
Adapt to Deep Pockets
Follow these strategies to therapeutically debride root surfaces within periodontal pockets.
The challenge of both manual and power instrumentation is to access and effectively instrument all areas of the tooth/root surface. By providing a bird’s-eye view of the pocket post-scaling, the dental endoscope has confirmed that all bacterial biofilm and bacteria-retentive calculus must be entirely removed before inflammation will resolve completely. If left behind, even small areas of residual calculus will lead to areas of inflammation on the adjacent epithelial lining.
POWER OF THE PROBE
The primary and most effective instrument for identifying, accessing, and measuring the deepest and most challenging periodontal pockets is a periodontal probe. This straight, thin instrument can be maneuvered into the most difficult-to-reach pockets. The exception is an interproximal furcation when a curved Nabers probe is better for reaching into class II or greater furcations. A curved or contra-angled ultrasonic insert/tip (UIT) is also more effective in reaching into these furcations than a straight tip. The terminal portion of most UITs is thin and straight and mimics the shape of a periodontal probe. The lateral surface of the terminal few millimeters of the UIT is the only part that should be used for treatment. This part of the tip has the most movement, making it the most effective. The point, which also has maximum movement, should not be used on the root because it can cause serious damage. The point is sometimes recommended for use on heavy, tenacious calculus deposits, but only when direct contact with the root can be avoided.

THE RIGHT POSITION
With a magnetostrictive insert, all 360° of the tip are active and available for use in treatment. With a piezoelectric tip, only the lateral sides of the tip are effective because the instrument moves linearly. This requires more rotation of the instrument to keep the effective surface of the tip well adapted to the tooth. This is essentially the same rotation needed to adapt the lateral surfaces of a universal curet without the issue of blade angulation. For good adaptation, there will be a 90° rotation between treatment of the mid-facial or mid-lingual and the proximal surface.


PARAMETERS OF THE POCKET
Based on sales figures, the most popular UITs are the straight shank configuration. With that in mind, the illustrations and discussion of instrument adaption that follow use straight shanked, sometimes incorrectly called “universal” UITs. However, the best technique is to use the straight shank configuration in anterior areas and contra-angled UITs in posterior areas. A future article will address the use of contra-angled UITs.
In order to therapeutically debride in a periodontal pocket, every part of the root surface needs to be contacted by the tip of the UIT. The effective stroke width of the tip is very narrow. The idea that a few sweeps of the insert through a pocket will debride the surface is not realistic. Ultimately, good instrumentation requires an in-depth understanding of the parameters of the pocket and root anatomy, in addition to effective adaptation of the instrument. Fortunately, with ultrasonic instrumentation, there are no concerns about blade angulation and no need to create and manage lateral pressure. To adapt to the root surface in a periodontal pocket, the UIT is almost always positioned parallel to the long axis of the tooth in the same way that a periodontal probe would be positioned. Just as a probe is tilted to reach under the contact area, the UIT is tilted to reach under the contact but without letting the back of the instrument press against the gingiva at the line angle.


VISUAL GUIDE
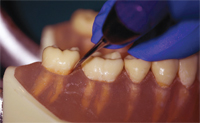
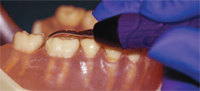
Figure 1 through Figure 3B show instrument adaptation on the mesial line angle of tooth #31. Figure 1 shows normal positioning of a periodontal probe on the line angle with a reading of about 6 mm. Figure 2 shows positioning of a straight magnetostrictive insert that mirrors the position of the probe. This position allows access to the full depth of the pocket without distending the gingival tissue. Figure 3A shows positioning of the same insert but with the point angled toward the interproximal area.


This is a common technique that feels much like the familiar approach used with curets. This technique works when the pockets are shallow but not when they are deep. Visually, the instrument may look like it is positioned well for treatment of the line angle as the visible portion of the UIT is pointing toward that area. However, if only the terminal 1 mm to 2 mm of the tip is effective for treatment, this part of the insert is positioned too close to the interproximal area for effective treatment of the pocket at the line angle. In Figure 3B (page 56), the UIT is at the same angle and distance facial-lingually as in Figure 3A, but it has been lifted out of the pocket to show that the position of the UIT’s tip is incorrect. If an instrument with this adaptation was forced downward and/or facially to reposition the tip to the line angle area, the back of the UIT would be pressed against the soft tissue, which can cause damage.
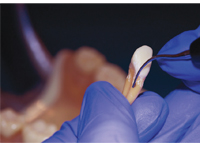
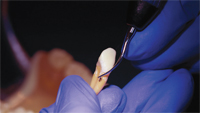
Figure 4A and 4B show good adaptation to the mesial line angle from a more occlusal view. A magnetostrictive insert is shown in Figure 4A. Any surface of the tip may be used with this instrument. A piezoelectric tip is shown in Figure 4B. The placement of the tip—at a right angle to the surface being treated—is necessary with piezoelectric instruments because only the lateral surfaces are effective for debridement. This can make good adaptation with a straight tip challenging on the proximal surfaces of molars, especially in a small mouth. A contra-angled tip may be more effective in adapting the lateral surfaces of a piezoelectric tip to the proximals of molars.
Figure 5 demonstrates instrumentation of the true interproximal area of the molars. Figure 5A shows good adaptation of a probe, Figure 5B illustrates a magnetostrictive insert, and Figure 5C demonstrates with a piezoelectric tip. Note the upright position of the working end of all three instruments with a slight tilt to reach under the contact area. This adaptation is the most effective for reaching the deepest part of the pocket in the col area.


Figure 6 through Figure 9 relate to adaptation of UITs for calculus removal in a pocket on the distal facial aspect of tooth #27. This same information applies to the true interproximal surface as well. The black dot represents a calculus spicule. In Figure 6, tooth #27 is shown without gingiva to demonstrate that an upright, probe-like position with a slight curve of the UIT toward the proximal will most easily reach the deposit (Figure 6A). Figure 6B shows the UIT positioned with the toe angled slightly toward the interproximal area. It is unlikely that the deposit at the line angle will be effectively instrumented with this technique. As shown in the figure, the tip misses the deposit because it enters the area too far toward the proximal surface.


An effort to upright the UIT in order to swing the toe toward the buccal area is not possible because of the close proximity of the maxillary arch. An effort to move the entire UIT toward the facial surface will cause pressure against the gingiva. With this technique, a bruise of the papilla or, in extreme cases, a linear laceration of the gingiva at the line angle can result. These positions are duplicated with the gingiva in place in Figure 7. Good adaptation is shown in Figure 7A and poor adaptation is in Figure 7B. Notice the potential to press the back of the UIT against the gingiva while trying to adapt to the deep line angle in Figure 7B. Figure 8 and Figure 9 replicate the same adaptation situation as Figure 6 and Figure 7 with a piezoelectric insert.

CONCLUSION
The goal of nonsurgical periodontal therapy is to arrest or reverse the progression of periodontal disease. In order to accomplish this goal, root instrumentation performed by either ultrasonic or hand instruments must be meticulously and effectively completed. A good understanding of root and pocket topography along with thoughtful adaptation of the terminal millimeters of the UIT are necessary for positive treatment outcomes. Mimicking the position used with the periodontal probe to identify the location and extent of the pockets is an excellent starting point for achieving a successful outcome in ultrasonic instrumentation of periodontal pockets.
From Dimensions of Dental Hygiene. October 2012; 10(10): 54,56,58-59 .

{kind=link}