 SAM EDWARDS / OJO IMAGES / GETTY IMAGES PLUS
SAM EDWARDS / OJO IMAGES / GETTY IMAGES PLUS
Ergonomic Equipment Considerations for the Dental Hygienist
Making informed decisions about the use of loupes, seating alternatives, and instrument selection in order to improve ergonomics is key to career longevity.
Dental hygienists are commonly affected by musculoskeletal disorders (MSDs) due to repetitive motions and awkward, static postures sustained during clinical practice.1,2 Previous studies indicate 64% to 93% of dental hygienists have musculoskeletal pain or MSDs in the neck, back, shoulders, and wrists.3–5 Additionally, research indicates MSDs may occur in student populations before their careers even begin.6,7 Because of the high rate of MSDs and biomechanical risk factors dental hygienists experience, maintaining proper ergonomics is important to decrease the risk for work-related injuries and increase career longevity.
Ergonomics is the science of workplace design and job demands to increase efficiency and safety.8,9 Ergonomics focuses on the nature of the work, armamentarium used, and the work environment. For dentistry and dental hygiene, this may include designing tools, equipment, work areas, and tasks to, ultimately, fit the nature of clinical practice to the clinician.9 When applied, dental ergonomics may reduce the prevalence of MSDs in oral health professionals.9,10 Research has examined equipment and practices and their effects on ergonomics.11–17 The following information may guide dental hygienists in making informed decisions about armamentarium choices and techniques to improve workplace safety. This may decrease their risk for MSDs and increase their knowledge of ergonomic practices and choices while providing dental hygiene care.
Ergonomic Considerations for Loupes
Adopting an ergonomically sound approach may reduce MSDs. Maintaining an upright sitting position with a neutral neck and trunk is recommended.18,19 Loupes are often introduced in preclinical dental hygiene education and are promoted as an aid to neutral positioning.7,11,12 The most popular type of loupes is through-the-lens (TTL) option in which the magnification ocular is mounted directly into the lens of the frame. Front-lens-mounted loupes have the oculars mounted to the frame rather than into the lens and are sometimes adjustable.
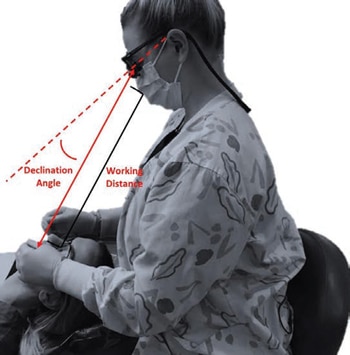
Regardless of type, clinicians must be measured and fitted for the correct working distance, depth of field, and declination angle (downward vertical angle of the optical lens). Customized measures for proper fit will prevent forward tilting of the head and neck and compromised postures.20,21 The working distance and declination angle are important in determining how much neck flexion is needed to view the oral cavity.21 Ideally, the declination angle should be steep enough to allow the dental hygienist to look downward while working without excessive forward flexion of the neck or eye strain (Figure 1).
Research conducted by my colleagues and I found decreased trunk flexion while scaling when dental hygienists wore custom-fitted declination angle loupes compared to standard TTL loupes with a preset declination angle.13 Another study found decreased head tilt angles while wearing vertically adjustable, front-lens-mounted loupes with a declination angle of 40° to 45° compared to TTL loupes.22 Loupes properly measured for declination angle and custom fit in order to help clinicians maintain a neutral posture may decrease poor ergonomics that lead to MSDs.
Some manufacturers are now offering loupes in which the ocular is positioned to allow clinicians to look forward without tilting their heads and necks downward to view the working area. While more research is needed, loupes of this type may allow dental hygienists to sit upright, adopt a neutral position, and reduce muscle strain on the neck. Overall, dental hygienists should consider loupes with adjustable vertical declination angle or those with steeper declination angles to maintain a neutral position for improved ergonomics.
Ocular Types and Magnification Considerations
The magnification power of loupes may offer ergonomic benefit, as it affects the working distance and field of view (area/teeth and structures that can be viewed with clarity).20,23,24 Loupes are generally classified into Galilean and Keplerian (prismatic). Galilean loupes use two lenses—one convex and one concave—and generally provide magnification between 2.0x and 3.5x. Keplerian loupes have two or more convex lenses with a prism offering higher magnification from 3.5x to 8x.
