
General Anesthesia in the Treatment of Early Childhood Caries
While the rise in tooth decay among preschoolers has increased the use of general anesthesia during restorative care, the financial and societal costs are great.
The American Academy of Pediatric Dentistry1 (AAPD) defines early childhood caries (ECC) as “the presence of one or more decayed (noncavitated or cavitated lesions), missing (due to caries), or filled tooth surfaces in any primary tooth in a child under the age of 6.” Untreated, ECC can irreversibly destroy the dentition, cause abscesses, and lead to serious illness.2 Infection and pain due to ECC can impair growth; cause speech, learning, and eating problems; increase school absenteeism; and negatively affect quality of life.2
Although most children with ECC can be successfully treated in the dental office, some require complete sedation provided by general anesthesia (GA), which is administered in a hospital setting. The most common indication for GA at this age is extensive caries.3 As the prevalence of ECC continues to grow, so has the use of GA to treat pediatric patients.4 While GA can help provide comprehensive care in a timely and effective manner, it is costly and presents health risks, as do all forms of anesthesia.5
PREVALENCE
According to the United States Centers for Disease Control and Prevention, the number of children between the ages of 2 and 5 with tooth decay has increased 15% in the past decade.6 More than 40% of children have caries by the time they reach kindergarten.7 Although ECC is disproportionately concentrated among socially disadvantaged children, there has been a significant increase among nonpoor children as well.6 In fact, nonpoor children between the ages of 2 and 4 experienced the largest increase in ECC between the periods of 1988 and 1994, and 1999 and 2004—rising from 18% in 1988 to 26% in 2004.6
EARLY CHILDHOOD CARIES RISK FACTORS
There are many reasons why preschoolers suffer from such extensive tooth decay. ECC can be caused by frequent snacking, especially on caries-promoting foods. Excessive bottle or sippy cup use containing liquids such as milk, formula, fruit juice, and soda, especially near bedtime or naptime, can lead to ECC.8 Another factor is the choice of bottled water for children, rather than fluoridated tap water. In addition, parents may have become more lax about toothbrushing habits, reflecting a change in parenting styles.9 A 2001 survey of pediatric dentists indicated that children were less cooperative than in the past, and the study authors attributed this finding to changes in parenting styles, primarily a failure of parents to set limits on children’s behavior.9 Parents who share utensils with their children or “cleanse” a pacifier or toy with their mouth, may transfer the caries-promoting bacteria Streptococcus mutans through their saliva to the child.10 Finally, the cost of dental care is a barrier to families of lower socio-economic status. Children between the ages of 2 and 5, who have not visited a dentist within the past 12 months, are more likely to have caries in their primary teeth than those who have received professional dental care during the same time frame.6
CONSEQUENCES AND COST
In addition to pain and infection, ECC can affect speech and communication, eating and nutrition, sleeping, playing, and learning.11 American children age 5 to 7 lose more than 7 million school hours annually because of dental problems and/or visits, many of which are due to caries that began when they were preschoolers.11 A previous history of caries is the greatest indicator of future decay in both primary and permanent dentitions.11
 Due to the young age of children affected by ECC and their extensive dental needs, restorative treatment may be provided in an operating room under GA.12 GA is a controlled state of unconsciousness that eliminates awareness, movement, and discomfort during dental treatment. The AAPD approves the use of GA for treating rampant forms of ECC.4,12 GA can also be helpful for children who are uncooperative, fearful, or anxious; for the very young who do not understand how to cooperate; and for patients with special health care needs.13
Due to the young age of children affected by ECC and their extensive dental needs, restorative treatment may be provided in an operating room under GA.12 GA is a controlled state of unconsciousness that eliminates awareness, movement, and discomfort during dental treatment. The AAPD approves the use of GA for treating rampant forms of ECC.4,12 GA can also be helpful for children who are uncooperative, fearful, or anxious; for the very young who do not understand how to cooperate; and for patients with special health care needs.13
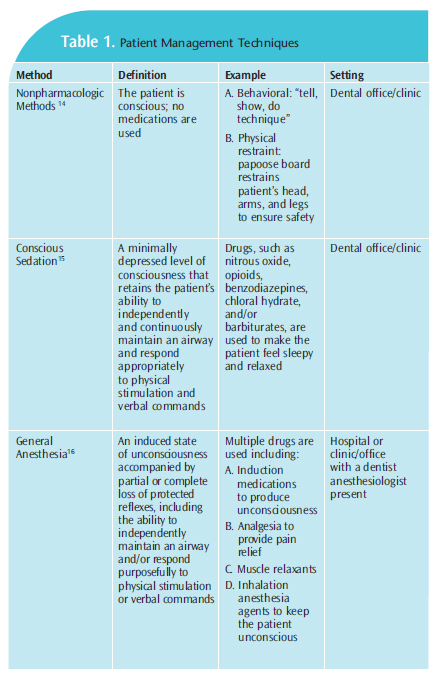
