 PEOPLEIMAGES / ISTOCK / GETTY IMAGES PLUS
PEOPLEIMAGES / ISTOCK / GETTY IMAGES PLUS
Addressing Suicide Risk in the Dental Setting
Incorporating screening questionnaires that assess probability for suicide ideation, capability, and attempt into the medical history form may help ensure at-risk patients receive the help they need.
This course was published in the April 2022 issue and expires April 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the differences between suicidal ideation, suicide attempt, and suicide.
- Explain the demographic information regarding those at risk for suicide.
- Note the risk and protective factors for suicide.
- Discuss the role healthcare providers play in addressing suicide risk.
Death by suicide is a serious public health problem that affects millions of people worldwide. Each year, approximately 700,000 people die of suicide.1–3 In 2019, it was the fourth leading cause of death among those ages 15 to 29 globally, with 77% of suicide deaths occurring in low- and middle-income countries.1–3 In 2018 to 2019, suicide was the tenth leading cause of death in the United States and the second leading cause of death among young adults.4–6 Death by suicide is not only devastating to the family involved, but it reverberates throughout the community and social circles.1,4,6 Healthcare providers can be gatekeepers for the detection of patients at risk for suicide. More specifically, oral heath professionals are on the frontlines of preventive healthcare, with many patients seeking treatment biannually. This gives dental hygienists the opportunity to identify and address early warning signs of depression, self-harm, suicide ideation, and attempt.
Categories Associated With Suicide
Suicide ideation is the consideration of suicide along with the capability of suicide, but the individual has difficulty overcoming strong and natural fears of pain, injury, and death. Suicide attempt is defined as an unsuccessful effort to end one’s life. Successful suicide occurs when an individual inflicts methods of self-harm that ultimately result in death.3–5 Suicide capability is the level of access to lethal means of executing death by suicide such as firearms, controlled substances, carbon monoxide poison, sharp objects for cutting, and/or ligatures for hanging.5,7–9 The use of firearms is the most common means (51%) of suicide in the US, and the majority of deaths caused by firearms each year in the US are related to suicide.7–9
Demographic Information
Globally, suicide was the fourth leading cause of death among individuals between the ages of 15 and 19 in 2019, and, in the US, it was the second leading cause of death among those between the ages of 10 and 24. In the US, suicide rates have increased 57.7% between 2007 and 2018.1,4,10,11
Individuals who identify as lesbian, gay, bisexual, transgender, queer, intersex, asexual, and other sexual orientations not included in the acronym, LGBTQIA+, have significantly higher rates of depression, suicide ideation, and suicide attempts due to discrimination, stigma, loss of social supports, and /or internalized heterosexualism.12–14
Suicide is a leading cause of death among ethnic minorities (Asians, African Americans, American Indians, and Hispanics) in the United States.4,15–17 Discrimination is a chronic stressor for people of color, which may lead to mental health problems and high blood pressure.15–17
The suicide rate for US military veterans is 1.5 times higher than the general population.4,18–20 In 2019, firearms were used in approximately 70% of all male veteran suicides and about 50% of all female veteran suicides.18,20 Military veterans are at high risk for suicide due to substance abuse, acute psychosocial stressors, insomnia, and other mental health conditions, with post-traumatic stress disorder (PTSD) doubling the risk of suicidal attempt or ideation.19,21,22
Impact of COVID-19
The COVID-19 pandemic brought significant challenges to mental health, and suicide ideation is thought to have increased over the past 2 years. The intersections of extreme social distancing, geographic isolation, rising unemployment, and disruption in routine contributed to financial strain, work-related stress, childcare challenges, and interpersonal struggles.23–25 In the US, mental health-related emergency department visits for adolescents ages 12 to 17 years saw a 31% increase in 2020 as compared to 2019.25,26
Communities of color—specifically American Indian and Alaska Native women and men, Black/African-American women, and Hispanic women— experienced significantly increased risk of suicide—139%, 71%, 65%, and 37%, respectively— due to failure to receive adequate healthcare, job/business loss, and other economic consequences.9,23,26 For racial and ethnic groups, the amalgamation of the aforementioned consequences and trying to survive amid the pandemic may result in an exacerbated risk of suicide ideation and attempt.
