
Early Detection of Type 2 Diabetes In Children and Adolescents
Following are assessment techniques that are easily implemented into routine dental hygiene practice.
This course was published in the December 2017 issue and expires December 2020. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the relationship between periodontal diseases and type 2 diabetes.
- Identify the components of the medical history and physical assessment that may reveal signs and symptoms of type 2 diabetes in pediatric and adolescent patient populations.
- Discuss the practice implications for oral health professionals in the effort to support early detection of type 2 diabetes in children and adolescents.
Periodontal disease is noted as the “sixth complication of diabetes”4 and evidence suggests that periodontal diseases adversely affect health outcomes among patients with diabetes.5 Diabetes affects all periodontal parameters, including bleeding scores, probing depths, attachment loss, and tooth loss.6–9 Patients with diabetes are five times more likely to be partially edentulous as those without diabetes.7 Other oral complications related to diabetes include: candidiasis, dental caries, gingivitis, lichen planus, neurosensory disorders (such as burning mouth syndrome), salivary dysfunction, taste impairment, and xerostomia.8
Periodontal destruction in children and adolescents with diabetes begins earlier than previously thought.10 These populations experience significantly increased gingival inflammation compared with control subjects, even after adjusting for oral hygiene levels.11
PERIODONTAL DISEASES AND TYPE 2 DIABETES
Periodontitis is preceded by gingivitis, which can be prevented through regular oral hygiene care.12 Individuals with uncontrolled, undiagnosed, or poorly controlled type 2 diabetes are more susceptible to periodontal diseases. These patients may demonstrate more severe periodontitis compared with those with adequate metabolic glycemic control.13 This is due to impaired antibacterial functions of neutrophils and wound healing and other biologic mechanisms in which infection (such as is caused by gingivitis and periodontitis) can increase insulin resistance in peripheral tissues.14 Cianciola et al15investigated the prevalence of periodontal disease in children with insulin-dependent diabetes mellitus (IDDM) and control subjects. Among children between the ages of 11 and 18, 9.8% of those with IDDM showed signs of periodontitis vs only 1.7% in the control group. In children age 10 or younger, Cianciola et al15 found no evidence of periodontitis in either group. However, other research documents the presence of gingivitis associated with diabetes in children as young as 5.16
The incidence of periodontal diseases in child and adolescent populations increases when they have type 2 diabetes with periods of hyperglycemia (fasting plasma glucose of 126 mg/dL or higher).17 Patients with hyperglycemia often present with elevated blood glucose levels that contribute to tissue breakdown, regardless of whether the hyperglycemia is caused by type 1 or type 2 diabetes.17A significant bidirectional relationship has been reported between hyperglycemia and periodontal diseases, suggesting that both diseases may share common pathways.17
A two-way reciprocal relationship has been shown to exist when the inflammatory process associated with periodontal disease releases pro-inflammatory cytokines.18 These cytokines play a key role in regulatory responses, including disrupting the ability to control insulin levels. The balance between pro-inflammatory and anti-inflammatory responses is also crucial in the progression of periodontal diseases.18
Most oral health professionals routinely note type 2 diabetes as a risk factor in periodontitis. Obesity and diabetes in younger patients should also be used as risk factors for the development and progression of periodontal diseases.19
MEDICAL HISTORY AND PHYSICAL ASSESSMENT
The American Dental Hygienists’ Association (ADHA) Standards for Clinical Dental Hygiene Practice define assessment as the “collection and analysis of systematic and oral health data in order to identify client needs.”20 Vital sign assessment is part of the Standards for Clinical Dental Hygiene Practice and includes temperature, pulse, respiration, and blood pressure. These provide a baseline for identifying potential or undiagnosed medical conditions. One in three Americans is diagnosed with hypertension, including children.21 This increase is more profound among those with an increased body mass index (BMI).22