When treating young, uncooperative children with extensive dental needs, dental professionals have traditionally relied on three different patient management strategies (Table 1).14–16 Nonpharmacologic techniques include behavioral methods, such as “tell, show, do,” or using protective stabilization to protect the child from sharp instruments. The second method is conscious sedation (CS), which uses medications, including nitrous oxide, opioids, benzodiazepines, chloral hydrate, and/or barbiturates, to help children become relaxed or drowsy. Unlike GA, CS is not intended to make the patient unconscious or unresponsive. However, CS does not provide long-lasting effects, which may result in the need for multiple appointments to complete treatment.17 The final option is GA, which is considered a more compassionate method for treating children who cannot cooperate than the use of protective stabilizers, such as a papoose board.18 However, GA has risks.19 Using GA in healthy children can cause vomiting and nausea.19 In very rare cases, GA may result in brain damage or death.19 Parents requesting GA for recare appointments because, “my child cried at the last visit,” clearly do not understand the indications, risks, benefits, limitations, or costs of GA.9
Treatment of ECC is expensive and often involves extensive restorative care and/or extraction of teeth. The direct costs of ECC are difficult to document because information is not collected on related medical and dental services, however, estimates of cost are possible. The Medical Expenditures Panel Survey found that 19.4% of children in the US under the age of 5 had dental expenditures in 2006—totaling $729 million.11 When GA is used for dental treatment, the cost may increase anywhere from $1,500 to $6,000.11,20 The total amount depends on the time required in the operating room, in addition to the costs of dental treatment. The majority of cases using GA do not require an overnight hospital stay, although, treatment under these conditions still adds considerably to the cost of care, with payment coming from a variety of sources including public insurance (primarily Medicaid), private insurance, and private pay.
Demand for the use of GA in the dental treatment of young children is growing. A New York State study of ECC-related visits to emergency departments noted that in 2004, 34.9% of the patients in the study were treated under GA.21 This percentage increased to 75.2% in 2008.21 In 2010, the Seattle Children’s Hospital built a surgical wing because of the increased demand for oral surgery among preschoolers.22 The dental surgery center at Nationwide Children’s Hospital in Columbus, Ohio, has three operating rooms that were used to treat approximately 2,525 children in 2011—a 6% increase from 2010, according to Megann Smiley, DDS, a dentist anesthesiologist at the facility. Smiley reported that the average age of patients was 4, and most were treated for decay in six teeth to eight teeth, with the most severe cases involving 12 teeth to 16 teeth.
Tens of thousands of young children in the US undergo restoration and extraction of teeth under GA annually.23 The absolute numbers are unknown because there is no collective information compiled. Estimates are based on Medicaid records for children treated in hospitals. In North Carolina, more than 5,500 children received GA for dental services during a 2-year period.12 In Louisiana, more than 2,100 Medicaid-covered children received dental treatment under GA in a 1-year period; 60% were 3 years old or younger.24
In addition, the wait for GA or sedation services for children requiring dental treatment has increased in some areas to 1 month to 2 months.25 This is concerning because early treatment of decay is imperative to prevent further tooth destruction, tooth loss, and infection. Children with a history of ECC are susceptible to the development of new caries, even after comprehensive oral rehabilitation with GA.2 Retreatment rates have been reported as high as 50%.3
PREVENTION
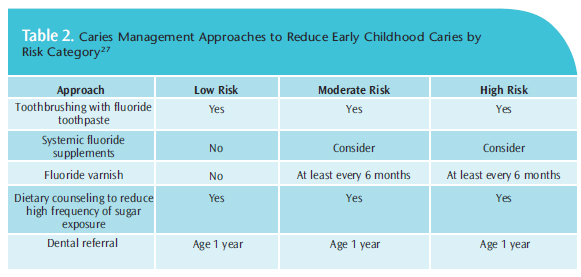
ECC is preventable and easily treated when diagnosed early.26 It is vital that dental hygienists educate at-risk children and their caregivers about prevention strategies. To monitor children’s teeth for ECC, the AAPD recommends that all children begin regular dental visits by 1 year of age. At a child’s first appointment, a caries risk assessment should be performed so that recommendations can be made to parents (Table 2).27 Parents should receive nutritional counseling to reduce the frequency of snacking and sugar exposure. Suggestions can be offered to substitute sugary snacks with less caries-promoting options. Replacing milk or juice in a bottle or sippy cup with water immediately before naptime and bedtime can be suggested. Dental hygienists must encourage parents to offer children fluoridated tap water instead of bottled water.
