Identify Moderate Caries Risk
Effective caries risk assessment and management are integral to helping your patients reduce their caries risk.
This course was published in the August 2012 issue and expires August 31, 2016. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify evidence-based methods for determining caries risk.
- Detail risk factors specific to the patient at moderate risk of caries.
- Discuss appropriate methods to reduce caries risk.
- Explain strategies for treatment of carious lesions.
Dental caries affects more than 80% of Americans, many of whom have little or no access to care.1 It remains one of the most common preventable diseases among children in the United States.2 Untreated dental caries significantly impacts health and can affect sleeping, eating, speaking, and the ability to concentrate. It can also be fatal.1,3 Oral health professionals are on the front lines of this battle against caries. Dental hygienists are an integral part of the oral health care team and they are responsible for assessing patient needs prior to providing care. Simply informing patients of their disease risk, however, is not enough. Dental hygienists must also provide planned dental hygiene care in addition to counseling patients about disease risk reduction strategies.4
Caries management by risk assessment (CAMBRA) provides guidelines to help oral health practitioners manage dental caries in their patients. The principles of CAMBRA include: assessing and determining each patient’s risk of caries, helping the patient reduce this risk, managing current disease, and providing minimally invasive restorative procedures to repair damaged tooth surfaces.5,6 To effectively manage caries disease, the level of risk must first be identified.6 For comprehensive guidelines on assessing and managing caries in patients of all ages, review the October 2007 issue of the Journal of the California Dental Association.7
Research has shown that humans are not born with caries-causing pathogens in the oral cavity.8 Young children are colonized with caries-causing bacteria before their immune systems become mature enough to resist the infectious pathogens.8 Transmission of caries-related bacteria occurs unknowingly from parents, primary caregivers, or siblings through vehicles such as spoons, kisses, fingers, and shared toys.8 Pregnant women and primary caregivers of young children should be advised to reduce their own risk and avoid transmitting the bacteria to their infants and toddlers.
 PERFORMING A CARIES RISK ASSESSMENT
PERFORMING A CARIES RISK ASSESSMENT
Clinicians assess and address risk for disease during most patient care appointments. To assess caries risk, clinicians check for signs of caries, such as white spot lesions (the more subtle, early signs of caries infection), carious lesions in radiographic images, and recent restorative care. The California Dental Association (CDA) has created a comprehensive caries risk assessment form, which is available with the web version of this article.5 Once a caries assessment tool is in place and data have been collected, critical thinking and clinical decision-making create an effective risk assessment. The CDA caries risk assessment form helps clinicians determine whether a patient is at extreme, high, moderate, or low risk of caries.5,6 Individuals at high or extreme caries risk present with at least one of four disease indicators: visible active lesions, active white spot lesions, recent history of restorations due to caries, and approximal radiographic carious lesions.5 Caries management for these patients includes therapeutic and restorative protocols.
Patients at moderate and low risk of dental caries are identified by the number of risk factors and protective factors present. Currently, the following nine factors are known to increase the risk of caries: medium or high numbers of Streptococcus mutans and Lactobacillus in the oral cavity; visible, heavy plaque on the teeth; frequent snacking; deep pits and fissures; recreational drug use; inadequate saliva flow; presence of saliva reducing factors; exposed roots; and wearing of orthodontic appliances.5,6 The more risk factors present, the higher the risk. Conversely, the more protective factors present, the lower the caries risk. Protective factors include access to fluoridated community water supply; daily use of fluoride toothpaste and fluoride mouthrinse; brushing with a prescription-strength fluoride dentifrice; fluoride varnish or other topical fluoride application within the past 6 months; use of chlorhexidine; chewing xylitol gum or lozenges at least four times per day over the past 6 months; using a calcium/phosphate paste during the past 6 months; and adequate saliva flow. Patients at low risk of caries are generally told to “keep up the good work,” but they should be advised about the behaviors that are reducing their risk so their status can be maintained.
Acid challenges resulting from fermentable carbohydrate consumption can increase caries risk. Hormone changes in adolescence and challenges from low saliva flow due to medication use, illness, or radiation therapy can alter the buffering capacity of the saliva and remineralization, negatively impacting caries risk in spite of a low caries-related bacterial count.9 Prevention education is key to maintaining a low caries risk.
