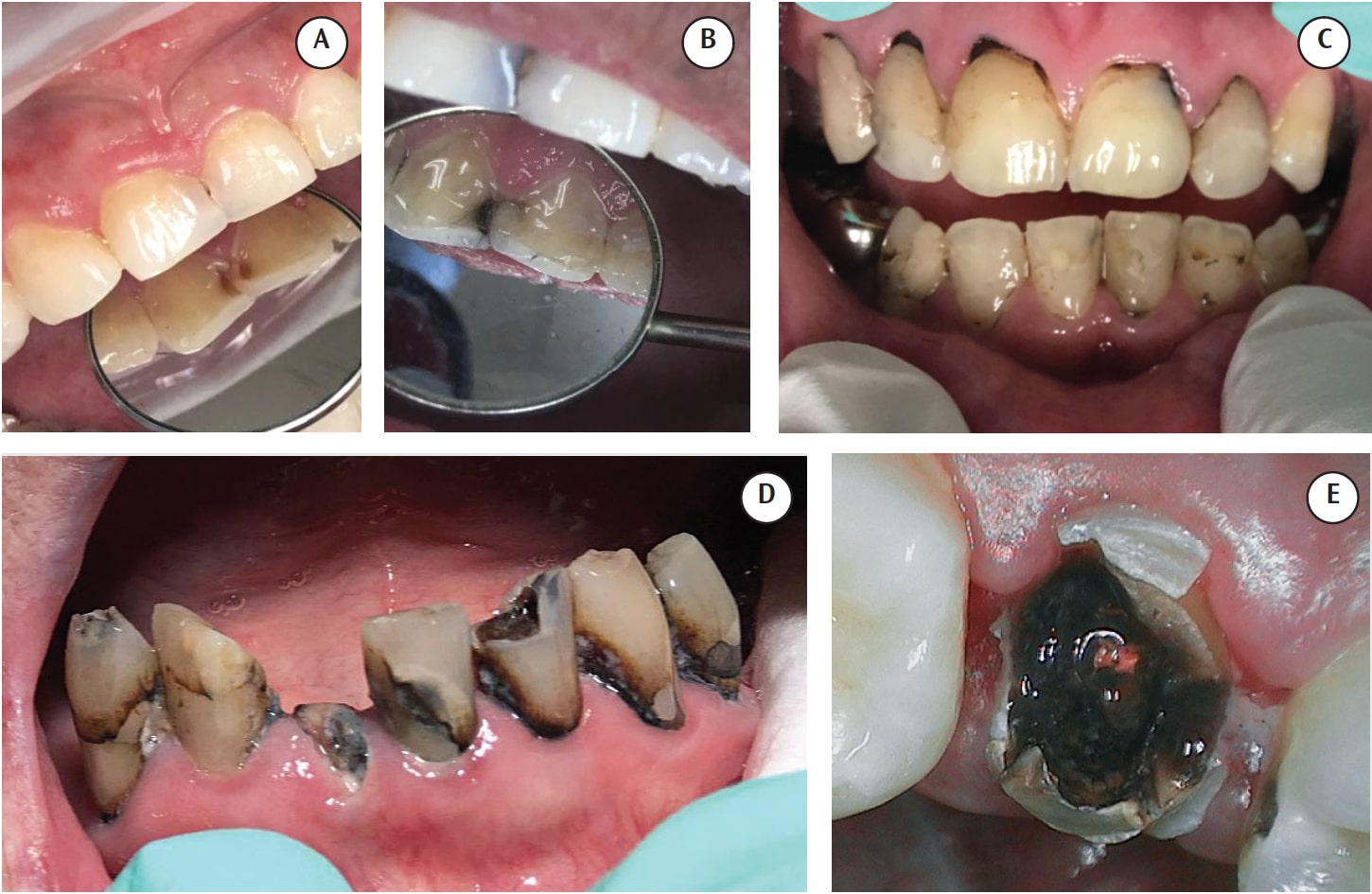
One consideration when deciding whether SDF is appropriate is the agent’s unesthetic properties, as it will permanently stain caries lesions black (Figure 2). Treatment can be made more esthetic with traditional therapies or the use of the silver modified atraumatic restorative technique at a later appointment.3 When assessing risks vs benefits, quality of life and the patient’s priority on physical appearance must be considered. It is also important to consider that acceptance of unesthetic staining may be greater than expected.