 Parents also need to be taught how to deliver effective oral care to their children. Dental hygienists must emphasize that for children age 2 and younger, parents should brush the teeth for them, twice daily, using a “smear” of fluoride toothpaste. At age 2, the amount of toothpaste should be increased to a pea-size dollop, brushing twice daily. Parents should also floss their child’s teeth, especially if overcrowding exists. Educating parents to avoid saliva-sharing behaviors to help prevent early colonization of Streptococcus mutans is also necessary. Children will not voluntarily alter their diet or improve oral hygiene habits. The responsibility for these necessary changes rests with the parent or caregiver. Dental hygienists need to actively pursue parents and caregivers to promote a preventive agenda, emphasizing termination of night time nursing habits, use of fluoride, increased toothbrushing by the parent, and regular professional dental visits. Aggressive preventive measures for high-risk children are less costly than repeated treatment under GA. It also frees up hospital personnel and resources to attend to other pediatric cases.
Parents also need to be taught how to deliver effective oral care to their children. Dental hygienists must emphasize that for children age 2 and younger, parents should brush the teeth for them, twice daily, using a “smear” of fluoride toothpaste. At age 2, the amount of toothpaste should be increased to a pea-size dollop, brushing twice daily. Parents should also floss their child’s teeth, especially if overcrowding exists. Educating parents to avoid saliva-sharing behaviors to help prevent early colonization of Streptococcus mutans is also necessary. Children will not voluntarily alter their diet or improve oral hygiene habits. The responsibility for these necessary changes rests with the parent or caregiver. Dental hygienists need to actively pursue parents and caregivers to promote a preventive agenda, emphasizing termination of night time nursing habits, use of fluoride, increased toothbrushing by the parent, and regular professional dental visits. Aggressive preventive measures for high-risk children are less costly than repeated treatment under GA. It also frees up hospital personnel and resources to attend to other pediatric cases.
CONCLUSION
ECC has tremendous impact on affected children and their families. It also puts an enormous strain on the health care system and society. Early, preventive dental visits for children at high risk of developing caries can reduce the need for restorative care, thereby decreasing dental caries-related treatment costs and the need to use GA.
REFERENCES
- American Academy of Pediatric Dentistry, American Academy of Pediatrics,American Academy of Pediatric Dentistry Council on Clinical Affairs. Policy on EarlyChildhood Caries (ECC): Classifications, Consequences, and Preventive Strategies.Available at: www.aapd.org/media/Policies_Guidelines/P_ECCClassifications.pdf.Accessed September 17, 2012.
- US Department of Health and Human Services, National Institute of Dental andCraniofacial Research, US Public Health Service. Oral Health in America: Report of theUS Surgeon General. Rockville, Md: DHHS; 2000.
- Sheller B, Williams BJ, Hays K, Mancl L. Reasons for repeat dental treatment undergeneral anesthesia for the healthy child. Pediatr Dent. 2003;25:546–552.
- Hicks CG, Jones JE, Saxen MA, et al. Demand in pediatric dentistry for sedation andgeneral anesthesia by dentist anesthesiologists: a survey of directors of dentistanesthesiologist and pediatric dentistry residencies. Anesth Prog. 2012;59:3–11.
- Wilson W. Pharmacological management of the pediatric dental patient. PediatrDent. 2004;26:131–136.
- Dye BA, Tan S, Smith V, et al. Trends in oral health status: United States, 1988-1994and 1999-2004. National Center for Health Statistics. Vital Health Stat 11. 2007:1–92.
- Pierce KM, Rozier RG, Vann WF Jr. Accuracy of pediatric primary care providers’screening and referral for early childhood caries. Pediatrics. 2002;109:E82–2.
