 ZINKEVYCH/ISTOCK/GETTY IMAGES PLUS
ZINKEVYCH/ISTOCK/GETTY IMAGES PLUS
Focus on Caries Prevention
Risk assessment and management are key to a caries prevention strategy.
Dental caries is a chronic and multifactorial disease that affects people of all ages throughout the world.1,2 This disease process can progress to a painful and life-threatening condition when left untreated as well as create a financial burden.3 In an effort to place more focus on prevention, dental hygienists can be proactive by performing a caries risk assessment along with providing oral health education and recommendations related to the caries risk level of individual patients.
Considered an infectious and preventable disease, tooth decay affects the hard tissue and progresses from the outer surface of the tooth inward. Dental caries affects the mineral content of the tooth as it goes through stages of demineralization and remineralization. This influence on the demineralization of the tooth surface can range from undetectable mineral loss to severe and clinically visible mineral loss and tooth destruction. As they progress, caries lesions become irreversible, necessitating treatment. What can turn into a painful and destructive disease of the hard tissues begins with early changes that cannot be detected clinically.1,2 Data from the World Health Organization show that untreated dental caries was the most common health condition in 2017, and an estimated 2.3 billion people have decay present on permanent teeth.4
Tooth destruction via dental caries is caused by bacterial by-products in the form of acids that lower the oral pH. These acidic by-products are the result of bacterial fermentation of dietary carbohydrates found in the biofilm coating the tooth and oral surfaces.2 Acidogenic and acidophilic bacteria involved with the caries process include Streptococcus mutans, S. sobrinus, and Lactobacillus.2
Although mineral loss begins with the acid by-products from carbohydrate fermentation, the amount of tooth loss is influenced by physical, biological, environmental, behavioral, and lifestyle-related factors.1,2,5,6 Low socioeconomic status and psychological factors may also influence the disease process.1 Biological factors may include high numbers of cariogenic bacteria, inadequate salivary flow, and insufficient fluoride exposure while behavioral factors may refer to poor oral hygiene and inappropriate feeding habits for infants.2
-
- Treatment protocols based on patient risk levels. Available at: Click here. Accessed January 18, 2022.
-
- American Dental Association. Oral Health Topics. Available at: Click here. Accessed January 18, 2022.
-
- American Dental Association: Council on Scientific Affairs and United States Department of Health and Human Services. Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure. Available at: Click here. Accessed January 18, 2022.
-
- Sharma S, Mishra S, Mittal N. Influence of tobacco dependence on caries development in young male adults: a cross-sectional study. J Conserv Dent. 2018;21:597–601. Copyright Jennifer E. Fehrenbacher, Reviewed by USI faculty 4/ 21.
Risk Factors
Many risk factors are associated with dental caries and they may change over time. A combination of personal, oral, and environmental factors influence patients’ risk levels. Personal risk factors include education, sociodemographic information, income, dental insurance coverage, knowledge, attitudes, oral health literacy, and behaviors such as oral hygiene and snacking habits. Factors affecting the oral environment include fluoride, sealants, chewing gum, plaque pH, microbial species present, sugars, protein, saliva composition and flow rate, and use of antibacterial agents. Additional factors that may contribute to the caries process are time, bacteria in the biofilm, and diet.2 Immunology, special needs, and genetic factors are additional aspects of a risk profile that need to be considered. The strongest predictor of a future decay, however, is the existence of current caries.5
A Shift from Reactive to Proactive
While restorative therapy once was the standard of care, over the past three decades, a more preventive approach has become preferred. Restorations are a way to treat tooth decay; however, they can be expensive and they require maintenance. Minimally invasive dentistry—including increased oral hygiene for the removal of biofilm and the use of fluoride and sealants—is now the recommended approach. Both dentists and dental hygienists should base treatment decisions on each patient’s individual risk factors while focusing on disease control and prevention.2
Dental hygienists play an important role in the prevention of dental caries. Due to their education and their one-on-one contact with patients, dental hygienists are well positioned to provide risk assessment, education, oral disease prevention, and evidence-based disease management.7 Along with the dental team, dental hygienists can assist in caries management plans that are unique to each patient’s needs. A knowledge of the recommended guidelines for caries management, such as fluoride use and dental sealant application, is needed to make appropriate recommendations.8
Caries Risk Assessment
As a part of a focus on prevention, a caries risk assessment should be performed to determine patients’ individual risk factors.5 Several caries risk assessment forms are available to help clinicians asses both protective and risk factors in order to assign a risk level. Risk levels include low, moderate, high, and extreme (high risk with hyposalivation).9 Assessing risk level helps to represent the likelihood of future caries development and assists the decision-making process concerning the treatment, control, and prevention of caries lesions.