In a 2017 study of 98 mothers and 22 fathers, the parents were educated about the option of SDF treatment for their children, and were next asked about acceptance and preferences. In posterior cases, 67.5% of parents felt the staining was tolerable, and 53.6% answered that SDF treatment would be preferred over traditional treatment. For anterior applications, the percentages were 29.7% and 26.9%, respectively. When given the choice between SDF and treatment under general anesthesia, the percentages of parents who preferred SDF treatment were reported as 68% for posterior cases and 60.3% for anterior dentition.12
For noncooperative, medically compromised patients, SDF may be a safe and minimally invasive treatment option. Other patients who may experience benefits include patients on a wait list for operating room treatment, those who are noncompliant with oral hygiene, individuals with rampant or difficult-to-restore caries, patients with failing prosthodontic work, those who refuse extraction of nonrestorable teeth, and patients whose temporary conditions restrict them from traditional treatment. That noted, a patient does not have to fall into one of these categories to benefit from SDF therapy; this is a viable option for any patient who desires minimally invasive dentistry.
Information about pregnancy considerations for SDF therapy is not readily available at this time. This agent should not be used on patients with a silver allergy,1 and its use should be avoided in patients with open lesions, stomatitis, or ulcerative gingivitis. The staining of epithelium will eventually resolve with epithelial turnover. If it is subepithelial, however—as is possible in an open lesion—the staining can be permanent.1
Given its propensity to stain lesions black, one of the most important steps prior to the use of SDF is to obtain informed, written consent from the patient and/or parent/caregiver.
TAILOR THE TECHNIQUE
The technique for SDF delivery can be modified to meet the needs of individual patients. A suggested SDF protocol for patients with behavioral challenges is to dry, apply, and protect.
- Obtain informed consent
- Achieve the best isolation possible
- Dry the tooth with air and gauze
- Although not necessary, some clinicians prefer to remove caries with a spoon excavator
- Apply SDF with a microbrush
- Do not rinse
- Protect the site by brushing fluoride varnish or petroleum jelly over SDF-treated surfaces
The use of varnish will not “seal in” the SDF;1 in this protocol, varnish is used to create a short-term barrier between the treated surface and saliva. While there is little to no evidence to support partially removing the caries lesion,1,11 it is included in this protocol as there is no evidence to suggest partial caries removal causes harm. In addition, it may be easier for oral health professionals to monitor arrest with partial caries removal.
Clinicians are advised to check in 1 week to 3 weeks post-application to see if caries have been arrested. If the lesion is not arrested, SDF should be reapplied.13 If arrested, however, the agent should be reapplied every 3 months to 6 months, or until operative treatment can be performed.1 Although SDF has demonstrated its efficacy if applied every 6 months,14 as with all treatments, success is not guaranteed and regular follow-up is recommended. The recare schedule should be based on individual risks and results.