PATIENT AT MODERATE RISK
Patients at moderate risk of caries often have a history of caries, although the disease process may be currently controlled. They may have white spot lesions that are hard, glossy, brown, or even black—indicating remineralization has taken place.10
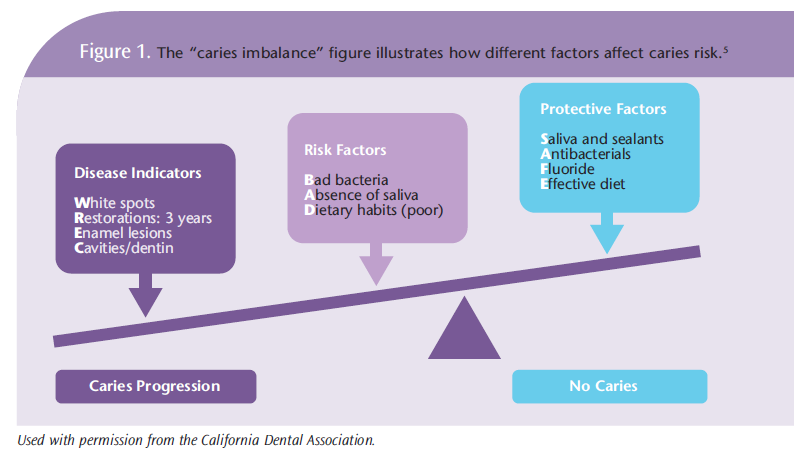
This profile describes the majority of patients in dental practices. Patients at moderate risk need to be educated about their risk of future caries activity and the strategies necessary to prevent new carious lesion formation. A history of low caries risk does not guarantee a caries-free future. Disease indicators carry much more weight than risk factors and preventive factors (Figure 1). A patient at moderate risk of caries generally displays no disease indicators, but more risk factors than protective factors. A patient at low caries risk displays more protective factors than risk factors. To remain caries free or inhibit caries progression, protective factors must outweigh risk factors. Adding fluoride to drinking water, toothpaste, and oral rinsing to the “no caries” side of the scale reduces caries risk. Thorough daily plaque removal, applying pit and fissure sealants, and healthy snacking habits also reduce caries risk. A change in medical history, such as taking medications that reduce saliva flow, may add weight to the “caries progression” side of the scale, shifting the caries balance.5,6 The patient at moderate caries risk has the scale carefully balanced, and any change in diet, oral hygiene, or oral environment can shift that balance, resulting in new carious lesions.
![]() RISK REDUCTION AND TREATMENT STRATEGIES
RISK REDUCTION AND TREATMENT STRATEGIES
Prevention includes daily fluoride use, maintaining neutral pH, and limiting fermentable carbohydrates between meals.
Applying topical fluoride to moderate risk caries patients at recare visits is like adding weight to the “no caries” side of the caries balance scale. Patients with medically-induced xerostomia should be encouraged to hydrate frequently; avoid sugar-laden mints, gums, and medications; incorporate xylitol-containing products as frequently as possible; and receive regular dental care visits and fluoride application.11 Patients should be questioned about their use of antacids because they often contain sugar, and if consumed at night when saliva flow is lowest, they may significantly lower the pH and increase demineralization.
The CAMBRA protocol states that carious lesions should be treated as soon as they are detected.6,9 The minimally invasive repair of carious lesions, in conjunction with antimicrobial therapy to reduce the bacterial load, is recommended.12 Carious lesions detected in radiographs or through visual examination that have not penetrated the dentoenamel junction can be reversed and remineralized with the addition of fluoride, calcium, phosphate, and acid-neutralizing strategies.13 A systematic review of the literature showed that prescription fluoride toothpastes (5,000 ppm) provided greater remineralization and preventive benefits than 1,500 ppm fluoride dentifrices.13 The review suggested a positive dose response between exposure to higher fluoride levels and increased remineralization rates on enamel and root surfaces, which could particularly benefit patients at moderate caries risk. Glass ionomer sealants add fluoride to the tooth and saliva, which can enhance the antimicrobial and strengthening properties of the fluoride.14
CASE STUDY
Mrs. Smith, a 68-year-old woman presented with a history of chronic periodontitis that required surgical intervention. She had generalized 1 mm to 3 mm root exposure and 2 mm to 3 mm pocket depths.
Mrs. Smith had gold crowns and gold onlays on her molars but no new restorations placed in the past 3 years. Saliva flow was watery and clear. Her oral hygiene was meticulous. She used an interdental cleaning aid, an interdental brush, and a 5,000 ppm fluoride dentifrice daily. She visited her dental hygienist every 3 months for periodontal maintenance. Her medical history included a battle with breast cancer, high blood pressure, and hyperlipidemia. Oral-related side effects of the Tamoxifin prescribed for breast cancer suppression can include nausea, vomiting, pharyngeal irritation, and cough, although Mrs. Smith did not experience these side effects.15 The medications prescribed to control her blood pressure and cholesterol can cause xerostomia. She had been a carefully balanced patient at moderate caries risk for several years. But Mrs. Smith’s husband had recently died and she had begun taking an antidepressant (selective serotonin reuptake inhibitor), which caused xerostomia. During her regular 3-month visit, four vertical bitewing radiographs revealed a large carious lesion on the molar abutment of her three-unit bridge.
