All Sugars Are Not Created Equal
While it is well known that consuming too much sugar has negative consequences, emerging research is demonstrating that high-fructose corn syrup may exert specific, unique effects on both systemic and oral health.
This course was published in the June 2015 issue and expires June 30, 2018. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Compare and contrast high-fructose corn syrup (HFCS) and refined sugar.
- Discuss the composition of HFCS.
- Identify the effects of fructose on systemic and oral health.
Studies are emerging that link consumption of high-fructose corn syrup (HFCS) with heightened risk of diabetes, heart disease, obesity, cancer, dementia, liver failure, and caries. In Europe, glucose-fructose syrup (GFS) is the official name used on ingredient labeling, although this sweetener is sometimes is referred to as isoglucose because the production process uses isomerization enzymes. Within the European Union (EU), the Sugar Regime regulates the allowed production quota. Currently, production of GFS is limited to about 5% of total sugar production in the EU. Therefore, wide-scale replacement of sugar has not occurred in Europe and it remains a small market.1 This is not the case in the United States. American annual consumption of this additive is estimated to be the highest in the world and it is important for health care providers and consumers alike to understand the oral and systemic ramifications associated with the ingestion of HFCS.2
COMPARATIVE CONSIDERATIONS BETWEEN SUCROSE AND HIGH-FRUCTOSE CORN SYRUP
Today, Americans ingest most of their added sugar as table sugar or sucrose and HFCS.3 HFCS and refined sugar are not biochemically identical, nor are they processed by the body in the same way. Sucrose is a disaccharide with one molecule of glucose tightly bound to a molecule of fructose in a 50% glucose and 50% fructose ratio. The chemical link between glucose and fructose is extremely stable, making the sweetener resistant to breakdown when it is boiled or baked. In the gut, a group of enzymes called brush-border hydrolases digest all dietary polysaccharides and disaccharides, including sucrose. The small intestine is lined with fingerlike projections called villi that are composed of epithelial cells. When dietary sucrose comes in contact with the villi, a hydrolase (sucrase) is produced. The digestion of sucrose begins in the duodenum, where it is cleaved into free glucose and fructose by sucrase. As an enzyme, sucrase is a specialized protein designed to recognize, fit, and cleave the chemical bond between fructose and glucose. Once enzymatic cleavage of sucrose has occurred, the resultant mono-saccharides (glucose and fructose) are taken up by a specialized transport system in the wall of the small intestine and moved into circulation. This system carries the newly formed mon-saccharides to the liver for further processing.
After leaving the liver, glucose travels to nearly every cell in the body where insulin facilitates its cellular uptake for energy production. Metabolic breakdown of glucose is achieved through glycolysis, which converts glucose to pyruvate (Figure 1). Pyruvate is an acidic compound that can enter either aerobic or anaerobic respiration to produce energy. The metabolism of fructose, on the other hand, occurs through the complex process of fructolysis.4 One important by-product of fructolysis is glyceraldehyde, which can be utilized to convert glycerol to glycerol-1-phosphate, a substrate in the synthesis of triacylglycerol. In mammals, the major site for triacylglycerol storage is in the cytoplasm of adipose cells.5 Unlike glycolysis, which can take place in nearly all tissues, fructolysis occurs primarily in the liver.4
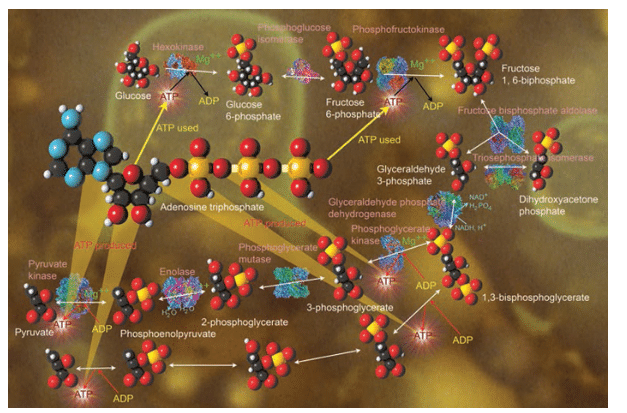
FIGURE 1. CAROL AND MIKE WERNER / SCIENCE SOURCE
In the manufacture of HFCS, sugars are extracted from corn through a chemical and enzymatic processes. The resultant syrup is a chemically and biologically novel product in which fructose and glucose exist as mono-saccharides. Because there is no chemical bond between fructose and glucose molecules, no digestion is required before these mono-saccharides are rapidly absorbed into the bloodstream. It is this difference in metabolism that has many experts concerned about systemic and oral consequences of HFCS ingestion.