Risk and Protective Factors
Most individuals who are depressed, attempt suicide, or have other risk factors do not necessarily die by suicide.4,5,27 However, related risk factors include previous suicidal behavior; psychosocial trauma; family history of suicidal behavior; mental health diagnoses; misuse and abuse of alcohol or other drugs; exposure to violence (eg, child abuse and neglect, sexual violence, and intimate partner violence); recent loss of a loved one or job; hopelessness; severe insomnia; social isolation; chronic disease/pain; and access to lethal means.4,5,11,19,22,27–29
Protective factors encompass social connectedness (interpersonal or institutional); effective life coping and problem-solving skills; availability of quality and ongoing physical and mental healthcare; cultural, religious, or moral beliefs that prohibit suicide; and limited access to lethal means.4,22,27–30
Suicide prevention requires a multidisciplinary approach.4,25,27,29,30 Hospitals, schools, tribes, and branches of the military have expanded suicide prevention and screening efforts in an attempt to reduce suicide nationally and globally.
Prevention Strategies
State and national programs are available to support suicide prevention. States, such as Tennessee, Massachusetts, and Texas, have made independent investments in suicide prevention by forging strong relationships with local healthcare systems and implementing the national Zero Suicide model.8,9 In 2001, the Henry Ford Health System in Michigan improved its suicide prevention screening process, resulting in an 80% reduction in suicide rates between 2009 and 2010.26,27,30,31 Parkland Hospital in Dallas implemented universal suicide risk screening in 2015.26,32 The University of Pennsylvania evaluates all patients in its emergency department and outpatient setting on probability for suicide ideation, capability, and attempt.26,33 The Billings Clinic serving Montana, Wyoming, and the western Dakotas screens all patients in its emergency department.26,34
School programs—such as the Universal Sources of Strength, Maine Youth Suicide Prevention Program, PROSPER project, University of Washington’s Communities That Care, 2004 Garrett Lee Smith Memorial Act, and the worldwide program Youth Aware of Mental Health—emphasize suicide screening, prevention, and training in the educational setting.4,8,9,27,30,35–39
For American Indian/Alaska Native populations, programs—such as the Native American Rehabilitative Association of the Northwest, 1991 Johns Hopkins Center for American Indian Health, 2001 White Mountain Apache Tribe Celebrating Life Prevention Team, and 2017 US Centers for Disease Control and Prevention Preventing Suicide: a Technical Package of Policy, Programs, and Practices—promote comprehensive suicide prevention efforts through decreasing harm and reducing risk.4,8,9,30,40
The 1996 US Air Force Suicide Prevention Program, 2007 Joshua Omvig Veterans Suicide Prevention Act, 2009 Army Service Suicide Prevention Program, 2012 Navy and Marine Corps Suicide Prevention Program, 2019 PREVENTS Program, 2019 Hannon Act, and 2020 the Veterans Combat Act were established to address suicide prevention efforts across multiple levels of the military.9,20,27,41
Role of Oral Health Professionals
Oral health professionals may lack specific training to handle patients at risk for suicide. With additional education, dental providers can conduct routine screenings in a variety of settings to identify individuals at risk, create safeguards to protect patients from self-harm, and refer for follow-up care.42–44 Dental hygienists are well positioned to screen for suicidal tendencies as they often treat patients twice annually. Biannual review of medical histories that incorporate suicide risk questionnaires may help prevent suicide ideation, capability, and attempt.
Table 1 provides a list of tools clinicians may use to assess patients for suicide risk: the Patient Health Questionnaire (PQH-9), Ask Suicide Screening Questions (ASQ), and Columbia-Suicide Severity Rating Scale (C-SSRS).22,28,43,45 These questionnaires are evidence-based, effective, and easily administered in the clinical setting. The PQH-9 is a brief assessment tool, incorporating nine questions that measure depression severity. The ASQ is a standardized screening tool for suicide risk using four yes/no questions that be administered in as little as 20 seconds. The C-SSRS assesses suicidal ideation and suicidal behavior via six yes/no questions.22,28,43,45 Training is recommended for the administration of the C-SSRS and can be found online free-of-charge.