With the increase in magnification, the field of view is diminished, but the possibility of a longer working distance is provided.23,25 Many loupes manufacturers commonly offer 2.5x to 3.5x magnification for dental hygiene loupes; some even offer oculars with adjustable magnification. Studies have found improved posture and increased visual acuity with the use of 2.5x, 3.5x, and 4.0x magnification strengths with both Galilean and Keplerian oculars.26,27
Generally, Galilean loupes are lightweight and suitable for a wide range of tasks.25 Keplerian loupes may be heavier because the telescopes are generally longer, which could potentially compromise neck and trunk posture. Additionally, Keplerian loupes may offer increased visual acuity for all ages because of the increased magnification but may be indicated for more intricate procedures such as endodontic work.26,28
Dental hygienists should explore varying magnification strengths in a working position to find the best field of view and working distance to avoid compromising posture. The weight of different oculars on the frame or in the lens should also be considered as this may result in more forward tilting or muscle strain on the neck.
Lighting in Combination with Loupes
Insufficient lighting while performing dental hygiene tasks may lead to eye fatigue, unnecessary postural demands, and compromised performance.3,29 Coaxial illumination (headlight) is often used with loupes and, while subjective, may help dental hygienists maintain a neutral posture.23,30 Headlights are typically mounted directly to the frame of the loupes and align with the working area to provide a shadow-free environment and eliminate the need to adjust the overhead light.23
Most headlights use light-emitting diode (LED) technology and can be corded or cordless. Studies related to perceptions of LED headlights in combination with loupes cite increased ergonomics, accuracy, and efficiency as advantages.31,32 When choosing headlights to improve ergonomics, dental hygienists should examine the beam uniformity, brightness, color, and the detail they are able to see while in a working position to receive the best ergonomic benefit.21 Additionally, when using a corded or cordless headlight, examine the weight of the light while mounted to the frame and if there is drag from a cord, as these could potentially lead to a compromised neck and trunk position.
Alternative Seating Approaches to Improve Ergonomics
Prolonged seated hygiene work and assuming awkward postures while seated may also contribute to MSDs, particularly in the upper and lower back.33 Sitting in an upright position, with the spine in a natural “s” position with minimal forward flexion (< 20˚) reduces torque on the spine with gravity acting downward.18,19 Lumbar lordosis (sitting upright while keeping the natural curvature of the lumbar spine) decreases spine pressure and ligament tension, and may reduce back pain.34,35 Ergonomic chairs or saddle stools, especially when used with loupes and headlights, may facilitate a more balanced posture and alleviate poor postures.36
Conventional dental operatory chairs have a flat seat while ergonomic chairs or stools place the hips higher than the knees and the seat portion is tilted downward to open the hip angle and decrease pressure on the spine.37 Ergonomic chair designs may have back support and/or arm rests, and ergonomic stools typically resemble a saddle. Some studies have found improved posture with saddle stools and ergonomic chairs while performing dental-related tasks compared to conventional chairs.14,36,38 Additionally, when used in combination with loupes, saddle stools may offer improved posture compared to traditional chairs without loupes.36
Postural variance throughout the workday may help reduce MSDs. Alternating between seated and standing positions may reduce time spent in static postures and may offer more variability for the muscles and joints. In various settings and jobs where seated postures are used, studies have examined postural variance (alternating seated and standing work) throughout the workday and have reported reduced musculoskeletal pain, reduced fatigue, and deceased spinal disorders.39,40
Dental hygienists may see similar benefits when alternating seated and standing dentistry for sound ergonomic postures while working. A pilot study on dental hygiene students alternating seated and standing postures during dental hygiene work found no differences in posture as measured by Modified Dental Operator Posture Assessment Instrument compared to not alternating postures; however, all participants in the training group perceived their pain and posture were improved using an alternating seated/standing protocol.15 More research should examine proper standing postures and training in standing dentistry to effectively quantify if alternating between seated and standing postures improves ergonomics.
Instrument Selection and Considerations for Ergonomics
The fine, repetitive, and forceful movements dental hygienists perform while scaling and root planing may also contribute to MSDs, particularly in the wrist and forearms.5,6 Periodontal instruments vary in their shape, weight, diameter, and material. Changing the weight and diameter of the instrument may influence muscle activity as well as pinch force.