The concentration of fructose in HFCS solution can vary.6,7 The most common forms of HFCS contain either 42% or 55% fructose, and these are referred to as HFCS 42 and HFCS 55, respectively. HFCS 42 is mainly used in processed foods, cereals, baked goods, and some beverages, HFCS 55 is used primarily in soft drinks.7
Research has found that the quality and composition of HFCS added to popular beverages can be much higher in fructose than the traditional HFCS 55.8 Researchers analyzed the five most popular brands of HFCS-sweetened sodas and found that they contained fructose-glucose ratios of 60/40 instead of the traditional 50/50 ratio. Because HFCS is available in higher concentrations,8,9 the higher fructose content may be the result of blending of HFCS-90 with HFCS-55 or glucose syrup.8,10 Without specification of the actual fructose content and possible blend of HFCS used, it is unclear exactly how much added fructose is contained in food and beverage products sweetened with HFCS. The increased concentration of fructose in sweetened beverages has the potential to affect the health and well-being of the estimated 88% of American children and adolescents who consume sweetened beverages on a daily basis.11
THE FRUCTOSE DEBATE
Recently, fructose has been the focus of attention in a debate on the possible adverse health effects of dietary sweetening agents. Some studies suggest that fructose is involved in the development of obesity and associated metabolic diseases such as heart disease and diabetes mellitus.12–14 It has been hypothesized that fructose may encourage overeating, which leads to obesity, because it is less satiating than other nutrients. More evidence is needed, however, to demonstrate this effect.12 While some experts suggest that fructose’s effect on body weight is the result of an increased energy intake unbalanced by increased physical activity, other investigators hypothesize that fructose increases appetite through stimulation and inhibition of appetite-controlling hormones and regions of the brain that affect hunger.12–14 Interestingly, increases in fructose consumption have paralleled the increasing prevalence of obesity in the US.15
The increasing prevalence of obesity is often discussed as an environmental phenomenon related to the types of foods consumed in modern society.12 As a component of HFCS, the substantial increase in the use of fructose as a sweetener and its potential role in the current obesity epidemic continues to be a focus of several clinical investigations.16–19
 In order to grasp the effects of fructose on appetite, the mechanism of hunger must be understood. Fuel sensing and appetite are both controlled by the hypothalamus and hunger is also influenced by an integrated network of other brain regions associated with the drive to eat.19 While it has been established that glucose ingestion decreases hypothalamic activity in humans,20,21 the effects of fructose on the hypothalamus are less clear. Bray et al18 attempted to clarify the role fructose plays on brain activity associated with appetite by employing functional magnetic resonance imaging (fMRI) techniques. The study team assessed the effects of glucose and fructose ingestion in human subjects on regional cerebral blood flow (CBF)—often used as an indirect marker of neuronal activation. The team demonstrated that the ingestion of glucose, but not fructose, reduced cerebral blood flow and, thus, activity in specific brain regions that regulate appetite. Reward processing was also decreased. Additionally, glucose ingestion produced increased ratings of satiety and fullness. When fructose was consumed, the study participants’ brain responses were much different. The investigators showed that fructose induced a small, transient increase in hypothalamic activity.22 Fructose consumption also did not deactivate a specific brain region known as the striatum. Hypothalamic and striatal deactivation occur when initially hungry individuals reach satiety.23,24 The research team further demonstrated that fructose ingestion reduced CBF in the hippocampus—a region in the brain that is important to memory function and emotional responses to food intake.25
In order to grasp the effects of fructose on appetite, the mechanism of hunger must be understood. Fuel sensing and appetite are both controlled by the hypothalamus and hunger is also influenced by an integrated network of other brain regions associated with the drive to eat.19 While it has been established that glucose ingestion decreases hypothalamic activity in humans,20,21 the effects of fructose on the hypothalamus are less clear. Bray et al18 attempted to clarify the role fructose plays on brain activity associated with appetite by employing functional magnetic resonance imaging (fMRI) techniques. The study team assessed the effects of glucose and fructose ingestion in human subjects on regional cerebral blood flow (CBF)—often used as an indirect marker of neuronal activation. The team demonstrated that the ingestion of glucose, but not fructose, reduced cerebral blood flow and, thus, activity in specific brain regions that regulate appetite. Reward processing was also decreased. Additionally, glucose ingestion produced increased ratings of satiety and fullness. When fructose was consumed, the study participants’ brain responses were much different. The investigators showed that fructose induced a small, transient increase in hypothalamic activity.22 Fructose consumption also did not deactivate a specific brain region known as the striatum. Hypothalamic and striatal deactivation occur when initially hungry individuals reach satiety.23,24 The research team further demonstrated that fructose ingestion reduced CBF in the hippocampus—a region in the brain that is important to memory function and emotional responses to food intake.25
While additional research is needed to clarify fructose’s role in hunger and satiety, obesity is affecting the quality of life of many American adults and children. Obesity-related conditions—such as heart disease, stroke, type 2 diabetes, and certain types of cancer—represent the leading causes of preventable death.26 Overconsumption of unnecessary calories is directly related to weight gain. As such, health care professionals should guide their patients toward decreased consumption of sweeteners—including HFCS.
