
Expanding Your Instrument Armamentarium
The use of extended shank, area-specific instruments in nonsurgical periodontal therapy.
 The newly designed extended shank, area-specific instruments may play a role in providing efficacious nonsurgical periodontal therapy as they are designed to effectively instrument complex root anatomy. In general, area-specific curets are de signed to adapt to specific tooth surfaces and areas of the mouth. Most instrument companies offer a full array of area-specific Gracey curets numbered 1 through 18. The 1/2 design with a straight shank adapts to an terior teeth, and the higher numbers with curved, complex shanks (ie, 11/12, 13/14, etc) are designated for posterior areas.
The newly designed extended shank, area-specific instruments may play a role in providing efficacious nonsurgical periodontal therapy as they are designed to effectively instrument complex root anatomy. In general, area-specific curets are de signed to adapt to specific tooth surfaces and areas of the mouth. Most instrument companies offer a full array of area-specific Gracey curets numbered 1 through 18. The 1/2 design with a straight shank adapts to an terior teeth, and the higher numbers with curved, complex shanks (ie, 11/12, 13/14, etc) are designated for posterior areas.
Standard area-specific designs were initially developed to extend deep into subgingival areas to remove calculus. In these designs, the one cutting edge that adapts to the tooth surface is angled 20% lower than the other nonworking side in relation to the shank. Extended shank area-specific instruments have these same features as well as additional ones to enhance their adaptability.
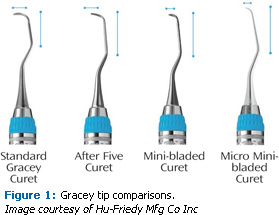
The potential benefits to instrumenting with extended shank area-specific curets are attributable to the unique instrument design that includes a longer terminal shank, a thinner blade, and a reduction in blade length (on some instruments). There are three categories of this type of curet: extended shank curets, mini-bladed curets, and the new micro mini-bladed curet (Figure 1).
The main difference among these instruments is that the terminal shank is 3 mm longer than the standard area-specific design to negotiate periodontal pockets 5 mm or greater. The blade is also thinner, facilitating ease of insertion and reduced tissue distention. This type of instrument is ideal for pocket areas deeper than 5 mm, especially those located on proximal surfaces. Extended shank area-specific designs are available with a standard flexible shank for fine calculus deposits and finishing of root surfaces, or with a rigid shank indicated for tenacious or residual deposits. Table 1 provides a comparison of extended, mini-bladed, and micro mini-bladed designs with standard area-specific designs.
What the Research Says
Nagy and others evaluated the effectiveness of subgingival scaling and root planing with rigid longer shank Gracey curets and rigid standard Gracey curets; 140 maxillary and mandibular incisors, canines, and premolars were evaluated.2 Using stereomicroscopic evaluation of the root surface, no statistically significant difference in effect between the two curets was found. The mesial root surfaces had less calculus remaining (27%) than the other root surfaces (44%). Distal surfaces had the most calculus remaining. The majority of remaining calculus was located in root flutes, below cementoenamel junctions, and on root surface line angles.3,4 Mean curet efficiency subgingivally ranged from 1 mm to 3.46 mm depending on the root surface and not on the curet used. Limitations of this study included the presence of tenacious calculus, limited operators, ultrasonic instrumentation not being employed, lack of fiberoptic illumination, and single versus multiple appointments. Further study comparing standard and extended shank curets is warranted.
The mini-bladed area-specific curets also have a 3 mm longer shank, which is indicated for 5 mm or deeper pockets. The added feature of this instrument is a 50% reduction in blade length compared to extended shank or standard area-specific designs. For this reason, mini-bladed curets adapt to narrow facial and lingual surfaces of anterior teeth, furcations, and root surfaces in narrow and deep periodontal pockets. In some instances, they might not be as useful for the midline of proximal surfaces due to the short blade, although they may be used adjacent to line angles, particularly in a deep pocket.
The newest extended shank design—the micro mini-bladed curet—has additional design features. The blade is 20% thinner than a mini-bladed area-specific curet to enhance subgingival extension and reduce tissue distention. The shank rigidity is slightly increased, which may reduce the need for lateral pressure during calculus removal, possibly resulting in less fatigue for the clinician. Also, heavier calculus and tenacious deposits might be removed with greater ease than the standard shank diameter, thus the micro-mini may be useful during initial therapy as well as in periodontal maintenance therapy.
 Extended shank, mini-bladed, and micro mini-bladed curets are manufactured in various instrument designs that correspond to the standard designs for anterior and posterior teeth. For example, a hygienist might select a 1/2, 5/6, 11/12, and 13/14 in both the extended shank and mini-bladed designs. This would be appropriate in generalized deep pockets where a longer blade and a short blade are indicated for various surfaces, furcations, and concavities. The micro mini, however, is currently only manufactured in the 1/2, 7/8, 11/12, and 13/14 designs.