CLINICAL EFFICACY
Numerous studies demonstrate the effectiveness of SDF, and the list extends beyond what is mentioned in this article.1–3,6,7,10,11,14–18 Silver and fluoride ions can penetrate approximately 25 microns into enamel, and 50 microns to 200 microns into dentin.1 In fact, SDF has arrested lesions 150 microns deep.1 Caries lesions are more effectively arrested with multiple applications.1,15
Due to the availability of a popular Japanese SDF product, many studies were conducted in the late 1960s and early 1970s—but these papers have a high risk of bias, as they were provided by the manufacturer. Several are included in this article because their age and origin offer interesting insight. A split-mouth study of 10 patients (using 30 SDF-treated teeth and 10 control teeth) found 61% of caries arrested in 3 months, 69% at 6 months, 87% at 12 months, 88% at 24 months, and 97% at 30 months.16 When examining incidence of reduced sensitivity, one study stated that 64% of patients said SDF provided relief, 31% reported it as being fairly effective, and 5% said it was ineffective.17 A split-mouth study was done to determine how SDF placement prior to alloy placement affected the rate of recurrent caries. The researchers found a recurrence rate of 31% after 2 years in the control side, and 0% in the SDF-treated side.18
More recent studies have also demonstrated effectiveness. A study on 375 preschoolers divided the children into five groups. Groups 1 and 2 received SDF annually, and groups 3 and 4 received 5% sodium fluoride varnish every 3 months. Groups 1 and 3 had soft caries removed, while groups 2 and 4 did not. Looking at the arrest of caries lesions, the results demonstrated that annual application of SDF was more effective than application of 5% sodium fluoride every 3 months. This research also demonstrated that it was not necessary to remove soft caries.11
A 2017 study of 32 children examined 118 active caries lesions. Researchers applied SDF to the lesions, and the subjects returned for follow-up at 3 weeks and again at 3 months. Of the 102 lesions the team was able to follow the entirety of the study, 100 were arrested after the first application, and the remaining two were arrested after the second application.13 Another study of 373 subjects ages 6 to 15 demonstrated that application of SDF every 6 months was 77% effective in arresting active caries on canines and permanent first molars.14
Yet another group looked at the effectiveness of SDF in arresting active root surface caries in a geriatric population. Eighty-three older adults were divided into three groups: annual application of soda water (control), annual application of SDF, and annual application of SDF, plus potassium iodide. The team reviewed 100 lesions over 30 months and found that 45% of the lesions were arrested in the control group. By comparison, 90% of the lesions in the SDF group were arrested, and in the SDF, plus potassium iodide group, 93% of the lesions were arrested.19
FURTHER CONSIDERATIONS
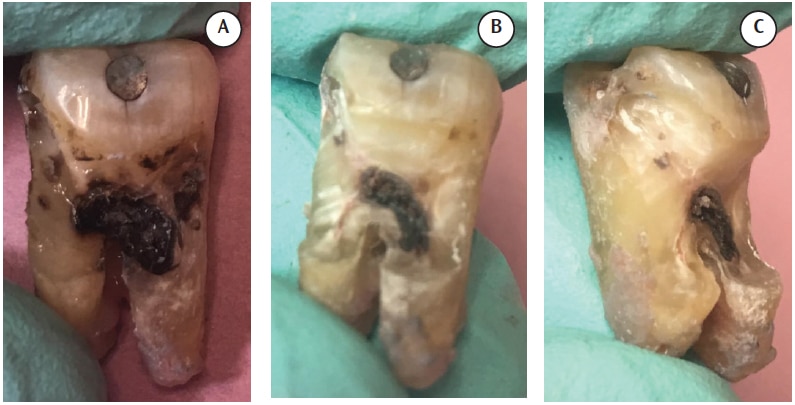
In large quantities, silver can be nephro/hepatotoxic and can cause intestinal irritation and graying of the sclera.7 It can also cross the blood-testis barrier. Only minimal amounts of silver are used in dental treatment with SDF; thus, clinicians who adhere to recommended maximum dosages should be able to avoid these problems.1 More realistic adverse effects include taste-induced nausea, pulpal irritation, and the aforementioned staining. Another consideration is that because SDF penetrates deep into dentin, if the caries extends to the pulp, the agent can, as well (Figure 3).
As noted, staining is the major adverse effect—and SDF can stain more than just teeth. It can also stain soft tissues, restoration margins, fingernails, skin, clothing, and operatory surfaces. The stain will dissipate when the epithelium turns over; that means about 14 days in the oral mucosa, a little longer on skin, much longer on nails, and permanent staining on the tooth, countertops, and clothing. The extent of staining and the length of staining vary significantly among individuals.
One clinical protocol recommends rinsing if the procedure calls for bonding to a direct restoration.1 Some studies suggest that SDF does not affect the bonding of glass ionomers and composites.20,21 In countries where SDF with potassium iodide is used, clinicians are advised to rinse off the precipitate prior to bonding.21
CONCLUSION
Despite widespread global use for years, there is much to learn about SDF. The intention of this article was to provide basic information about its clinical application. Through its ease of application and cost effectiveness, SDF has the potential to improve the oral heath of many underserved patient populations. This agent is not a miracle drug. However, it is a minimally invasive option for all patients—and, for some, perhaps the best and only option.
The author would like to thank Jeremy Horst, DDS, PhD, for his help with this manuscript.