CARDIOVASCULAR DISEASE
The American Heart Association (AHA) recommends limiting the amount of ingested food with added sugars to no more than half of the daily discretionary calories allowance. For most American women, this is no more than 100 calories per day or about 6 teaspoons of sugar. For men, it is 150 daily calories or about 9 teaspoons of sugar. The AHA recommendations focus on all added sugars without singling out any particular type.27 However, there are no universally accepted limitations on added sugar consumption and dietary recommendations.
The Institute of Medicine recommends that added sugars make up less than 25% of total calories, while the World Health Organization recommends less than 10%.28 Regardless of which dietary recommendations are used or what type of sweetener is ingested, many Americans consume more added sugar than is recommended for a healthy diet.28 Studies show that high levels of sugar consumption are correlated with an increased risk of death due to cardiovascular disease.28 Further, regular consumption of sugar-sweetened beverages (defined as seven servings or more per week) is associated with an increased risk of dying from cardiovascular disease.28 The American Beverage Association (ABA) issued a rebuttal to this study stating: “When it comes to risk for heart disease, there is nothing unique about the calories from added sugars, or sugar-sweetened beverages.”29
DIABETES
Global diabetes prevalence has more than doubled over the past three decades, with nearly one in 10 adults affected worldwide.30 The significant rise in rates of type 2 diabetes is thought to link to dyslipidemia, hypertension, and insulin resistance.31 The high prevalence of obesity associated with economic development may be the strongest risk factor for type 2 diabetes.31 Clearly, there is myriad risk factors at play. One controversial hypothesis is that excessive sugar intake may be a primary and independent driver of rising diabetes rates.31 Previous research has shown that sugars added to processed food, particularly fructose, can contribute to obesity.31 In an effort to understand worldwide diabetes development, researchers conducted a statistical analysis of panel data to empirically evaluate whether changes in sugar availability may account for the divergence in diabetes prevalence. By analyzing data on sugar availability and diabetes rates from 42 countries over the past decade, researchers found that high sugar levels in a population’s food supply were linked to increased rates of diabetes.31 Researchers found that the prevalence of diabetes in a population increased by 1% for every individual who consumed an extra 150 calories from sugars per day. A 150-calorie increase from other types of food only caused only a 0.1% increase in the rate. Additionally, results showed that diabetes rates increased the longer a population was exposed to excess sugar, and it decreased when sugar availability went down. Interestingly, countries that use HFCS in their food supply had a 20% higher prevalence of diabetes than countries that did not use it.31 The paper reported that out of 42 countries studied, the US had the highest per-capita consumption of HFCS.31
DENTAL CARIES
Dental caries should be part of all discussions related to sugar and health. Research on a link between sucrose and fructose ingestion and dental caries development, however, is not very compelling. A 2001 systematic review of the literature concluded that the association between tooth decay and sugar ingestion is weak in light of today’s widespread use of fluoride.32 Another 2014 systematic review found that evidence substantiating an association between sugar ingestion and caries is moderate.33
Numerous studies have implicated Streptococcus mutans as the main causative bacterial agent of dental caries.34 The host diet—especially ingestion of dietary sugars—is important for promoting the cariogenicity of S. mutans. Sucrose has been widely studied for its role in caries promotion. Of particular interest to oral health professionals is the ability of S. mutans to utilize sucrose as a substrate for adhesion-enabling glucan production. S. mutans also can metabolize various carbohydrates into organic acids, which may lead to the destruction of the tooth surface. It also has been demonstrated that sucrose plays an important role in the biofilm formation of S. mutans cells.35
Less widely studied is the role of fructose in caries production. To date, there appears to be only one study that looks specifically at this relationship, and it is an in vitro study, which makes real-life extrapolation of the results problematic.36 The study suggests that in the presence of HFCS, the cariogenicity of S. mutans may be different than the cariogenicity of S. mutans grown on sucrose. This investigation observed bacteria grown on media containing either HFCS or sucrose and found the bacterial colonies grown on sucrose were thicker, while the HFCS-grown colonies were less adherent.36 In light of the fact that bacterial adherence is a critical factor in caries etiology, this laboratory study indicates that HFCS may hinder caries lesion development. Again, it must be cautioned that the results of this in vitro investigation cannot be arbitrarily applied in biological models.