Dong et al16,41 in two separate studies found larger diameter (10 mm) instruments and lightweight instruments (15 g) required the least muscle load and pinch force during simulated scaling. Suedbeck et al17 examined instrument handle design and forearm muscle activity using commercially available instruments and found the largest instrument (11.1 mm) with the heaviest weight (23 g) generated the most muscle activity. The weight of the instrument appeared to also be a significant factor in generating more muscle activity. Based on research, smaller instrument diameters seem to increase muscle activity and pinch force while scaling. Additionally, heavier instruments may cause more strain on the muscle and grip when scaling.16,17,41
Scaling technique may also influence pinch force and muscle activity. Instrument manufacturers now offer instruments that use a modified scaling technique to remove deposits when scaling.42 Typical periodontal scaling technique with stainless steel instruments requires lateral pressure whereas a modified scaling technique with titanium nitride-infused stainless steel instruments uses a shaving technique with reduced lateral pressure, which may reduce pinch force and muscle activity. Suedbeck et al42 examined the two scaling techniques and found traditional scaling with lateral pressure required greater overall pinch force during scaling, and participants also preferred the instrument requiring a modified scaling technique compared to the instrument using a traditional scaling technique. While more research is needed on instrument design and scaling technique, dental hygienists may consider using instruments that are larger in diameter, round, tapered, and lightweight in an effort to reduce muscle activity and pinch force. Additionally, instruments requiring a modified scaling technique with reduced lateral pressure may decrease muscle load and pinch force.
Conclusion
Due to the nature of clinical practice, dental hygienists are at an increased risk for MSDs which may cause pain, stress, and, ultimately, affect career longevity. Ergonomic education and making informed decisions on everything from equipment to posture are important to start early in the career to combat biomechanical risk factors. With the information above, dental hygiene students, practicing dental hygienists, and educators may be able to make more informed decisions related to the use of loupes, seating alternatives while working, and instrument selection while scaling to improve ergonomics related to dental hygiene practice.
References
- Warren N. Causes of musculoskeletal disorders in dental hygienists and dental hygiene students: a study of combined biomechanical and psychosocial risk factors. Work. 2010;35:441–454.
- La Delfa NJ, Grondin DE, Cox J, Potvin JR, Howarth, Samuel J. The biomechanical demands of manual scaling on the shoulders & neck of dental hygienists. Ergonomics. 2017;60:127–137.
- Morse T, Bruneau H, Dussetschleger J. Musculoskeletal disorders of the neck and shoulder in the dental professions. Work. 2010;35:419–429.
- Akesson I, Johnsson B, Rylander L, Moritz U, Skerfving S. Musculoskeletal disorders among female dental personnel – clinical examination and a 5-year follow-up study of symptoms. Int Arch Occup Environ Health. 1999;72:395–403.
- Anton D, Rosecrance J, Merlino L, Cook T. Prevalence of musculoskeletal symptoms and carpal tunnel syndrome among dental hygienists. AJ J Ind Med. 2002;42:248–257.
- Netanely S, Luria S, Langer D. Musculoskeletal disorders among dental hygienist and students of dental hygiene. Int J Dent Hyg. 2020;18:210–216.
- Stambaugh JE, Calleros C, Siegel P, Nathe C. Evaluating the prevalence of musculoskeletal neck pain in dental hygiene students. J Dent Hyg. 2021;95:58–62.
- Darby ML, Walsh MM. Dental Hygiene: Theory and Practice. 4th ed. St. Louis: Saunders; 2015:145–160.
- Anu V, Suresh Babu AM, Madan Kumar KD. Insights about dental ergonomics among dental students: the need of the hour to recommend dental ergonomics in academic curriculum. J Adv Oral Res. 2018;949–954.
- Shaik AR. Dental ergonomics: basic steps to enhance work efficiency. Arch Med Health Sci. 2015;3:138–144.
- Hayes M, Osmotherly P, Taylor J, Smith D, Ho A. The effect of wearing loupes on upper extremity musculoskeletal disorders among dental hygienists. Int J Dent Hyg. 2014;12:174–179.
- Carpentier M, Aubeux D, Armengol V, Pérez F, Prud’Homme T, Gaudin A. The effect of magnification loupes on spontaneous posture change of dental students during preclinical restorative training. J Dent Educ. 2019;83:407–415.
- Ludwig EA, Tolle SL, Jenkins E, Russell D. Magnification loupes influence on neck and trunk flexion of dental hygienists while scaling-a pilot study. Int J Dent Hyg. 2021;19:106–113.
- De Bruyne MA, Van Renterghem B, Baird A, Palmans T, Danneels L, Dolphens M. Influence of different stool types on muscle activity and lumbar posture among dentists during a simulated dental screening task. Appl Ergon. 2016;56:220–226.
- Partido BB, Henderson R, Lally M. Impact of a seated-standing protocol on postures and pain among undergraduate dental hygiene students: a pilot study. J Dent Hyg. 2021;95:70–78.
- Dong H, Loomer P, Barr A, et al. The effect of tool handle shape on hand muscle load and pinch force in a simulated dental scaling task. Appl Ergon. 2006;38:525–531.
- Suedbeck JR, Tolle SL, McCombs G, Walker ML, Russell DM. Effects of instrument handle design on dental hygienists’ forearm muscle activity during scaling. J Dent Hyg. 2017;91:47–54.
