
Floss Alternatives
As an adjunct to floss, interdental cleaning devices can help patients begin a regimen of interproximal biofilm removal.
“Are you flossing daily?” Patients hear this question each time they visit their dental hygienist. Unfortunately, only one or two patients out of 10 say yes. Studies show that 10% to 21% of the American population practices daily flossing.1,2 As dental health care professionals, we know that one of the biggest benefits of interproximal plaque removal is the reduction of dental caries and gingival and periodontal diseases.3-6 In my opinion, the newer research demonstrating a correlation between periodontal infections and systemic diseases7 and that bacteria can be transmitted to infants from caregivers (especially mothers)8 may be the most effective in motivating patients.
In motivated patients who have normal probe readings, good dexterity, and embrasures where the papilla fills the interproximal space and the teeth are in contact, dental floss is the most effective tool for removing biofilm from the proximal surfaces.9 Patients with moderate to severe periodontal diseases often have recession that results in larger embrasure areas with little or no interproximal papilla and exposed concave root surfaces. These areas often cannot be thoroughly cleaned with dental floss. Patients with restorations may also require alternatives to floss due to their inability to properly maneuver the floss and/or lack of patience. Because of the benefit of interdental biofilm removal and the lack of patient compliance with daily flossing, alternative methods to flossing are important. 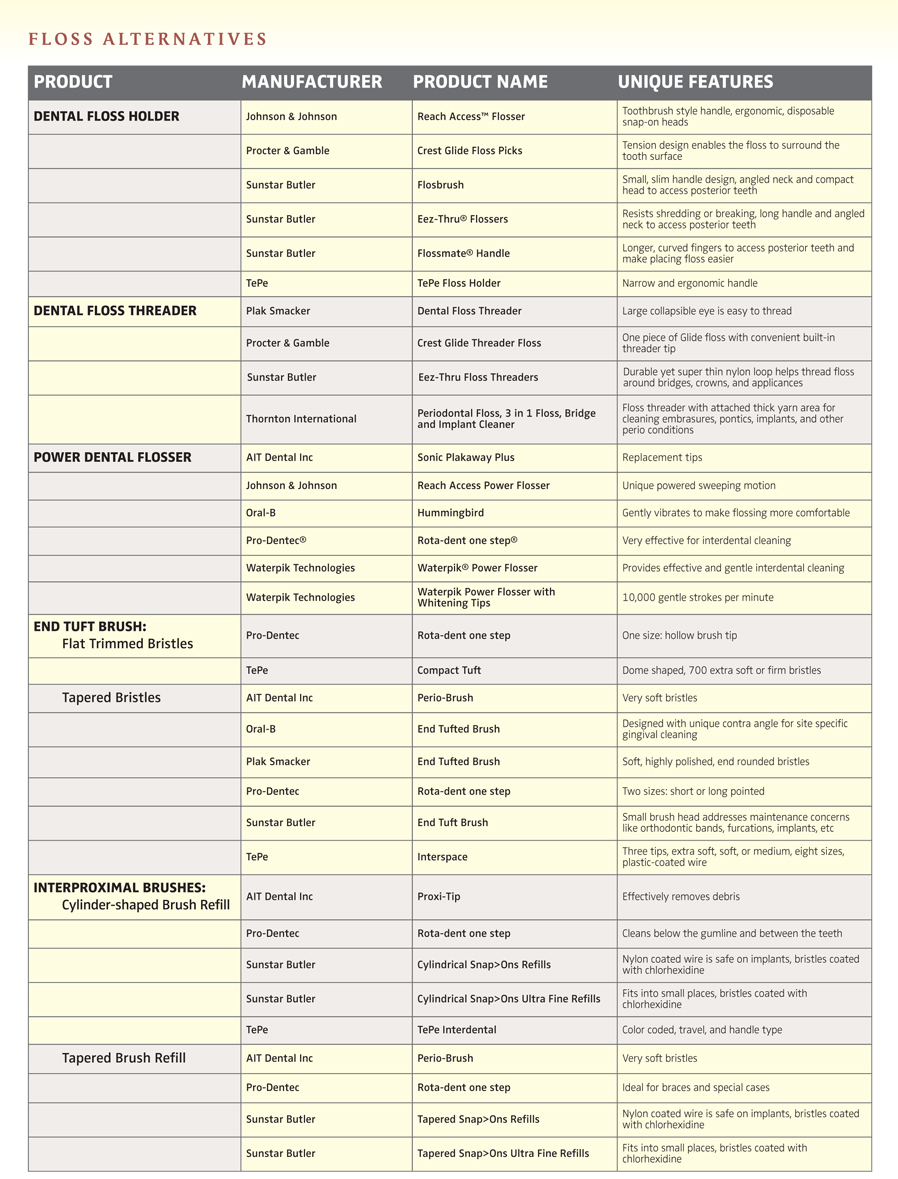
In reviewing the literature on interdental cleaning, few research studies and science-based information exist. Several short-term studies supporting the effectiveness of the different interdental cleaning devices have been done but more long-term studies are needed.9
In determining which alternative method is most appropriate for patients, the following criteria should be used: the patient’s periodontal condition (including anatomical challenges of the root surfaces and type of interdental embrasures), restorative work, age, motivation, and manual dexterity. All methods of interdental cleaning should be done one or two times per day with emphasis on the evening. Patients should use the interdental devices before toothbrushing. When biofilm is removed from the proximal surfaces first, the fluoride in toothpaste may reach the proximal surfaces, helping prevent dental caries.10 Using interdental devices before toothbrushing can also result in more efficient plaque removal because people are usually more meticulous about any task in the beginning. Lastly, they may not be as motivated to perform interdental cleaning after brushing because the mouth feels clean with brushing alone.
