Automate Your Probing Process
How technological advances are changing the way probing depths are measured and recorded.
Periodontal probing and assessment of clinical attachment level and width of attached gingiva are essential elements of the routine periodontal examination. Manual probes are the traditional instruments used in the assessment of probing depth and their use has proven efficacy.1 However, the success of manual probing is dependent on probe selection, clinician skill, and documentation.
Current probing methods are subjective, with accurate measurements dependent on insertion force, positioning, and probe design.2 Other factors to consider include root morphology, diameter, gingival conditions (edematous or fibrotic), angulation, pocket contour, and the reading and recording of measurements.
First and foremost, probing accuracy hinges on the clinician’s knowledge of root morphology and skilled technique. When measuring a pocket, the depth of probe insertion can also be influenced by the presence or absence of inflammation. Research shows that when probing with limited force in the presence of inflammation, the tip stops at the level of intact connective tissue fibers.3 In healthy sites, the tip fails to reach the connective tissue attachment even with heavy force.4 Computerized or automated probing devices have been developed to address pressure consistency in order to improve the reliability of measurements, reduce patient discomfort, and aid the clinician with proper recording and documentation. Regardless of which type of probing modality is used, clinicians must use diligence and precision to navigate root contours in order to obtain accurate readings.
|
Figures 2 and 3 courtesy of |

AUTOMATED PROBING SYSTEMS AND RECORDING
In an attempt to overcome some of the technical challenges associated with manual probes, electronic probes have been developed that permit probe insertion with a controlled force and reduce the amount of variation encountered.5,6 The use of automated probing systems can further enhance accuracy and efficiency of the periodontal probing assessment. The resolution, depending on the instrument, varies from 0.2 mm to 1.0 mm. Variations in manual probing force, size and shape of tip, location of tip placement, detection or reference landmarks for attachment level probing, degree of gingival inflammation, and transcription reliability may adversely influence accuracy. Electronic probes can offer improved resolution, force control, and automatic recording. Previous research has also reported improved reproducibility of probing measurements.7
More recent studies show that automated probes and manual probes are similar in their reproducibility of measurements. A systematic review of the literature looked at the reproducibility of manual probes versus electronic probes when measuring clinical attachment level in subjects with untreated periodontitis. Researchers found that both probes demonstrated similar reliability when used by a calibrated examiner.8,9
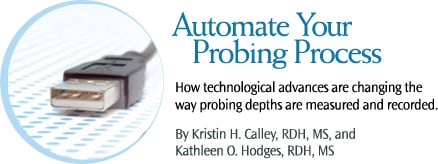
There are different types of automated probing systems on the market. Constant force probes, such as Florida Probe® (Florida Probe Corp), InterProbe™ (The Dental Probe Inc), and Probe One™ (The Dental Probe Inc), are the most widely used automated probes. Constant force probes provide objective and repeatable measurements of pocket depth with the ability to record attachment loss and record measurements. However, as with manual probing, automated probing systems require clinician experience to develop the necessary skills to effectively use the systems.
Florida Probe is an integrated system for periodontal assessment, automated recording, and self-care education (Figure 1). Florida Probe uses a constant force electronic probe connected to a computer for instantaneous data capture and storage. Probing forces are preset for 15 g of pressure. Once the probe is in place, the computer captures the measurements to the nearest 0.2 mm through a foot pedal.10
InterProbe and Probe One are integrated systems for periodontal probing, automated recording, and patient education. Both automated systems use an optical encoder handpiece that electronically reads and records pocket depth measurement. A constant gram force pressure of 15 g is used. The optical encoder handpiece electronically reads and records pocket depth measurement. The Inter- Probe is a first generation constant force probe that uses an independent computer system to record and print data. The Probe One attaches to any computer system using a USB adapter.
NEW AUTOMATED PROBE TECHNOLOGY
|
|