Not enough research has been conducted on the association between HFCS and caries to assume a causal relationship. Further in vivo research is necessary to clarify the role of HFCS ingestion in caries development or inhibition.
CONCLUSION
While the debate as to whether excessive consumption of HFCS or fructose alone leads to serious systemic and oral ramifications continues, one thing is clear. In today’s society, individuals are consuming sugar and other sweeteners in quantities that are overwhelming their metabolic systems. Regardless of what type of sweetener is ingested, moderation is the key. Oral health professionals are advised to keep abreast of developing research as more is learned about the effects of HFCS on oral and systemic health.
REFERENCES
- The European Food Information Council. Frequently Asked Questions. Available at: eufic.org/index/en. Accessed May 22, 2015.
- Goran MI, Ulijaszek SJ, Ventura EE. High fructose corn syrup and diabetes prevalence: a global perspective. Glob Pub Health. 2013; 8:55–64.
- Jabr F. Is sugar really toxic? Sifting through the evidence. Available at: blogs.scientificamerican. com/brainwaves/2013/07/15/is-sugar-really- toxicsifting- through-the-evidence. Accessed May 22, 2015.
- Jamerson A. The digestion and absorption of sucrose. Available at: healthy eating .sfgate.com/ digestion-absorption-sucrose-3680.html. Accessed May 22, 2015.
- Berg JM, Tymoczko JL, Stryer L. Triacylglycerols are highly concentrated energy stores. In: Biochemistry. 5th ed. New York: WH Freeman; 2002.
- Weingarten H. The secrets of manufacturing high fructose corn syrup. Available at: blog. fooducate. com/ 2012/10/09/the-secrets-of-manufacturing- high-fructose-corn-syrup. Accessed May 22, 2015.
- United States Food and Drug Administration. High Fructose Corn Syrup: Questions and Answers. Available at: fda.gov/Food/IngredientsPackagingLabeling/ FoodAdditivesIngredients/ ucm324856.htm. Accessed May 22, 2015.
- Walker RW, Dumke KA, Goran MI. Fructose content in popular beverages made with and without high-fructose corn syrup. Nutrition. 2014; 30:928–935.
- ADM. Sweeteners. Available at: origin. adm . com/en-US/ products/ food/ sweeteners/ Pages/ default.aspx. Accessed May 22, 2015.
- Parker K, Salas M, Nwosu V. High fructose corn syrup; production, uses and public health concerns. Biotechnol Mol Biol Rev. 2010; 5:71–78.
- Han E, Powell L. Consumption patterns of sugar sweetened beverages in the United States. J Acad Nutr Diet. 2013;113:43–53.
- The European Food Information Council. Science Briefs. Fructose: is public health action necessary? Available at: eufic.org/ page/en/ show/ latest-science-news/page/LS/fftid/Fructose-is-public- health-action-necessary. Accessed May 22, 2015.
- Tappy L, Mittendorfer B. Fructose toxicity: is the science ready for public health actions? Curr Opin Clin Nutr Metab Care. 2012;15:357–361.