Interdental Brushes
Interdental brushes are the most common alternatives to dental floss9 and can be very effective in bacterial plaque removal and in reducing gingival inflammation in embrasures with little or no interproximal papilla or in exposed furcation areas.11-15 In general, interdental brushes have nylon fibers attached to a wire that is then mounted on various types of plastic handles. The two basic shapes include conical and tapered. Each shape has varying sizes that range from very small to large. The majority of brushes are coated with nylon or plastic and these are safe to use with implants. Some brushes are treated with an antimicrobial agent. The newest interproximal brush has a plastic cylinder tube that can be filled with a therapeutic agent of choice. Brush sticks are the smallest interproximal brush. They have a plastic handle and two cleaning ends: one with a scored triangular-shaped tip and the other with a flexible stem with three rows of lateral bristles.
The interdental brush is indicated for periodontally involved patients with wider embrasure areas and/or recession with root surfaces exposed; restorative areas, such as bridges, crowns, and implants; and patients wearing orthodontic appliances with wide embrasure areas. In addition to removing biofilm, the brush can be used to apply different therapeutic agents. These brushes are contraindicated for patients with papilla that fills the interproximal space or for patients who do not have adequate dexterity or control, ie, someone with arthritis or tremors. Anecdotally, I would wait 1 to 2 weeks before using the interdental brush with a patient who has just had periodontal pocket reduction surgery. Introducing the brush too early may traumatize the site and delay healing.
The interdental brush is used by placing it at a 90° angle at the gingival margin in the open embrasure area (Figure 1, page 22). The brush is moved back and forth from the buccal to lingual and then lingual to buccal using a short stroke. With my patients, I have found that using five strokes per surface is usually efficient. Patients must practice and receive instruction on how to avoid trauma. Trauma usually results from the patient being too aggressive, going too fast, or trying to force the brush in an area that is too small.
The diameter of a brush should be slightly larger than the gingival embrasures of the area to be cleaned. This allows effective biofilm removal from both the mesial and distal surfaces. If the embrasure is larger than the brush, each proximal surface must be cleaned separately. In addition to the size of the brush, how the handle and refill brushes are attached is important. There are two styles of handles—the long handle with replaceable brush refills and the shorter handles that usually have permanently attached brushes. Patients with larger hands may find it easier to use a longer handle for better control. Patients who have difficulty with fine motor tasks will prefer brushes that are already attached. 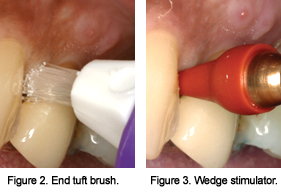
The brush refills should be changed according to the frequency of use, the number of areas it is used in, and the amount of pressure applied when using the brush. For example, if the brush is used two times per day for molars only, using slight to moderate pressure, the brush should be changed every 1 to 2 weeks. If a brush is used in only one area, one time a day, the brush could be changed every 1 to 2 months.
End Tuft Brushes
Single tuft or end tuft brushes are small brushes with nylon bristles that are attached to a plastic handle. There are variations in the shape of the tufts and the width and length of the handles. Single tuft brushes are indicated in open embrasure areas where there is little or no papilla. They are used by first placing the brush in the interdental area (Figure 2). The patient should then jiggle the brush in a small circular motion and/or use a sweeping motion away from the gingiva. The single tuft brush is for patients who prefer a longer handle and are not able to change the refills of the interproximal brush or patients who cannot control the interproximal brush due to manual dexterity or disabilities.