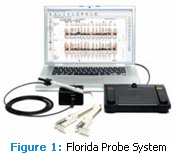
To build on the success of the current automated probing systems, researchers have been experimenting with ultrasonography for periodontal assessment.11,12 Ultrasound probing systems provide a noninvasive alternative to traditional probing methods (Figure 2).13 Though the ultrasound probes are not yet available, research is showing promising results, and manufacturers are in the process of obtaining Food and Drug Administration approval for these devices.
The US Probe (Visual Programs Inc) is an ultrasonographic instrument that uses diagnostic medical ultrasound techniques to automatically detect, map, and diagnose periodontal diseases. The ultrasound probe projects a very narrow beam of high-frequency (10 MHz to 15 MHz) ultrasound waves into the gingival sulcus. The probe then detects echoes of returning waves, which are reflected back from the tissues, eliminating the need for probing force into the sulcus. The ultrasound probe captures a series of observations (depth measurements plus contour) across the entire subgingival area as the probe tip passes along the gingival margin. As such, more information about present inflammation levels is obtained as opposed to just collecting readings at six individual sites. Figure 3 provides a diagram of an ultrasound probe in use. The US Probe is compatible with most computer systems.
The Perio-Imager (Perio-Imaging Inc) is an ultrasonographic digital imaging and diagnostic tool for detecting, mapping, characterizing, and evaluating the presence of and monitoring the treatment of periodontal diseases. The Perio-Imager requires a complete hardware and software system that includes a handpiece and a chairside computer console, in addition to the software needed for data acquisition, conversion, and display. The software converts the sonar wave signals that echo off the depth of the periodontal ligament’s outer boundary into a dimension (ie, pocket depth in millimeters). The Perio-Imager also detects the presence of calculus on the tooth’s surface so it can be more readily removed.
VOICE- AND FOOT-ACTIVATED TECHNOLOGY
The development of voice-activated software designed for dental and periodontal charting is expanding. Several dental software companies have integrated some form of voice-activation technology into their systems. These software programs are compatible with current office computer systems, eliminating the need to purchase new hardware. Also, by integrating a hands-free approach to data recording, cross contamination of patient records is reduced and the need for an assistant is eliminated.
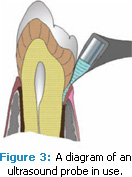
PerioPal® (PerioPal LLC) uses a voice command system that contains less than 100 words so only commands available for input are recognized (Figure 4). This voice command system differs from traditional dictation technologies that require clinicians to train the system to recognize their voices using individual words. The company claims that by using so few predetermined commands, voice recognition accuracy increases. The headset and microphone for this system are compatible with both Microsoft Windows XP and Mac (through Boot Camp/Parallels software) operating systems.
Patterson EagleSoft dental management software (Patterson Dental) integrates a voice module that uses the Microsoft Speech engine (Figure 5). The voice module uses dictation for voice recognition and its accuracy increases with continued use. EagleSoft is compatible with Microsoft Windows operating systems.
Dentrix dental management software (Henry Schein Practice Solutions) integrates VoicePro 5.0 for the recording of periodontal and restorative chartings (Figure 6). VoicePro 5.0 is a speech recognition tool that allows the clinician to record clinical charting, periodontal examinations, and clinical notes through speech recognition. VoicePro 5.0 is compatible with Microsoft Windows.
The Dental R.A.T. (Beckmer Products Inc) is a foot-operated mouse that records probe readings and operates intraoral cameras and digital X-rays (Figure 7). It allows the operation of dental software without the need for an assistant and its use reduces the risk of cross-contamination.
CONCLUSION
The differences between electronic probes and manual probes are based on comfort, cost of use, and time involved in measurement of clinical parameters, such as probing depths and clinical attachment levels. A definite advantage of computer-linked probes is they can record probe readings automatically. With automated systems, assistants are not needed for recording and clinicians do not need to transition from the mouth to a computer when recording readings.
Studies about automated probing dating from 1996 to 2009 are limited and evaluate pocket depth and/or clinical attachment level around teeth and implants in patients with untreated periodontitis or in periodontal maintenance patients. More clinical studies that evaluate the reliability and validity of automated probes alone and in comparison to manual probes for assessment of pocket depth, clinical attachment level in patients with periodontitis, and periodontal maintenance cases, are needed.
REFERENCES
- Academy of Periodontology. Position paper, diagnosis of periodontal diseases. J Periodontol. 2003;74:1237-1247.
- Mombelli A, Muhle T, Frigg, R. Depth-force patterns of periodontal probing. Attachment-gain in relation to probing force. J Clin Periodontol. 1992;19:295-300.
- Bulthuis HM, Barendregt DS, Timmerman,MF, Loos BG, van der Velden, U. Probe penetration in relation to the connective tissue attachment level: influence of tine shape and probing force. J Clin Periodontol. 1998;25:417-423.
- Barendregt DS, Van der Velden U, Timmerman MF, Van der Weijden GA. Comparison of two automated periodontal probes and two probes with a conventional readout in periodontal maintenance patients. J Clin Periodontol. 2006;33:276-282.
- Chamberlain AD, Renvert S, Garrett S, Nilveus R, Egelberg J. Significance of probing force for evaluation of healing following periodontal therapy. J Clin Periodontol. 1985;12:306-311.
- Garnick JJ, Keagle JG, Searle JR, King GE, Thompson WO. Gingival resistance to probing forces. II. The effect of inflammation and pressure on probe displacement in beagle dog gingivitis. J Periodontol. 1989;60:498-505.
- Wang SF, Leknes KN, Zimmerman GJ, Sigurds – son TJ, Wikesjo UM, Selvig KA. Reproducibility of periodontal probing using a conventional manual and an automated force-controlled electronic probe. J Periodontol. 1995;66:38-46.
- Silva-Boghossian CM, Amaral CS, Maia LC, Luiz RR, Columbo AP. Manual and electronic probing of the periodontal attachment level in untreated periodontitis: a systemic review. Evid Based Dent. 2009;10:39.
- Niederman R. Manual and electronic probes have similar reliability in the measurement of untreated periodontitis. J Dent. 2008;36:651-657.
- Araujo MW, Hovey KM, Benedek JR, et al. Reproducibility of probing depth measurement using a constant-force electronic probe: analysis of inter- and intraexaminer variability. J Periodontol. 2003;74:1736-1740.
- Tsiolis FI, Needleman IG, Griffiths GS. Periodontal ultrasonography. J Clin Periodontol. 2003;30:849-854.
- Hinders MK, Lynch JE, McCombs GB. Clinical tests of an ultrasonic periodontal probe. Reviews of Progress in Quantitative Nondestructive Evaluation. 2002;21:1880-1887.
- Lynch JE, Hinders MK. Ultrasonic device for measuring periodontal attachment levels. Rev Sci Instrum. 2002;73:2686-2688.
From Dimensions of Dental Hygiene. February 2011; 9(2): 44-47.

{kind=link}