- Haughie LJ, Fiebert IM, Roach KE. Relationship of forward head posture and cervical backward bending to neck pain. J Man Manip Ther. 1995;3:91–97.
- Gherig J, Sroda R, Sacuzzo D. Fundamentals of Periodontal Instrumentation and Advanced Root Instrumentation. 8th ed. Baltimore: Lippincott Williams & Wilkins; 2017.
- Rucker LM, Beattie C, McGregor C, Sunell S, Ito Y. Declination angle and its role in selecting surgical telescopes. J Am Dent Assoc. 1999;130:1096–1100.
- Chang BJ. Ergonomic benefits of surgical telescope systems: selection guidelines. J Calif Dent Assoc. 2002;30:161–169.
- Wilson C, Johnson T, Seiger C. Dental magnification loupes and head tilt angles among aental hygiene students and faculty: a comparative study. J Dent Hyg. 2021;95:59–64.
- Chang BJ. Guidelines for selecting economically correct surgical telescope systems. Dental Economics. 2003;93(11):84–91.
- Syme SE, Fried JL, Strassler HE. Enhanced visualization using magnification systems. J Dent Hyg. 1997;71:202–206.
- Aldosari MA. Dental magnification loupes: an update of the evidence. J Contemp Dent Pract. 2021;22:310–315.
- Perrin P, Eichenberger M, Neuhaus KW, Lussi A. Visual acuity and magnification devices in dentistry. Swiss Dent J. 2016;126:222–235.
- Urlic I, Verzak Z, Vranic D. Measuring the influence of galilean loupe system on near visual acuity of dentists under simulated clinical conditions. Acta Stomatologica Croatica. 2016;50:235–241.
- Mamoun JS. A rationale for the use of high-powered magnification or microscopes in general dentistry. Gen Dent. 2009;57:18–26.
- Dianat I, Sedghi A, Bagherzade J, Jafarabadi MA, Stedmon AW. Objective and subjective assessments of lighting in a hospital setting: implications for health, safety and performance. Ergonomics. 2013;56:1535–1345.
- Bly J, Jordre B. Improve visibility. Dimensionss of Dental Hygiene. 2015;13:18–23.
- Arnett M, Gwozdek A, Ahmed S, Beaubien H, Yaw K, Eagle I. Assessing the use of loupes and lights in dental hygiene educational programs. J Dent Hyg. 2017;91:15–20.
- Kissell D, Partido B, Moore W. Magnification and coaxial illumination in dental hygiene education: experience and attitudes of clinical educators. J Dent Hyg. 2019;93:7–15.
- Leggat PA, Kedjarune U, Smith DR. Occupational health problems in modern dentistry: a review. Ind Health. 2007;45:611–621.
- Pynt J, Higgs J, Mackey M. Seeking the optimal posture of the seated lumbar spine. Physiother Theor Pract. 2001;17:5–21.
- Hedman TP, Fernie GR. Mechanical response of the lumbar spine to seated postural loads. Spine. 1997;22:734–743.
- Dable RA, Pradnya WB, Babita YJ, Smita MI, Ashishkumar PK, Sunilkumar NN. Postural assessment of students evaluating the need of ergonomic seat and magnification in dentistry. J Indian Prosthodont Soc. 2014;14:51–58.
- Harrison DD, Harrison SO, Croft AC, et al. Sitting biomechanics part 1: review of the literature. J Manipulative Physiol Ther. 1999;22:9:594–609.
- Gandavadi A. Working postures in dental practitioners and dental students: relationships between posture, seating, and muscle activity. Available at: etheses.bham.ac./k/id/eprint/⯐/䁯/Gandavadi08PhD.pdf. Accessed August 17, 2022.
- Grobler SH, Mostert K, Becker P. The impact of a change in work posture from seated to stand-up on work-related musculoskeletal disorders among sewing-machine operators. Am J Ind Med. 2018;61:699–711.
- Hasegawa T, Inoue K, Tsutsue O, Kumashiro M. Effects of a sit-stand schedule on a light repetitive task. International Journal of Industrial Ergonomics. 2001;28(3-4):219–224.
- Dong H, Barr A, Loomer P, et al. The effects of periodontal instrument handle design on hand muscle load and pinch force. J Am Dent Assoc. 2006;137:1123–1130.
- Suedbeck JR, Armitano-Lago C. The effects of the traditional scaling technique versus a modified scaling technique on muscle activity and pinch force generation: a pilot study. J Dent Hyg. 2021;95:6–13.
From Dimensions of Dental Hygiene. September 2022; 20(9)14,16,18,21.

{kind=link}