Sticks and Picks
Wooden and plastic sticks or wedge stimulators reduce bleeding and inflammation when used to reduce plaque.16 These devices are made of balsa, bass, birch, or linden wood or plastic. Some of the wood sticks are treated with xylitol. Wood sticks are triangular in shape and come in varying sizes. Plastic sticks are smaller in size and have varying shapes. Both the wood and plastic are used only in areas that do not have gingiva filling the interproximal space. They are inserted in the interproximal space with the flat surface, the base of the triangle, resting on the gingival margin. The stick is moved in and out from buccal to lingual using short strokes. Wood sticks should be discarded if they splinter.
One of the most commonly used tools, toothpicks differ from the wooden triangular sticks in their shape and size and may not be as effective in plaque removal in open embrasures.15 A toothpick can be manipulated by hand, but a holder will usually increase a patient’s effectiveness in control and accessibility to posterior areas. The toothpick is placed at a 90° angle in the interproximal area and moved in and out from buccal to lingual. It can also be rubbed on each proximal surface using a gentle up and down motion.
Tip Stimulators
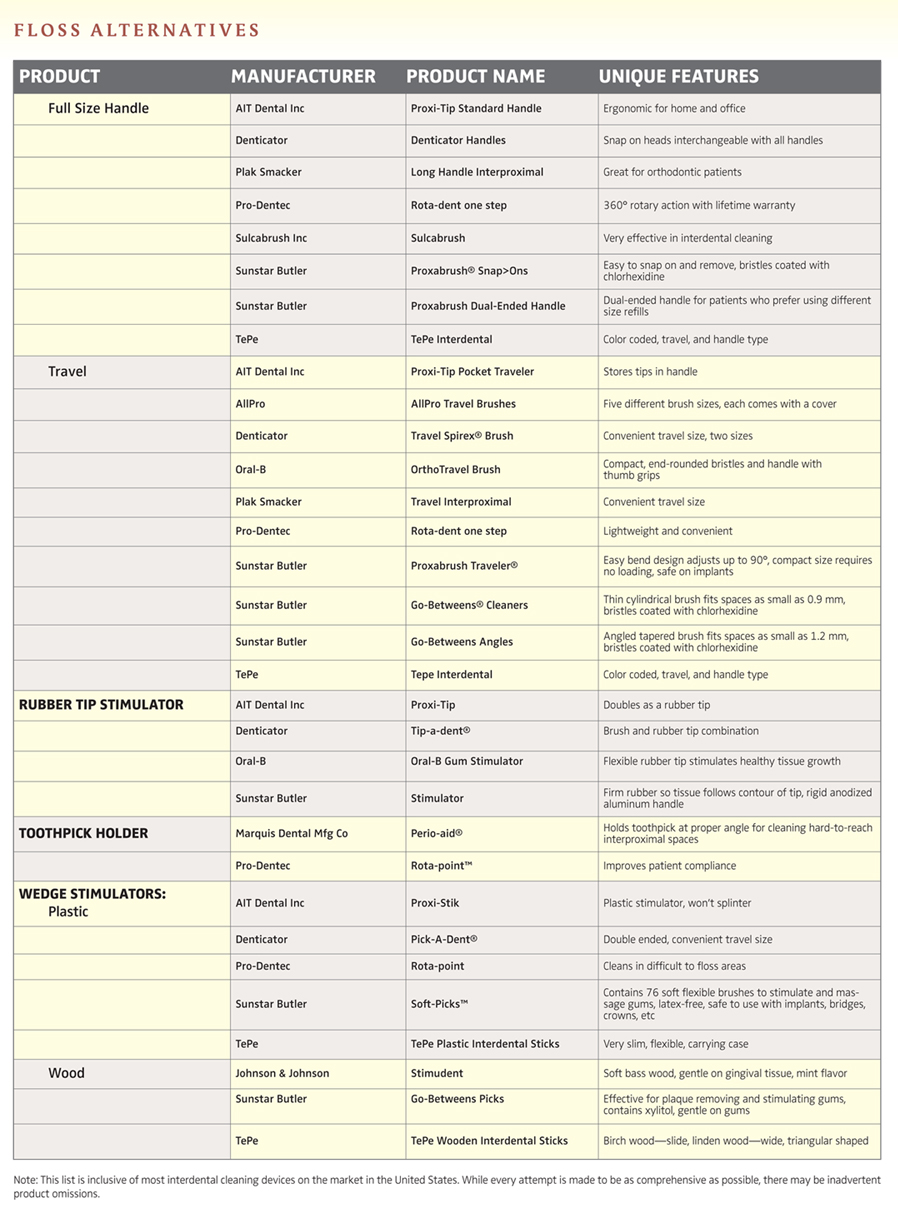
Rubber or plastic tips are recommended for gingival stimulation and for plaque removal in open embrasures. When using these devices for plaque removal, the tip is placed at a 90° angle in the interdental area next to the gingival margin (Figure 3). The tip is then moved with a sweeping motion from the gingival margin toward the incisal edges or moved from buccal to lingual using short back and forth strokes. Patients should be careful not to traumatize the tissue with the tip.