REFERENCES
- Horst JA, Ellenikiotis H, UCSF Silver Caries Arrest Committee, Milgrom PM. UCSF protocol for caries arrest using silver diamine fluoride: rationale, indications, and consent. J Calif Dent Assoc. 2016;44:16–28.
- Rosenblatt A, Stamford TC, Niederman R. Silver diamine fluoride: a caries “silver-fluoride bullet.” J Dent Res. 2009;88:116–125.
- MacLean J. Top 5 misconsceptions of silver diamine fluoride. Dental Town. 2017;89–93.
- Elevate Oral Care. Breakthrough Therapy Designation for Silver Diamine Fluoride granted by FDA. Available at: advantagedental.com/Media/zgefi04s.pdf. Accessed January 12, 2018.
- Decisions in Dentistry. Silver Diamine Fluoride Receives New FDA Designation. Available at: decisionsindentistry.com/article/silver-diamine-fluoride-receives-new-fda-designation/print/ posted. Accessed January 12, 2018.
- Alvear BA, Horst JA, Hirsch JP, Duffin S, Wong A, Young DA. Arresting caries. Dimensions of Dental Hygiene. 2016;14(7):61–64.
- Prabhu S, Poulose EK. Silver nanoparicles: mechanism of antimicrobial action, synthesis, medical applications, and toxicity effects. Int Nano Lett. 2012;2:32.
- Hernandez-Sierra JA, Ruiz F, Pena DC, et al. The antimicrobial sensitivity of Streptococcus mutans to nanoparticles of silver, zinc oxide and gold. Nanomedicine. 2008;4:237–240.
- Liau SY, Read DC, Pugh WJ, Furr JR, Russell AD. Interaction of silver nitrate with readily identifiable groups: relationship to antibacterial action of silver ions. Lett Appl Microbiol. 1997;25:279–283.
- Mei ML, Chu CH, Low KH, Che CM, LO EC. Caries arresting effect of silver diamine fluoride on dentine carious lesion with S. Mutans and L acidophilus duel species cariogenic biofilm. Med Oral Pato Oral Cir Bucal. 2013;18:e824–31.
- Chu CH, Lo EC, Lin HC. Effectiveness of silver diamine fluoride and sodium fluoride varnish in arresting dentin caries in Chinese preschool children. J Dent Res. 2002;81:767–770.
- Crystal YO, Janal MN, Hamilton DS, Niederman R. Parental perceptions and acceptance of silver diamine fluoride staining. J Am Dent Assoc. 2017:148:510–518.
- Clemens J, Gold J, Chaffin J. Effect and acceptance of silver diamine fluoride treatment on dental caries in primary teeth.J Public Health Dent. July 27, 2017. Epub ahead of print.
- Llorda JC, Rodriguez A, Ferrer B, Menardia V, Ramos T, Morato M. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36-month clinical trial. J Dent Res. 2005;84:721–724.
- Yee R, Holmgren C, Mulder J. Lama D. Walker D van Palenstein Helderman W. Efficacy of silver diamine fluoride for arresting caries treatment. J Dent Res. 2009;88:644–647.
- Nishino M. Studies on the topical application of ammoniacal silver fluoride for the arrest of dental caries. Osaka Daigaku Shigaku Zasshi. 1969;12:1–14.
- Aono M, Munemoto K, Okada H, et al. Effect of ammonical silver fluoride on cervical hypersensitivity. Jap J Conserv Dent.1967;10:31–36.
- Shimizu A. Effect of diamine silver fluoride on recurrent caries. Jap J Conserv Dent. 1974;17:183–201.
- Li R, Lo EC, Liu BY, Wong MC, Chu CH. Randomized clinical trial on arresting dental root caries through silver dimaine fluoride applications in community dwelling elders. J Dent. 2016;51:15–20.
- Quock RL, Barros JA, Yang SW, Patel SA. Effect of silver diamine fluoride on microtensile bond strength to dentin. Oper Dent. 2012;37:610–616.
- Knight GM, McIntyre JM, Mulyani. The effect of silver fluoride and potassium iodide on the bond strength of auto cure glass ionomer cement to dentine. Aust Dent J. 2006;51:42–45.
From Dimensions of Dental Hygiene. March 2018;16(3):29-30, 32.
The best videos just on https://ahmedxnxx.com….

{kind=link}