Anterior Instrumentation
Purposeful assessment, correct instrument selection, and effective technique are key to maintaining health in the anterior dentition.
Careful examination of gingival tissue, probe depths, bleeding, attachment loss, and radiographic changes are essential to the implementation of hand instrumentation. The topography of the anterior sextants is examined to aid in instrument choices. Consider embrasure spaces, recession, and gingival tone and thickness (eg, soft tissue biotype, which includes gingival width, gingival thickness, papilla height/proportion, and crown width/height ratio).
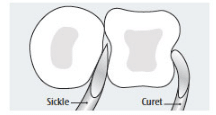
A type I healthy embrasure with tight tissue calls for a narrow blade. Shank length depends on pocket depth and its strength on tenaciousness (ie, attachment mode) of the deposit. In a type III open embrasure, a wide curet blade can adapt best. Although a sickle will fit into this embrasure, it is not effective due to its straight cutting edges and point, which may cause root striations. An anterior sickle will insert easily in areas with significant recession and root exposure. A curet tip, however, has the curvature needed to adapt to the root’s proximal concavities and concave and convex surfaces, while a sickle does not (Figure 1).
Soft tissue biotype does not seem to affect the results of scaling and root planing when pocket depths are greater than 3 mm; however, gingivae with less than 3 mm of depth exhibit more shrinkage in thin vs thick tissue.1 Therefore, in pathological pocket depths, instrument choice and instrumentation technique are paramount to successful therapy.
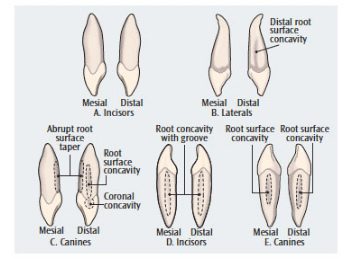
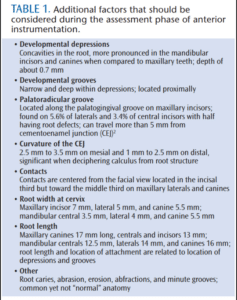
During assessment, recall of normal anterior root anatomy in both arches is important for instrument selection and successful debridement (Figure 2). Table 1 lists additional factors that should be considered during the assessment phase of anterior instrumentation.2
The root of an anterior tooth will feel different depending on the level of the attachment. For example, on the mandibular central incisor mesial surface, the depression deepens as it descends apically. With a 6 mm periodontal pocket, the depression at the apical end of the pocket will be deeper than at the cementoenamel junction (CEJ). On this same tooth, the cervix would be only 3.5 mm wide, as the root narrows and tapers toward the apex. Therefore, a mini- or micro-mini-bladed curet is a superior choice to reach the root’s midline on the proximal near the cervix. It also permits reaching the pocket depth due to the instrument’s long shank length. If calculus lies at the epithelial attachment and is tenacious, a periodontal file is ideal to reach and fragment the deposit. An alternative fulcrum, such as an opposite arch, might aid in navigating the pocket. If a suspected deposit is located on the proximal and will not budge, consider the normal contact and CEJ locations, as well as root anatomy, to decide whether to continue debriding or reevaluate at a later time.
INSTRUMENT CHOICES
The mandibular anterior segment is a common area for burnishing, especially on surfaces farthest from the clinician when sitting at a 12 o’clock position. Previous burnishing can be rectified with small and narrow Hirschfeld working files that enable access to the subgingival environment when the gingiva is taut. In fact, these files adapt better than curets due to their narrow width. The Hirschfeld 9/10 was designed for the anterior; however, the 3/7 and 5/11 adapt well and may be more effective (Figure 3). Alves et al3 showed that files and curets both left about 1 mm of attachment trauma and that neither was more significant in producing injury. Therefore, the use of Hirschfeld files near the attachment is safe and advantageous because the file is not placed underneath the deposit, as a curet would be.
Double- and single-bladed anterior sickles, such as H6/H7, are reserved for supragingival and minimal subgingival applications—gingival tone permitting. Elastic gingiva allows a sickle to be inserted subgingivally; however, the blades are straight and not satisfactorily adapted to curved surfaces like the roots of anterior teeth. Use a sickle scaler where appropriate, but not for complete root debridement.