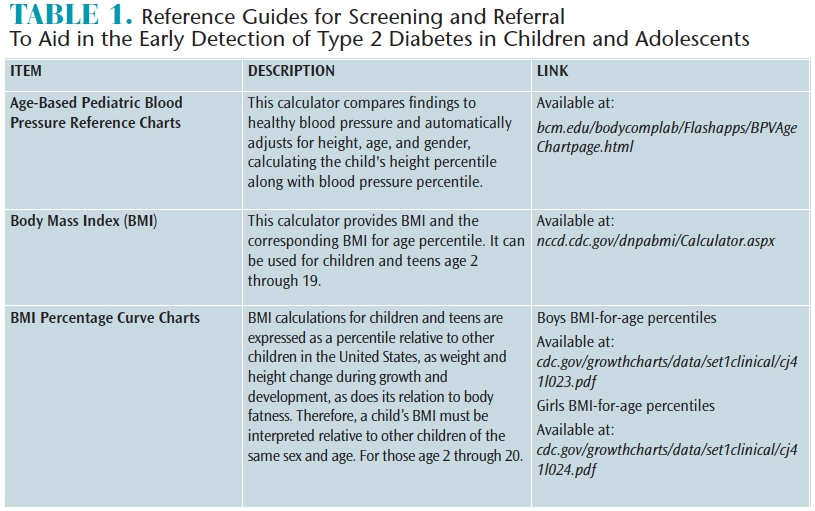
In both adult and pediatric patient populations, hypertension can increase the severity of periodontal diseases and cause other adverse health effects.23–25 Obtaining an accurate blood pressure reading is recommended by the American Academy of Pediatrics for all patients, beginning at age 3, to aid in early detection of blood pressure abnormalities.26 Hypertension in children and adolescents is determined by the patients’ height and gender, and is presented in a percentile curve chart (Table 1).27 Children with blood pressure readings higher than 120/80 are classified as pre-hypertensive. Environmental causes of hypertension include diet, exercise, and the health of the expectant mother.27 Genetic coding has shown several gene variants are linked to diabetes, hypertension, and metabolic syndromes.28 By routinely taking blood pressure readings in children and adolescents, oral health professionals can play important roles in the early detection of hypertension and other related conditions.
Childhood obesity is a significant risk factor for developing type 2 diabetes.19 Oral health professionals should include BMI as a component of vital sign assessment because of its impact on general and oral health. Comprehensive assessment should include an annual BMI calculation.21 In children and adolescents, BMI is categorized differently than in adults (Table 1). Patients with BMIs ranging from the 85th to the 95th percentile may indicate an abnormality in glucose metabolism. In these cases, a referral to a medical provider is recommended.21
Signs of type 2 diabetes in children and adolescents are not always listed on medical history forms. Often overlooked are physical signs and reported symptoms that can be detected during a routine dental hygiene appointment, including acanthosis nigricans, skin tags, dry itchy skin, poor general skin healing, and oral candidiasis.
As the obesity rates in children climb, so will the incidence of metabolic changes leading to type 2 diabetes. Skin changes are sometimes the first signs detected in a child or adolescent with undiagnosed type 2 diabetes. These skin changes—such as dry, irritated skin—may be observable by oral health professionals when securing the napkin around the patient’s neck.

Children and adolescents who are obese or have insulin resistance frequently present with a skin condition termed acanthosis nigricans.29Often caused by untreated hyperinsulinemia due to type 2 diabetes, acanthosis nigricans is a mucocutaneous disorder characterized by diffuse hyperpigmented areas of the skin, resulting in a velvety appearance.29 The affected areas appear dark and thickened and may be seen at the neckline, elbows, or on the backs of children’s hands.
Skin tags are another sign of type 2 diabetes in children.30 Flesh colored, skin tags can be observed in the neck and anterior chest area in children and adolescents with insulin sensitivity. Skin tags are harmless; however, they may represent insulin sensitivity in an asymptomatic child or adolescent.31
Oral health professionals should ask patients about dry itchy skin or the presence of any wound that does not appear to be healing.31Screening for the occurrence of frequent infections (including bladder infections) is also appropriate as part of screening for type 2 diabetes.32
During routine oral exams, candidiasis may be observed in children and adolescents with undiagnosed type 2 diabetes. Signs and symptoms of candidiasis include white patches on the tongue or other areas of the mouth and throat (Figure 1). Candidiasis is common among those with poorly controlled A1C levels.8,13,14,32 If blood glucose levels are not controlled, candidal colonization is likely.33 Oral candidiasis in an obese child or adolescent should alert oral health professionals to the likely presence of other health problems, including diabetes. Medical consultation with other health care providers may be indicated.