Suicide risk screening should also include direct interventions that address suicidal thoughts and behaviors. Table 2 illustrates screening inquiries that dental professionals can deploy while engaging with patients in the dental setting. Incorporating such questions on the health history form can help identify the warning signs of suicidal thoughts. Actively listening, asking follow-up questions, and, when necessary, referring to medical or mental health professionals are key components for the succesful management of patients at risk for suicide. 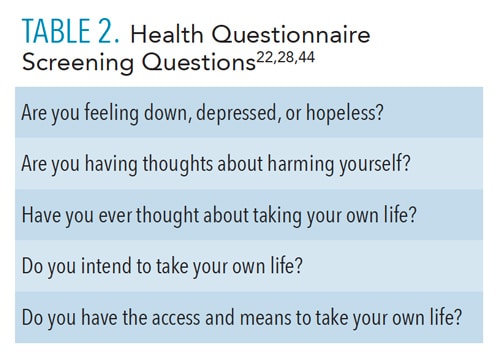
Conclusion
Several different levels of suicidal tendencies exist, ranging from self-harm, to ideation, to attempt, to ending one’s life. Suicide is a serious public health issue that has no single determining cause, but occurs in response to the intersections of multiple biological, psychological, interpersonal, environmental, and societal influences over time. Suicide ideation, risk, and attempt can be prevented by encompassing a comprehensive multidisciplinary approach on individual, relationship, societal, and community levels.
Asking suicide screening questions is an effective intervention step because it may be the first encounter in which a patient verbalizes his or her troubling thoughts about suicide ideation. The entire healthcare team bears responsibility to increase gatekeeper training, improve knowledge of the warning signs for suicide ideation and attempt, and understand when and how to connect individuals in crisis to medical assistance and follow-up care. As dental hygiene providers on the frontlines of preventive healthcare, we need to incorporate inquiries and/or screening questionnaires on the medical history form assessing patients’ probability for suicide ideation, capability, and attempt. Those who are having thoughts of suicide ideation should be encouraged to call 800-273-8255, or text HOME to 741741 from anywhere in the US.
References
- World Health Organization. Suicide Prevention fact Sheet. Available at: who.int/news-room/fact-sheets/detail/suicide. Accessed March 25, 2022.
- Cohen LJ, Gorman B, Briggs J, Jeon ME, Ginsburg T, Galynker I. The suicidal narrative and its relationship to the suicide crisis syndrome and suicidal behavior. Suicide Life Threat Behav. 2019;49:413–422.
- Muñoz-Sánchez JL, Sánchez-Gómez MC, Martín-Cilleros MV, Parra-Vidales E, De Leo D, Franco-Martín MA. Addressing suicide risk according to different healthcare professionals in Spain: a qualitative study. Int J Environ Res Public Health. 2018;15:2117.
- Miller BF, Coffey MJ. Understanding suicide risk and prevention. Available at: healthaffairs.org/do/葖.1377/hpb20201228.198475/full. Accessed March 25, 2022.
- Shahnaz A, Bauer BW, Daruwala SE, Klonsky D. Exploring the scope and structure of suicide capability. Suicide Life Threat Behav. 2020;50:1230–1240.
- Rural Health Information Hub. Overview of Suicide in the US. Available at: ruralhealthinfo.org. Accessed March 25, 2022.
- Rural Health Information Hub. Risk Factors for Suicide. Available at: ruralhealthinfo.org/toolkits/suicide/䁯/risk-factors. Accessed March 25, 2022.
- Substance Abuse and Mental Health Services Administration. National Strategy for Suicide Prevention Implementation Assessment Report. Available at: store.samhsa.gov/product/National-Strategy-for-Suicide-Prevention-Implementation-Assessment-Report/sma17-5051 Accessed March 25, 2022.