There are a plethora of area-specific curets, each with unique characteristics. Families include the Gracey, Turgeon, and Vision with standard, extended shank, mini-bladed, and micro-mini-bladed designs (Table 2). With tight gingival tissue and type I embrasures, the Gracey 1/2 is ideal because of its narrow blade width. Selection of an extended shank, mini-blade, or micro-mini-blade depends on pocket depth and root anatomy. Limited research reveals conflicting results. Laboratory studies concluded the extended shank curet removes more root deposit than the standard anterior gracey.4,5 Conversely, an in vivo comparison between a rigid long-shank Gracey and a standard Gracey curet revealed no statistically significant difference in plaque or calculus removal.6 These investigators noted that clinician time and expertise probably impacted results more than instrument design. Additional research is needed to study the multitude of hand instrument options in varying sites and situations.
Posterior area-specific, universal, and double-bladed area-specific curets (Figure 4), as well as diamond files, are possibilities for anterior regions. At times, the curvature of a mesial or distal posterior area-specific instrument adapts best to the gingival contour and root. Specifically, the mesial ends—11 and 12—are useful in isolated situations due to the minor curvature of the shank. Universal curets are beneficial on distal surfaces of canine teeth, as well as other surfaces. Double-bladed area-specific instruments adapt to the distal of one tooth and the mesial of the adjacent tooth without changing ends. Diamond-coated files are indicated for fine scaling and root planing predominantly in root depressions. Applying this instrument with endoscopic therapy is ideal because of its abrasiveness. The ability to directly observe its use helps complete the debridement without removing unnecessary root surface.

click to view
INSTRUMENTATION

Instruments must be sharp and correctly contoured. Dulling or poor contouring results in the clinician needing to use more force, which contributes to fatigue and patient discomfort. This heavy-handed approach also raises the risk of burnishing the deposit.
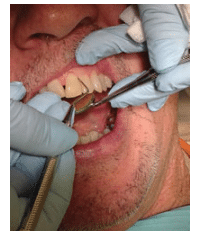
The traditional fulcrum is applicable for most situations; however, variations are necessary, such as an opposite arch (Figure 5), finger-on-finger, cross-arch, and instrument-across-finger fulcrums (Figure 6). These alternatives encourage correct principles of adaptation and activation, as well as support patient comfort and efficacy. Many anomalies can be present in anterior segments, such as rotated, missing, or supernumerary teeth, indicating the need for alternative fulcrum placement. Mobility from traumatic occlusion and periodontitis presents another challenge, and the finger-on-finger fulcrum is beneficial in this situation.
The many cutting edges on the Hirschfeld file will easily fragment calculus when placed parallel to and directly on the deposit. The channeling process is not used as with curets.7,8 Instead, an inward and short pull stroke is activated. After initial fracturing, the same working file and curets follow. Avoid placing the cutting edges directly on the root surface in the absence of calculus because of the risk of sensitivity or roughened root surface. This procedure is delicate and deliberate, yet forceful for a very limited location and duration.
Make a conscious effort to adapt the terminal end of an anterior curet or sickle. No matter if an extended shank, mini-bladed, or standard curet is chosen, only the tip or terminal 1 mm to 2 mm will be adapted to achieve the best channeling. Adapting the middle aspect of the blade should be avoided for multiple reasons, including reduced efficiency, effectiveness, and thoroughness, as well as increased trauma and pain for the patient. The toe or point of the instrument will project into the gingival tissue.
At times, the blade of a curet can be longer than the width of an anterior tooth’s root. For this reason, the curet toe placed toward the root apex is an effective approach on facials and linguals (Figure 7). Horizontal and oblique strokes are engaged and care is taken not to drag the curet toe on the attachment to prevent damage. Mentally visualizing these surfaces as isolated from the mesial and distal allows focus and localized applications. It is vital to evaluate the line angles because of the division of the tooth into three surfaces instead of two. Facial or lingual pocket depth helps determine instrument choice. A very shallow sulcus or pocket could be treated with a conventional Gracey 1/2 with this approach. Conversely, the base of a very deep pocket could not be treated this way because the blade would not be long enough. Instead, a micro- or mini-bladed curet would be used with vertical and oblique strokes.
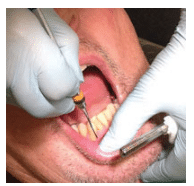 FIGURE 5. An opposite-arch fulcrum may be appropriate during anterior instrumentation.
FIGURE 5. An opposite-arch fulcrum may be appropriate during anterior instrumentation.
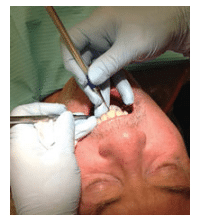 FIGURE 6. In anterior instrumentation, an instrument-across-finger fulcrum on the maxillary lingual may be most effective.
FIGURE 6. In anterior instrumentation, an instrument-across-finger fulcrum on the maxillary lingual may be most effective.