- Tappy L. Q&A: Toxic effects of sugar: should we be afraid of fructose? BMC Biology. 2012; 10:42.
- Page KA, Chan O, Arora J, et al. Blood flow in brain regions involved with appetite and reward pathways. JAMA. 2013;309:63–70.
- Havel PJ. Dietary fructose: Implications for dysregulation of energy homeostasis and lipid/ carbohydrate metabolism. Nutr Rev. 2005; 63:133–157.
- Jürgens H, Haass W, Castañeda TR, et al. Consuming fructose-sweetened beverages increases body adiposity in mice. Obes Res. 2005; 13: 1146–1156.
- Bray GA, Nielsen SJ, Popkin BM. Consumption of high-fructose corn syrup in beverages may play a role in the epidemic of obesity. Am J Clin Nutr. 2004;79:537–543.
- Morton GJ, Cummings DE, Baskin DG, Barsh GS, Schwartz MW. Central nervous system control of food intake and body weight. Nature. 2006;443: 289–295.
- Liu Y, Gao JH, Liu HL, Fox PT. The temporal response of the brain after eating revealed by functional MRI. Nature. 2000;405:1058–1062.
- Smeets PA, de Graaf C, Stafleu A, van Osch MJ, van der Grond J. Functional MRI of human hypothalamic responses following glucose ingestion. Neuroimage. 2005;24:363–368.
- Page KA, Seo D, Belfort-DeAguiar R, et al. Circulating glucose levels modulate neural control of desire for high-calorie foods in humans. J Clin Invest. 2011;121:4161–4169.
- Tataranni PA, Gautier JF, Chen K, et al. Neuroanatomical correlates of hunger and satiation in humans using positron emission tomography. Proc Natl Acad Sci U S A. 1999; 96: 4569–4574.
- Small DM, Zatorre RJ, Dagher A, Evans AC, Jones-Gotman M. Changes in brain activity related to eating chocolate: from pleasure to aversion. Brain. 2001;124:1720–1733.
- Volkow ND, Wang GJ, Baler RD. Reward, dopamine and the control of food intake: implications for obesity. Trends Cogn Sci. 2011; 15:37–46.
- Centers for Disease Control and Prevention. Adult Obesity Facts. Available at: cdc.gov/obesity/ data/adult.html. Accessed May 21, 2015.
- American Heart Association. Added Sugars. Available at: heart.org/HEARTORG/Getting Healthy/ Nutrition Center/ HealthyDietGoals/ Added-Sugars_ UCM_ 305858_ Article.jsp. Accessed May 21, 2015.
- Yang Q, Zhang Z, Gregg EW, Flanders WD, Merritt R, Hu FB. Added sugar intake and cardiovascular diseases mortality among US adults. JAMA Intern Med. 2014;174:516–524.
- American Beverage Association. Beverage Industry Responds to Study on Added Sugar Intake and Cardiovascular Diseases Mortality. Available at: ameribev.org/news-media/news-releasesstatements/ more/325. Accessed May 22, 2015.
- American Diabetes Association. Overall Numbers, Diabetes and Prediabetes. National Diabetes Statistics Report, 2014. Available at: diabetes.org/diabetes-basics/statistics. Accessed May 22, 2015.
- Danaei G, Finucane MM, Lu Y, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 countryyears and 2.7 million participants. Lancet. 2011;378:31–40.
- Burt BA, Pai S. Sugar consumption and caries risk: a systematic review. J Dent Educ. 2001;65: 1017–1023.
- Freeman R. Moderate evidence support a relationship between sugar intake and dental caries. Evid Based Dent. 2014:15:98–99.
- Dragana A, Pham TTV. Global transcriptional analysis of Streptococcus mutans sugar transporters using microarrays. J Bacteriol. 2007;189: 5049–5059.
- Decker E-M, Klein C, Schwindt D, von Ohle C. Metabolic activity of Streptococcus mutans biofilms and gene expression during exposure to xylitol and sucrose. Int J Oral Sci. 2014; 6: 195–204.
- Ma R, Sun M, Wang S, et al. Effect of high-fructose corn syrup on the acidogenicity, adherence and biofilm formation of Streptococcus mutans. Aust Dent J. 2013;58:213–218.
From Dimensions of Dental Hygiene. June 2015;13(6):60–64.