IMPLICATIONS FOR PRACTICE
Oral health professionals are well qualified to note the oral and systemic manifestations of diabetes and can actively contribute in the early detection of type 2 diabetes. Dental hygienists already routinely perform a thorough health assessment. A first step in reducing the type 2 diabetes epidemic may be to modify the approach in collecting health data to include a focus on signs and symptoms specifically related to type 2 diabetes. This should include BMI calculations,22 blood pressure measurement for all patients older than 3,34 and inquiring about returning or persistent infections.32
Oral health professionals should consider signs and symptoms of type 2 diabetes while completing the visual physical assessment of the head and neck, including looking for acanthosis nigricans, skin tags, and dry, itchy skin.29–31 Oral examination should include determining the presence of oral candidiasis, xerostomia, or other recurring infections.32,33
The ADHA Standards for Clinical Dental Hygiene Practice recommend referral to other medical providers when noticing any combination of these signs and symptoms.20 Perhaps the most important role oral health professionals play in the early detection of type 2 diabetes in children and adolescents is in educating patients and parents/caregiver on oral and systemic links.
CONCLUSION
Unfortunately, the prevalence of type 2 diabetes and obesity continues to grow at an alarming rate, which may also increase risk for periodontal diseases. In 2013, 285 million people were diagnosed with diabetes worldwide.11 Obesity is also a global epidemic, affecting all age groups, populations, and countries—regardless of socioeconomic status. Children with obesity are particularly at risk for health problems.12 As such, a new approach is needed to aid in detection. Disciplines that do not traditionally focus on diabetes/obesity as a routine component of evaluation, such as oral health care, should begin including these assessments to ensure early diagnosis and to prevent oral disease.13
ACKNOWLEDGMENTS
The authors would like to thank Juan F. Yepes, DDS, MD, MPH, MS, DrPH, FDS RCSEd, and Mike Fetscher for their help with this manuscript.
REFERENCES
- American Diabetes Association. Initial Evaluation and DiabetesManagement Planning. Diabetes Care. 2015;38(Supplement 1):S17–S19.
- WorldHealth Organization. Diabetes Fact Sheet.Available at: who.int/mediacentre/factsheets/fs312/en.Accessed November 11, 2016.
- BoydL, Gilblin L, Chadbourne D. Bidirectional relationship between diabetes mellitus and periodontal disease: state of the evidence. Canadian Journal of Dental Hygiene. 2012;46(2):93–102.
- Loe H. Periodontal disease: the sixth complication ofdiabetes mellitus.Diabetes Care. 1993;16:329–334.
- BorgnakkeW, Ylöstalo P, Taylor G, Genco R. Effectof periodontal disease on diabetes:systematic review of epidemiologicobservational evidence. J Clin Periodontol.2013;40:S135–S152.
- Bridges R, Anderson J, Saxe S, GregoryK, Bridges S. Periodontal status of diabeticand non-diabetic men:effects of smoking, glycemic control,and socioeconomic factors. J Periodontol.1996;67:1185–1192.
- EmamiE, deSouza RF,Kabawat M, Feine JS. Theimpact of edentulism on oral and generalhealth. Int J Dent. 2013;2013:498305.
- Lamster IB. Non-periodontal oral complications ofdiabetes mellitus. In: Lamster IB, ed. Diabetes Mellitus and Oral Health. Hoboken New Jersey: John Wiley & Sons; 2014:157–190.
- Khader Y, Dauod A, El-QaderiS, Alkafajei A, Batayha W. Periodontalstatusof diabetics compared with nondiabetics: a meta-analysis. J Diabetes Complications. 2006;20:59–68.
- GuravAN. Management of diabolicaldiabetes mellitus and periodontitis nexus: are we doing enough?World J Diabetes. 2016:7:50–56.
- Merchant AT, Oranbandid S, Jethwani W, et al. Oral carepractices and a1c among youth with type 1 and type 2 diabetes.J Periodontol. 2012;83:856–863.
- Tolle SL. Periodontal risk assessment. In: Darby M,Walsh M, eds. Dental Hygiene Theory and Practice. 4th ed.St. Louis: Elsevier; 2015:321–329.
- Llambes F, Arias-Herrera S, Caffesse R. Relationship between diabetesand periodontal infection. World J Diabetes. 2015;6:927–935.
- ArmitageGC. Potential impact of periodontalinfection on overall general health In: Darby M, Walsh M,eds. Dental Hygiene Theory and Practice. 4th ed. St.Louis: Elsevier; 2015:357–358.