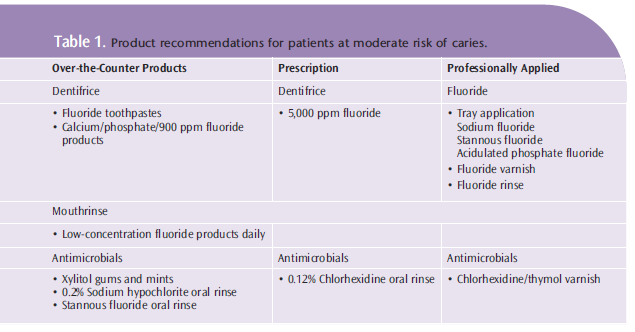
This is a patient at moderate caries risk whose status quickly changed when medication use and illness drastically increased her vulnerability. Though it would have been difficult to predict the death of her husband, based on the many risk factors of exposed roots, caries history, and medication-induced xerostomia, her dental team should have considered additional strategies to help reduce caries risk (Table 1). The professional application of fluoride at each recare appointment would have further increased remineralization of the root surfaces.13 Studies show that chlorhexidine/ thymol varnish may reduce the incidence of root caries in adults.11 Strategies for maintaining a neutral pH should have been discussed with the patient since she was already taking two medications that may reduce saliva flow.
The critical pH of the root surface is close to neutral, about 6.5.9 In Mrs. Smith’s case, her medication-induced dry mouth may have played a key role in the sudden change in caries activity. Saliva possesses key factors integral to the maintenance of a neutral, healthy oral environment.5,9 Decreased saliva flow reduces the ability of the saliva to buffer acids and the acidophilic, caries-causing bacteria began to proliferate. The presence of acidic foods, beverages, and snacks contribute to a drop in the critical pH below 6.5. This creates an environment for demineralization of the fragile root surface.5,9 Sugar-free gums, mints, sprays, and even rinsing with water after acid challenges can increase the buffering capacity of the saliva—minimizing the chance of acid damage to the enamel and fragile root surfaces.
CONCLUSION
Just like periodontal diseases and oral cancer, the risk of dental caries is dynamic. Each patient should be assessed for changes to disease risk at all recare appointments. In spite of increased understanding of caries etiology and the wide availability of preventive and therapeutic treatments, dental caries is still one of the most common preventable diseases in the United States. The goal of each oral health care professional should be to educate patients about how to stop the spread of this disease. Utilizing a caries risk assessment form will help dental hygienists quickly identify caries risk factors, as well as appropriate protective factors that can be added to the patient’s caries prevention regimen. Understanding the personal, physical, and financial challenges of patients will also help determine the best preventive and therapeutic recommendations. Dental hygienists are key players in reducing caries risk in their patients and their families, which will lead to a cascade of improved oral health.
REFERENCES
- Edelstein BL. The dental caries pandemic anddisparities problem. BMC Oral Health. 2006;6(Suppl1):S2.
- Beltrán-Aguilar ED, Barker LK, Canto MT, et al.Surveillance for dental caries, dental sealants, tooth retention, edentulism, and enamel fluorosis—United States, 1988-1994 and 1999-2002. MMWR Surveill Summ. 2005;54:1–43.
- Otto M. For want of a dentist. The Washington Post. February 28, 2007:B01.
- American Dental Hygienists’ Association.Standards for clinical dental hygiene practice.Available at: www.adha.org/downloads/adha_standards08.pdf. Accessed July 24, 2012.
- Doméjean S, White JM, Featherstone JD.Validation of the CDA CAMBRA caries risk assessment—a six-year retrospective study. J Calif Dent Assoc. 2011;39:709–715.
- Featherstone JD, Doméjean-Orliaguet S, JensonL, Wolff M, Young DA. Caries risk assessment in practice for age 6 through adult. J Calif Dent Assoc. 2007;35:703–713.
- Journal of the California Dental Association.October 2007. Available at: http:// cda.org/library/cda_member/ pubs/ journal/ jour1007/index.html. Accessed July 26, 2012.
- Berkowitz RJ. Streptococci: acquisition and transmission. Pediatric Dent. 2006;28:106–109.
- Peters M. Strategies for noninvasive demineralized tissue repair. Dent Clin of North Am. 2010;54:507–525.
- Wilkins EM. Clinical Practice of the Dental Hygienist. 9th ed. Baltimore: Lippincott, Williams& Wilkins; 2005:393–401.
- Rethman MP, Beltrán-Aguilar ED, Billings RJ, et al. Nonfluoride caries-preventive agents.Executive summary of evidence-based clinical recommendations. J Am Dent Assoc. 2011;142:1065–1071.
- Kidd EAM. Clinical threshold for carious tissue removal. Dent Clin of North Am. 2010;54: 541–549.
- Gibson G, Jurasic MM, Wehler CJ, Jones J.Supplemental fluoride use for moderate and high caries risk adults: A systematic review. J Public Health Dent. 2011;71:171–184.
- Beiruti N, Frencken JE, van’t Hof MA, Taifour D, van Palenstein Helderman WH. Caries preventive effect of a one time application of composite resin and glass ionomer sealants after 5 years. Caries Res. 2006;40:52–59.
- Medline Plus. Drugs, supplements, and herbal information. Available at: www.nlm.nih.gov/medlineplus/druginformation.html.Accessed July 24, 2012.
From Dimensions of Dental Hygiene. August 2012; 10(8): 14-17.