Power assisted interproximal cleaning devices have been developed to improve compliance. These devices include a variety of interdental brush heads that attach to the handle of a power assisted brush, interdental cleaners that are a triangular plastic attachment for a power assisted toothbrush handle, or a nylon filament tip with an automated handle. Automated interproximal devices have been shown to reduce plaque, but the research is very limited.3, 17 Some of the interproximal attachments can be purchased coated with a whitening agent. All of these devices are used by placing the brush or tip at a 90° angle into the interproximal area and holding it in place for 5 to 10 seconds.
Additional research is needed to help practitioners make an evidence-based decision when recommending interproximal plaque removing devices. As professionals, we have a responsibility to educate our patients regarding the importance of interdental cleaning, to help the patient select the most appropriate tool(s), to educate the patient on effective technique, and to continually evaluate the patient’s compliance and make modifications when necessary.
References
- Macgregor ID, Regis D, Balding J. Self-concept and dental health behaviours in adolescents. J Clin Periodontol. 1997;24:335-339.
- Rimondini L, Zolfanelli B, Bernardi F, Bez C. Self-preventive oral behavior in an Italian university student population. J Clin Periodontol. 2001;28:207-211.
- Kinane DF. The role of interdental cleaning in effective plaque control: Need for interdental cleaning in primary and secondary prevention. In: Lang NP, Loe H, Armstrong R. Proceedings of the European Workshop on Mechanical Plaque Control. Berlin: Quintessence. 1998;156-168.
- Loe H. Oral hygiene in the prevention of caries and periodontal disease. Int Dent J. 2000;50:129-139.
- Graves RC, Disney JA, Stamm JW. Comparative effectiveness of flossing and brushing in reducing interproximal bleeding. J Periodontol. 1989; 60:243-247.
- Wright GZ, Banting DW, Feasby WH. The Dorchester dental flossing study: final report. Clin Prev Dent. 1979;1:23-26.
- Fowler EB, Breault LG, Cuenin MF. Periodontal disease and its associations with systemic disease. Mil Med. 2001;166:85-89.
- Asikainen S, Chen C, Alaluusua S, Slots J. Can one acquire periodontal bacteria and periodontitis from a family member? J Am Dent Assoc. 1997;128:1263-1271.
- Consensus Report: Discussion, Section II. Proceedings of the World Workshop on Clinical Periodontics. Chicago, American Academy of Periodontology. 1989;13-17.
- Wilkins EM. Clinical Practice of the Dental Hygienist. Baltimore: Lippincott Williams & Wilkins, 2005.
- Smith BA, Armstrong CS, Morrison EC, Caffesse RG . Efectiveness of four interproximal cleaning devices in plaque removal and gingival health. Am J Dent. 1988;1:57.
- Smukler H, Nager MC, Tolmie PC. Interproximal tooth morphology and their effect on plaque removal. Quintessence Int. 1989;20:249.
- Walsh, MM, Heckman BH, Moreau-Diettinger R. Use of gingival bleeding for reinforcement of oral home care behavior. Community Dental Oral Epidemiol. 1985 13:133.
- Kiger RD, Nylund K, Feller RP. A comparison of proximal plaque removal using floss and interdental brushes. J Clin Periodontol. 1991;18:681-684.
- Christou V, Timmerman MF, Van der Velden U, Van der Weijden FA. Comparison of different approaches of interdental oral hygiene: interdental brushes versus dental floss. .J Periodontol. 1998;69:759.
- Lewis MW, Holder-Ballard C, Selders RJ Jr, Scarbecz M, Johnson HG, Turner EW. Comparison of the use of a toothpick holder to dental floss in improvement of gingival health in humans. J Periodontol. 2004;75:551-556.
- Sicilia A, Arregui I, Gallego M, Cabezas B, Cuesta S. Home oral hygiene revisted. Options and evidence. Oral Health Prev Dent. 2003;1:407-422.
From Dimensions of Dental Hygiene. October 2005;3(10):22, 24, 26.

{kind=link}