- Dye BA, Thorton-Evans G. Trends in oral health by poverty status as measured byHealthy People 2010 objectives. Public Health Rep. 2010;125:817–830.
- Casamassimo PS, Wilson S, Gross L. Effects of changing US parenting styles ondental practice: Perceptions of diplomates of the American Board of PediatricDentistry presented to the College of Diplomates of the American Board of PediatricDentistry 16th Annual Session, Atlanta, GA, Saturday, May 26, 2001. Pediatr Dent.2002;24:18–22.
- Berkowitz RJ. Mutans streptococci: acquisition and transmission. Pediatr Dent.2006;28:106–109.
- Tinanoff N, Reisine S. Update on early childhood caries since the SurgeonGeneral’s Report. Acad Pediatr. 2009;9:396–403.
- White HR, Lee JY, Rozier RG. The effect of general anesthesia legislation onoperating room visits by preschool children undergoing dental treatment. PediatrDent. 2008;30:70–75.
- Bohaty B, Spencer P. Trends in dental treatment rendered under generalanesthesia, 1978 to 1990. J Clin Pediatr Dent. 1992;16:222–224.
- Wright GZ, Stigers JI. Nonpharmacologic management of children’s behaviors. In:McDonald and Avery’s Dentistry for the Child and Adolescent, 9th ed. Dean JA, Avery,DR, McDonald RE, eds. Maryland Heights, Mo: Mosby Elsevier; 2011;27–40.
- Dock M. Pharmacologic management of patient behavior. In: McDonald andAvery’s Dentistry for the Child and Adolescent, 9th ed. Dean JA, Avery, DR, McDonaldRE, eds. Maryland Heights, Mo: Mosby Elsevier; 2011;253–276.
- Weddell JA, Jones JE. Hospital dental services for Children and the use of generalanesthesia. In: McDonald and Avery’s Dentistry for the Child and Adolescent, 9th ed.Dean JA, Avery, DR, McDonald RE, eds. Maryland Heights, Mo: Mosby Elsevier;2011:277–295.
- Dionne RA, Yagiela JA, Coté CJ, et al. Balancing efficacy and safety in the use oforal sedation in dental outpatients. J Am Dent Assoc. 2006;137:502–513.
- Fuhrer CT 3rd, Weddell JA, Sanders BJ, Jones JE, Dean JA, Tomlin A. Effect onbehavior of dental treatment rendered under conscious sedation and generalanesthesia in pediatric patients. Pediatr Dent. 2009;31:492–497.
- Enger DJ, Mourino AP. A survey of 200 pediatric dental general anesthesia cases.ASDC J Dent Child. 1985;52:36–41.
- Kanellis MJ, Diamiano PC, Momany ET. Medicaid costs associated with thehospitalization of young children for restorative dental treatment under generalanesthesia. J Public Health Dent. 2000;60:28–32.
- Nagarkar SR, Kumar JV, Moss ME. Early childhood caries-related visits toemergency departments and ambulatory surgery facilities and associated charges inNew York State. J Am Dent Assoc. 2012;143:59–65.
- Rowley ST, Sheller B, Williams BJ, Mancl L. Utilization of a hospital for treatment ofpediatric dental emergencies. Pediatr Dent. 2006;28:10–17.
- Casamassimo PS, Edelstein BE. Beyond the dmft: the human and economic costof early childhood caries. J Am Dent Assoc. 2009;140:650–657.
- Griffin SO, Gooch BF, Beltrán E, Sutherland JN, Barsley R. Dental services, costs, andfactors associated with hospitalization for Medicaid-eligible children, Louisiana 1996-
- J Public Health Dent. 2000;60:21–27.
- Lewis CW, Nowak AJ. Stretching the safety net too far waiting times for dentaltreatment. Pediatr Dent. 2002;24:6–10.
- Brown A, Lowe E, Zimmerman B, Crall J, Foley M, Nehring M. Preventing earlychildhood caries: lessons from the field. Pediatr Dent. 2006;28:553–560.
- American Academy of Pediatric Dentistry. Guidelines on risk-assessment andmanagement for infants, children, and adolescents. Available at:www.aapd.org/media/Policies_Guidelines/G_CariesRiskAssessment.pdf. AccessedSeptember 17, 2012.
From Dimensions of Dental Hygiene. October 2012; 10(10): 34–39.

{kind=link}