Caries management by risk assessment (CAMBRA) is an evidence-based approach to caries risk assessment that can be performed in dental offices.5,9 Caries risk assessment is used to assess patient risk in order to provide appropriate treatment and recommendations.10 CAMBRA provides a checklist that includes a series of patient questions that oral health professionals use to determine patients’ caries risk levels. Treatment options—both preventive and restorative—are recommended based on an individual’s assessed risk level.11 Caries risk assessment is strongly recommended for every patient in dental hygiene practices. Dental hygienists can play an important role in completing these assessments and recommending preventive and management strategies for patients.8
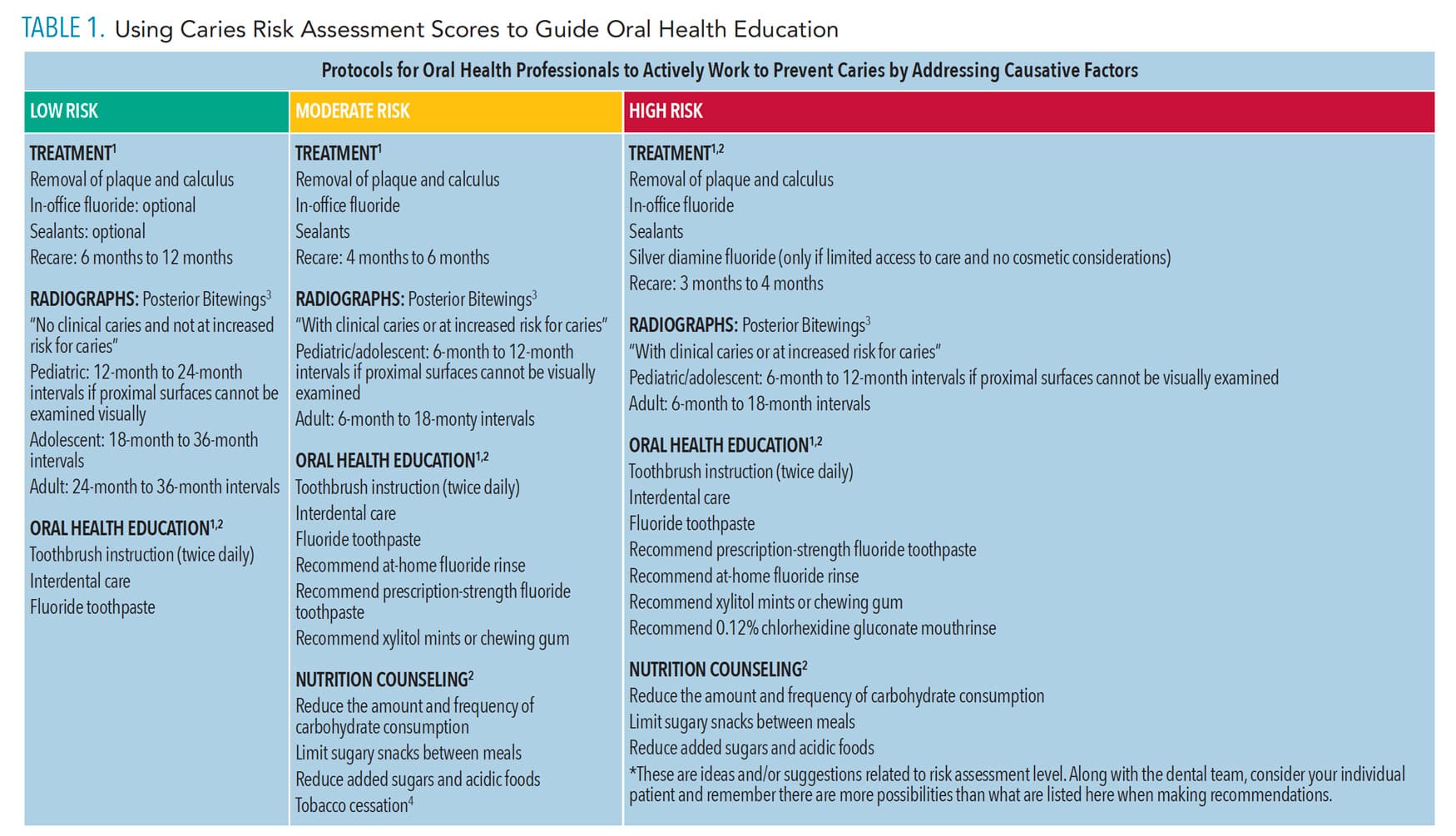
In order to help dental hygiene students at the University of Southern Indiana Dental Clinic connect the implementation of the American Dental Association (ADA) Caries Risk Assessment form to oral health education, a flow chart was created (Table 1, page 27). The chart will appear as a laminated visual in units with a copy of the ADA Caries Risk Assessment form on one side and the flow chart on the other. Students will use a dry erase marker to determine caries risk level and the flow chart to make corresponding suggestions regarding care.