- United States Department of Health and Human Services. The Surgeon General’s Call to Action on Suicide Prevention. Available at: hhs.gov/sites/default/files/sprc-call-to-action.pdf. Accessed March 25, 2022.
- Kim J, Pike K, McCauley E, Stoep AV. Ethnic variations of trajectories in suicide ideation and attempt: From middle school to high school. Suicide Life Threat Behav. 2019;49:432–443.
- Horowitz L, Tipton MV, Pao M. Primary and secondary prevention of youth suicide. Pediatrics. 2020;145:195–203.
- Horwitz AG, Berona J, Busby DR, et al. Variation in suicide risk among subgroups of sexual and gender minority college students. Suicide Life Threat Behav. 2020;50:1041–1053.
- Romanelli M, Xiao Y, Lindsey MA. Sexual identity—behavior profiles and suicide outcomes among heterosexual, lesbian, and gay sexually active adolescents. Suicide Life Threat Behav. 2020;50:921–933.
- Salentine CM, Hilt LM, Muehlenkamp JJ, Ehlinger BA. The link between discrimination and worst point suicidal ideation among sexual and gender minority adults. Suicide Life Threat Behav. 2020;50:1621–1629.
- Coleman KJ, Johnson E, Ahmedani BK, et al. Predicting suicide attempts for racial and ethnic groups of patients during routine clinical care. Suicide Life Threat Behav. 2020;49:724–734.
- Brooks JR, Hong JH, Cheref S, Walker RL. Capability for suicide: Discrimination as a painful and provocative event. Suicide Life Threat Behav. 2020;50:1173–1180.
- Cheref S, Talavera D, Walker RL. Perceived discrimination and suicide ideation: Moderating roles of anxiety symptoms and ethnic identity among Asian American, African American, and Hispanic emerging adults. Suicide Life Threat Behav. 2019;49:665–677.
- American Foundation for Suicide Prevention. Military and Veteran Suicide Prevention. Available at: afsp.org/military-and-veteran-suicide-prevention. Accessed March 25, 2022.
- Hooper CR. Suicide among veterans. Available at: americanaddictioncenters.org/veterans/suicide-among-veterans. Accessed March 25, 2022.
- Office of Mental Health and Suicide Prevention United States Department of Veteran Affairs. National Veteran Suicide Prevention Annual Report. Available at: mentalhealth.va.gov/docs/data-sheets/떕/떕-National-Veteran-Suicide-Prevention-Annual-Report-FINAL-9-8-21.pdf. Accessed March 25, 2022.
- Batterham PJ, Calear AL, Christensen H, Carragher N, Sunderland. Independent effects of mental disorders on suicidal behavior in the community. Suicide Life Threat Behav. 2018;48:512–521.
- Abuse and Mental Health Services Administration. Addressing Suicidal Thoughts and Behaviors in Substance Abuse Treatment. Available at: store.samhsa.gov/sites/default/files/d7/priv/sma13-4793.pdf. Accessed March 25, 2022.
- Fitzpatrick KM, Harris C, Drawve G. How bad is it? Suicidality in the middle of the COVID-19 pandemic. Suicide Life Threat Behav. 2020;50:1241–1249.
- Pruitt LD, McIntosh L. Suicide safety planning during a pandemic: The implications of COVID-19 on coping with a crisis. Suicide Life Threat Behav. 2020;50:741–749.
- Yard E, Radhakrishnan L, Ballesteros MF, et al. Emergency department visits for suspected suicide attempts among persons aged 12-25 years before and during the COVID-19 pandemic—United States, January 2019–May 2021. MMWR Morb Mortal Wkly Rep. 2021;70:888–894.
- Angelone, KM. Suicide risk screenings can save lives. Available at: pewtrusts.org/en/research-and-analysis/articles/떖/葍/葥/suicide-risk-screenings-can-save-lives?utm_campaign=2022-01-26+Suicide+Risk+Reduction+launch&utm_medium=email&utm_source=Pew&subscriberkey=00Q0P00000jkaPgUAI. Accessed March 25, 2022.