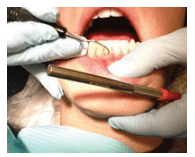 FIGURE 7. When the blade of a curet is longer than the width of an anterior tooth’s root, the curet toe should be placed toward the root apex.
FIGURE 7. When the blade of a curet is longer than the width of an anterior tooth’s root, the curet toe should be placed toward the root apex.
It is essential to visually estimate the blade-to-tooth angle. A greater or less than ideal angle creates burnishing and trauma. When the ideal 70° to 80° blade-to-root angle is achieved on proximals, the shank of straight-shanked instruments should slightly cross the buccal or lingual surface. This angle is too closed if the straight shank is leaning near the midline of an anterior tooth’s crown (Figure 8).
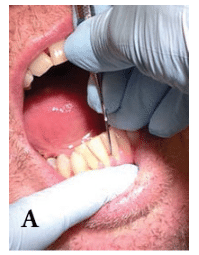 FIGURE 8. Standard fulcrum with correct (A)blade-to-root angle.
FIGURE 8. Standard fulcrum with correct (A)blade-to-root angle.
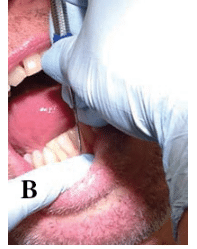 FIGURE 8. Incorrect (B) blade-to-root angle.
FIGURE 8. Incorrect (B) blade-to-root angle.
Modulation of firm to light pressure is always appropriate when moving from heavy tenacious to finer calculus elimination. The activation stroke is equally balanced between the pressure on the fulcrum and grasp. Care should be taken to avoid pressing downward (or upward) on the fulcrum finger too much, especially in the mandibular anterior. Excessive pressure results in residual soreness in the temporomandibular joint area.
CONCLUSION

Anterior teeth are not compromised or lost as often as posterior teeth, due to root length and less complex anatomy. It is, however, an essential area to thoroughly debride for health and esthetics. Purposeful assessment, instrument selection, and instrumentation are vital. One study examining only single rooted teeth demonstrated that nonsurgical and surgical periodontal therapies are effective, severe interproximal bone loss and infrabony defects worsen results, and tooth/site factors influence outcomes more than patient factors.9 Therefore, it is important to be mindful of all aspects that contribute to efficacy in anterior regions. The attention to detail during the assessment and care planning phases contributes to successful implementation.
Debridement involves many factors such as pain management, sharp instruments, adaptation of the terminal 1 mm to 2 mm of a curet, and modulating pressure (Table 3). A seemingly routine skill, such as debridement in anterior sextants, involves critical thinking and self-assessment of decision making. Clinician motivation and self-assessment greatly influence the learning of effective root debridement.10 Remaining willing to try new instruments and observe instrument choices and technique in anterior sextants will enhance motivation and outcomes.
REFERENCES
- You HK. Association of gingival biotype with the results of scaling and root planing. J Periodontal Implant Sci. 2013;43:283–290.
- Kogon SL. The prevalence, location and conformation of palato-radicular grooves in maxillary incisors. J Periodontol. 1986;57:231–234.
- Alves R, Machion L, Casati MZ, Nociti Junior FH, Sallum EA, Sallum WA. Clinical attachment loss produced by curettes and periodontal files. J Int Acad Periodontol. 2004;6:76–80.
- Landry C, Long B, Singer D, Senthilselvan A. Comparison between a short and a conventional blade periodontal curet: an in vitro study. J Clin Periodontol. 1999;26:548–551.
- Singer DL, Long BA, Lozanoff S, Senthilselvan A. Evaluation of a new periodontal curet. An in vitro study. J Clin Periodontol. 1992;19:549–552.
- Nagy RJ, Otomo-Corgel J, Stambaugh R. The effectiveness of scaling and root planing with curets designed for deep pockets. J Periodontol. 1992;63:954–959.
- Hodges KO. Incorporate channeling into instrumentation. Dimensions of Dental Hygiene. 2013;11(7):36–38.
- Hodges KO. Channeling for success. Dimensions of Dental Hygiene. 2013;11(5):34–37.
- Kim TS, Schenk A, Lungeanu D, Reitmeir P, Eickholz P. Nonsurgical and surgical periodontal therapy in single-rooted teeth. Clin Oral Invest. 2007;11:391–399.
- König J, Rühling A, Schlemme H, Kocher T, Schwahn C, Plagmann HC. Learning root debridement with curettes and power-driven instruments in vitro: the role of operator motivation and self-assessment. Eur J Dent Educ. 2002;6:169–75.
From Dimensions of Dental Hygiene. September 2014;12(9):48–49,50,52–53.

{kind=link}