Oral Health Habits
Poor oral hygiene habits leave bacterial biofilm on the tooth surfaces, raising caries risk.2 As this biofilm harbors the pathogenic bacteria that produce acid by-products, thorough biofilm removal is key. Patients should be instructed to brush their teeth two times daily with a fluoride toothpaste, drink fluoridated water, and encourage professional fluoride applications and or the use of at-home fluoride rinses when warranted by risk level.5,10 Daily interdental cleaning, such as flossing, should also be encouraged.10 Products, such as xylitol chewing gum, can also be recommended to increase saliva and potentially promote remineralization.5
Nutrition
Because the caries process is influenced by fermentable carbohydrates and their role in bacterial acid production, nutritional counseling should be an additional aspect of patient education based on caries risk.10 Frequent consumption of refined carbohydrates, such as sugary snacks and drinks, provides a medium for bacteria to metabolize—leading to production of acidic by-products, which, ultimately, results in mineral loss.2,5 Oral health professionals can advise patients to reduce the amount and frequency of fermentable carbohydrate consumption, an important part of the caries management plan for patients with high caries risk.10
Additional Interventions
Possible therapeutic interventions based on patient risk include increased frequency of radiographic assessment, use of chemotherapeutic agents such as 0.12% chlorhexidine gluconate mouthrinse, application of pit and fissure sealants, and use of prescription fluoride toothpaste and mouthrinses.
The ADA Council on Scientific Affairs and the Center for Evidence-Based Dentistry issued new evidence-based guidelines on nonrestorative treatments for caries in 2018. They recommend the use of 38% silver diamine fluoride, sealants, 5% sodium fluoride varnish, 1.23% acidulated phosphate fluoride gel, and 5,000 ppm fluoride toothpaste or gel.12
In addition to in-office treatment for plaque and calculus removal, the length between recare appointments can vary from 3 months to 6 months depending on risk level.13 Radiograph intervals also vary according to age and caries risk level, with a range of posterior bitewings every 6 months to 18 months for high-risk adults and every 24 to 36 months for low-risk adults.14
Patient motivation and adherence are integral to the success of caries management.10 Motivational interviewing—a patient-centered technique—can be used by dental hygienists to help guide management plans that are individualized and take patient preferences into account.
Conclusion
While many factors contribute to dental caries, addressing the patient’s risk level and providing oral health education and recommendations based on that risk level equate to a preventive management approach. Understanding risk factors and possible interventions as they relate to caries risk level is an important aspect of care provided by dental hygienists that will help to relieve the burden caused by tooth decay.
References
- Charland R, Voyer R, Cudzinowski L, Salvail P, Abelardo L. Dental caries: diagnosis and treatment. N Y State Dent J. 2002;68:38–40.
- Selwitz RH, Ismail AI, Pitts NB. Dental caries. The Lancet. 2007;369:51–59.
- Fleming E, Afful J. Prevalence of total and untreated dental caries among youth: United States, 2015-2016. NCHS Data Brief. 2018;307:1-8.
- World Health Organization. Oral Health. Available at: who.int/news-room/fact-sheets/detail/oral-health. Accessed January 19, 2022.
- Ding-Yu Y, Hsiao-Ching K, Yi-Hsin Y, Pei-Shan H. The responsiveness of patients’ quality of life to dental caries treatment—a prospective study. PLoS One. 2016;11:10.
- Young DA, Nový BB, Zeller GG, Hale R, Hart T, Truelove EL. The American Dental Association caries classification system for clinical practice: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2015;146:79.
- Langelier M, Continelli T, Moore J, Baker B, Surdu S. Expanded scopes of practice for dental hygienists associated with improved oral health outcomes for adults. Health Aff. 2016;35:2207–2215.
- Clovis J, Horowitz A, Kleinman DV, Wang MQ, Massey M. Maryland dental hygienists’ knowledge, opinions and practices regarding dental caries prevention and early detection. J Dent Hyg. 2012;86:292–305.
- Featherstone JDB, Chaffee BW. The evidence for Caries Management by Risk Assessment (CAMBRA®). Adv Dent Res. 2018;29:9–14.
- Maheswari S, Raja J, Kumar A, Seelan R. Caries management by risk assessment: A review on current strategies for caries prevention and management. J Pharm Bioallied Sci. 2015;7:320–324.
- Urban R, Rowe DJ. Knowledge, attitudes and practice of dental hygienists regarding caries management by risk assessment. J Dent Hyg. 2015;89:55–62.
- Slayton RL, Urquhart O, Araujo MWB, et al. Evidence-based clinical practice guideline on nonrestorative treatments for carious lesions: A report from the American Dental Association. J Am Dent Assoc. 2018;149:837–849.
- Treatment Protocols Based on Patient Risk Levels. Available at: multimedia.3m.com/mws/media/591994O/treatment-protocols-based-on-patient-risk-assessment.pdf. Accessed January 18, 2022.
- American Dental Association Council on Scientific Affairs and United States Department of Health and Human Services. Dental Radiographic Examinations: Recommendations for Patient Selection and Limiting Radiation Exposure. Available at: ada.org/~/media/ADA/Publications/ADA%20News/Files/Dental_Radiographic_Examinations_2012.pdf?la=en. Accessed January 18 2022.
From Dimensions of Dental Hygiene. February 2022;20(2):26-28.

{kind=link}