- Cianciola L, Park B, Mosovich E, Genco R. Prevalenceof periodontal disease in insulin-dependent diabetes mellitus (juvenile diabetes). J Am Dent Assoc. 1982104:653–660.
- Oh TJ, Eber R, Wang HL. Periodontal diseases in the child andadolescent. J Clin Periodontol.2002;29:400–410.
- Chiu S, Lai H, Yen A, et al. Temporalsequence of the bidirectional relationshipbetween hyperglycemia and periodontal disease: a community-based study of5,885 Taiwaneseaged 35–44 years (KCIS No. 32). Acta Diabetol. 2015;52:123–131.
- AkramZ, Abduljabbar T, Abu Hassan M, et al. Cytokine profilein chronic periodontitis patients with and without obesity: a systematic review and meta-analysis. Dis Markers. 2016;2016:4801418.
- Eckel R, Kahn S, FerranniniE, et al. Obesity and type 2 diabetes: what can be unifiedand what needs to be individualized? Diabetes Care. 2011;34:1424–1430.
- American Dental Hygienists’ Association. Standards for Clinical DentalHygiene Practice. Available at: adha.org/resources-docs/2016-Revised-Standards-for-Clinical-Dental-Hygiene-Practice.pdf. Accessed November 11, 2017.
- Morandi A, Maffeis C. Predictorsof metabolic risk in childhood obesity. Horm Res Paediatr. 2014;82:3–11.
- Dumont D, Baker L, George E, Sutton N. Diabetes and BMI: health equity through early intervention ondysglycemia, and how providerscan help. R I Med J. 2016;99:33–36.
- UnitedStates Centers for Disease Control and Prevention. HighBlood Pressure Fact Sheet Data& Statistics. Available at: cdc.gov/dhdsp/data_statistics/fact_sheets/fs_bloodpressure.htm. Accessed November 11, 2017.
- Paizan MLM, Vilela-Martin JF. Is there an association between periodontitis and hypertension? Curr Cardiol Rev. 2014;10:355–361.
- Bassareo PP, Mercuro G. Pediatric hypertension: anupdate on a burning problem. World J Cardiol. 2014;6:253–259.
- MoyerV. Screening for Primary Hypertensionin Children and Adolescents: U.S. Preventive Services TaskForce Recommendation Statement. Ann Intern Med. 2013;159:613–619.
- BankerA, Bell C, Gupta-MalhotraM, Samuels J. Blood pressure percentile charts to identifyhigh or low bloodpressure in children. BMC Pediatr. 2016;16:16–98.
- de Oliveira S, da Cunha Nascimento D, Tibana R, et al. Elevated glycated hemoglobin levels impair bloodpressure in children and adolescentswith type 1 diabetes mellitus. Diabetol Metab Syndr. 2016;8:4.
- KutlubayZ, Engin B,Bairamov O, TüzünY. Acanthosis nigricans:A fold (intertriginous) dermatosis. Clin Dermatol. 2015;33:466–470.
- TabákA, Herder C, RathmannW, Brunner E, Kivimäki M. Prediabetes: a high-riskstate for diabetesdevelopment. Lancet. 2012;379:2279–2290.
- BustanR, Wasim D,Yderstraede K, Bygum A. Specific skin signs as a cutaneous marker of diabetes mellitus and the prediabetic state—a systematic review.Dan Med J. 2017;64:A5316.
- YeshitelaB, Gebre-Selassie S, Feleke Y. Asymptomaticbacteriuria and symptomatic urinary tract infections (UTI) in patientswith diabetes mellitusin Tikur AnbessaSpecialized University Hospital, AddisAbaba, Ethiopia.Ethiop Med J. 2012;50:239–249.
- Shenoy M, Puranik R, Vanaki S, Puranik S, Shetty P, Shenoy R. A comparative study of oral candidalspecies carriage in patients withtype1 and type2 diabetes mellitus. J Oral MaxillofacPathol. 201418:60.
- Hansen M, Gunn P, Kaelber D. Underdiagnosis ofHypertension in Children and Adolescents.JAMA. 2007;298:874.
Featured photo by BANANASTOCK/BANANASTOCISTOCK/GETTY IMAGES PLUS
From Dimensions of Dental Hygiene. December 2017;15(12):49-52.