- Stone D, Holland K, Bartholow B, Crosby A, Davis S, Wilkins N. Preventing suicide: a technical package of policy, programs, and practices. Available at: cdc.gov/suicide/pdf/suicideTechnicalPackage.pdf. Accessed March 25, 2022.
- American Psychiatric Association. Suicide and serious mental illness: An overview of considerations, assessment, and safety planning. Available at: smiadviser.org/wp-content/uploads/떔/葘/SMI-Adviser-Suicide-and-Serious-Mental-Illness.pdf. Accessed March 25, 2022.
- Rural Health Information Hub. Protective Factors for Suicide. Available at: ruralhealthinfo.org/toolkits/suicide/䁯/protective-factors. Accessed March 25, 2022.
- National Center for Injury Prevention and Control, Division of Violence Prevention. Suicide Prevention: A Public Health Issue. Available at: stacks.cdc.gov/view/cdc/. Accessed March 25, 2022.
- Henry Ford Health System. Suicide Prevention Guidelines for Health Care Providers. Available at: henryford.com/services/behavioral-health/zero-suicide. Accessed March 25, 2022.
- Parkland Hospital. Parkland Mental Health Providers Shine Spotlight on Rising Rates of Suicide. Available at: parklandhospital.com/phhs/news-and-updates/parkland-mental-health-providers-shine-spotlight-o-1624. Accessed March 25, 2022.
- University of Pennsylvania. Penn Center for the Prevention of Suicide. Available at: med.upenn.edu/suicide. Accessed March 25, 2022.
- Billings Clinic. Psychiatric Services. Available at: billingsclinic.com/services-specialties/psychiatric-services. Accessed March 25, 2022.
- Sources of Strength. Universal Suicide Prevention. Available at: sourcesofstrength.org/#:~:text=The%20mission%20of%20Sources%20of,approach%20for%20youth%20suicide%20prevention. Accessed March 25, 2022.
- Maine Department of Health and Human Services. The Maine Suicide Prevention Program. Available at: maine.gov/suicide. Accessed March 25, 2022.
- Prosper ISD. Mental Health/Suicide Prevention and Awareness. Available at: prosper-isd.net/Page/찰. Accessed March 25, 2022.
- University of Washington. The Center for Communities That Care. Available at: communitiesthatcare.net. Accessed March 25, 2022.
- Mental Health in Mind International AB. Youth Aware of Mental Health. Available at: y-a-m.org. Accessed March 25, 2022.
- Kennedy K, Carmichael A, Brown MM, Trudeau A, Martinez P, Stone DM. The state of state, territorial, and tribal suicide prevention: Findings from a web-based survey. Available at: cdc.gov/suicide/pdf/State-of-the-States-Report-Final-508.pdf. Accessed March 25, 2022.
- National Action Alliance for Suicide Prevention and the Substance Abuse Mental Health Services Administration. National Strategy for Suicide Prevention Implementation Assessment Report Addendum: Federal Crosswalk. Available at: theactionalliance.org/sites/default/files/addendum_nssp_implementation_assessment_report_federal_crosswalk.pdf. Accessed March 25, 2022.
- National Action Alliance for Suicide Prevention: Clinical Workforce Preparedness Task Force. Suicide Prevention and the Clinical Workforce: Guidelines for Training. Available at: theactionalliance.org/sites/default/files/guidelines.pdf. Accessed March 25, 2022.
- Rural Health Information Hub. Screening for and Addressing Suicide Risk in Clinical Settings. Available at: ruralhealthinfo.org/toolkits/suicide/䁰/screening-tools Accessed March 25, 2022.
- Mokkenstorm JK, Kerkhof JFM, Smit, JH, Beekman ATF. Is it rational to pursue zero suicides among patients in health care? Suicide Life Threat Behav. 2018;48:745–754.
- The Columbia Lighthouse Project. The Columbia Protocol (C-SSRS). Available at: cssrs.columbia.edu/the-columbia-scale-c-ssrs/about-the-scale. Accessed March 25, 2022.
From Dimensions of Dental Hygiene. April 2022;20(4):34-37.