Extended shank, mini-bladed, and micro mini-bladed curets are manufactured in various instrument designs that correspond to the standard designs for anterior and posterior teeth. For example, a hygienist might select a 1/2, 5/6, 11/12, and 13/14 in both the extended shank and mini-bladed designs. This would be appropriate in generalized deep pockets where a longer blade and a short blade are indicated for various surfaces, furcations, and concavities. The micro mini, however, is currently only manufactured in the 1/2, 7/8, 11/12, and 13/14 designs.
Technique Highlights
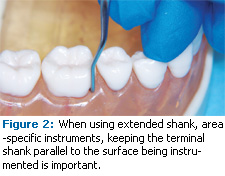
Technique strategies for effective adaptation and activation of these instruments are similar to those for standard area-specific curets. Some basic highlights include ensuring that the blade extends apical to the calculus deposit in a deep pocket and having the terminal shank parallel to the surface being instrumented (Figure 2).
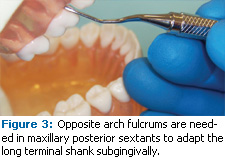
The use of periodontal pocket probe readings is valuable in assessing if extension is reaching the most apical regions of the pocket. Opposite arch fulcrums are needed in maxillary posterior sextants to adapt the long terminal shank subgingivally (Figure 3). In this case, the clinician places the hand further up on the instrument handle to establish the fulcrum on the mandibular teeth. Extraoral fulcrums may be used to accomplish this needed extension into deep pockets. Extended shank instruments are useful after ultrasonic debridement with a subgingival insert to finish the surface. Additionally, using these instruments in periodontal maintenance therapy is recommended because the thinner blade can be inserted subgingivally when tight nonelastic gingival tissue is present.
 Another indication for mini-bladed curets is on direct lingual and facial surfaces of teeth, particularly anterior teeth, because of the shorter blade. A toe-down approach can be used in shallower pockets where the gingiva permits access due to inflammation. Again, the thinner blade enhances access subgingivally and the shorter blade helps prevent unintentional trauma to the epithelial attachment.
Another indication for mini-bladed curets is on direct lingual and facial surfaces of teeth, particularly anterior teeth, because of the shorter blade. A toe-down approach can be used in shallower pockets where the gingiva permits access due to inflammation. Again, the thinner blade enhances access subgingivally and the shorter blade helps prevent unintentional trauma to the epithelial attachment.
Alves et al5 studied the immediate effect of trauma from instrumentation after scaling and root planing with different instruments. The study looked at 10 subjects with moderate chronic periodontitis and probe depths ranging from 3.5 mm to 6.5 mm on anterior teeth. The anterior teeth were scaled and planed with Gracey mini-bladed curets (Mini-Five), and standard Gracey curets. The study found that root instrumentation caused an average trauma from instrumentation of 0.76 mm as measured by relative attachment level post-treatment. Also, they found no differences between the tested instruments (Gracey mini-bladed and Gracey standard curets) when evaluating trauma from instrumentation post-scaling and root planing. Although not specifically stated, instrumentation would have included a variety of strokes, therefore, the toe down approach would not have been evaluated alone in this study.
Perhaps it is the meticulous nature of scaling and root planing that affects the outcome of periodontal therapy rather than the choice of curets or method of instrumentation used. Certainly the experience and skill of the clinician affect the ultimate outcome as well. More research is needed to evaluate the effects of various instrument designs on thorough and fastidious instrumentation.
References
- American Academy of Periodontology. Treatment of Plaque-Induced Gingivitis, Chronic Periodontitis, and other Clinical Conditions. Chicago: Research, Science and Therapy Committee, American Academy of Periodontology. J Periodontol. 2001;72:1790-1800.
- Nagy RJ, Otomo-Corgel J, Stambaugh R. The effectiveness of scaling and root planing with curets designed for deep pockets. J Periodontol. 1992;63:954-959.
- Brayer WK, Mellonig JT, Dunlap RM, Marinak KW, Carson RE. Scaling and root planing effectiveness: the effect of root surface access and operator experience. J Periodontol. 1989;60:67-72.
- Fleischer HC, Mellonig JT, Brayer WK, Gray JL, Barnett JD. Scaling and root planing efficacy in multirooted teeth. J Periodontol. 1989;60:402-409.
- Alves RV, Machion L, Casati MZ, Nociti Júnior FH, Sallum AW, Sallum EA. Attachment loss after scaling and root planing with different instruments. A clinical study. J Clin Periodontol. 2004;31:12-15.
From Dimensions of Dental Hygiene. May 2009; 7(5): 31-33.

{kind=link}