Building On The Dental Hygiene Base
Expanded function models can ease the access-to-care problems faced throughout the United States.
The American Dental Hygienists’ Association (ADHA) is leading the transformation of the dental hygiene profession to improve the public’s oral and overall health. The organization believes that better utilization of the existing oral health care workforce will open the doors to professional dental care for many. Registered dental hygienists—practicing to the fullest extent of their education and preparation—can provide opportunities for countless Americans who otherwise would not have access to oral health care.
A 2014 report from the National Governors Association discussed expanding the provision of affordable preventive services outside of the private dental practice, noting that many states are looking into altering supervision or reimbursement rules, as well as creating professional certifications for advanced-practice dental hygienists.1 Currently, 37 states allow dental hygienists to initiate patient care in settings outside of the private dental office without the presence of a dentist. These policies enable dental hygienists to provide care in community settings and reach a variety of patient populations.
![]() MID-LEVEL PROVIDERS
MID-LEVEL PROVIDERS
 MID-LEVEL PROVIDERS
MID-LEVEL PROVIDERSThe mid-level oral health practitioner is one example of an expanded function model, which the ADHA defines as a licensed dental hygienist who has graduated from an accredited dental hygiene program and who provides primary oral health care directly to patients to promote and restore oral health through assessment, diagnosis, treatment, evaluation, and referral services. The mid-level oral health practitioner has met the educational requirements to provide services within an expanded scope of care and practices under regulations set forth by the appropriate licensing agency. The ADHA is committed to supporting new dental hygiene-based models for oral health care delivery. Dental hygienists are an available, educated, and prepared asset to the workforce. The educational infrastructure is in place, with 335 dental hygiene programs currently educating students across the country. Dental hygienists today work in a variety of settings, and the public will benefit from practitioners who can provide both preventive and restorative services.
There is not a single definition for mid-level dental providers because each state using these practitioners has created its own variation based on the needs of its citizens, composition of the workforce, and demographics. While there are many different types of mid-level providers, the ADHA specifically supports workforce models that culminate in graduation from an accredited institution, professional licensure, and the ability to provide direct-access patient care. Direct access enables dental hygienists to initiate treatment based on their assessment of a patient’s needs without the specific authorization of a dentist, to treat the patient without the presence of a dentist, and to maintain a provider-patient relationship.
MINNESOTA AND MAINE
In 2009, Minnesota passed legislation that created the dental therapist (DT) and the advanced dental therapist (ADT). Some ADTs in Minnesota are dually licensed as registered dental hygienists and ADTs, as Normandale Community College/Metropolitan State University require students to be licensed dental hygienists as a prerequisite of the program. Today, nearly 5 years after passing the legislation, 42 DTs and six ADTs are practicing in Minnesota. ADT services are provided under general supervision, pursuant to a written collaborative agreement with a Minnesota licensed dentist. DTs, however, must work under the direct supervision of a licensed dentist.
In 2014, Maine passed legislation creating the dental hygiene therapist (DHT). DHTs in Maine will be dually licensed as registered dental hygienists and DHTs, as the Maine statute requires that applicants to the program must possess a license in dental hygiene. DHTs must work under direct supervision of a Maine licensed dentist, with a written practice agreement. The Minnesota Department of Health and the Minnesota Board of Dentistry released the report “Early Impacts of Dental Therapists in Minnesota: Report to the Minnesota Legislature 2014” in February 2014.2 This report was a directive from the 2009 Minnesota legislation that created the United States’ first state-authorized mid-level oral health practitioner. Key conclusions in the report indicate that the dental therapy workforce is growing and appears to be serving predominantly low-income, uninsured, and underserved patients. Furthermore, DTs are practicing safely, and clinics report improved quality and high patient satisfaction with DT services.
CHALLENGES AHEAD
On the other end of the spectrum, Alabama, Georgia, Mississippi, and Wyoming have some of the most restrictive state laws when it comes to practicing dental hygiene. These regulations impede the ability of dental hygienists to practice at the fullest extent of their scope of practice, and underutilize their education and experience. For example, these states require that a child must be seen by a dentist prior to receiving dental sealants—an unwarranted restriction that has no evidence to substantiate its need. By placing such limits on supervision and the setting in which they practice, the ability of dental hygienists to access underserved populations and deliver essential care are drastically reduced.
UNITING DENTAL HYGIENE VOICES
The ADHA is committed to working collaboratively with oral health partners and other health advocates to improve access to dental services throughout the country, and to ensure the public is receiving the best possible care. Several states will introduce legislation in 2015 to authorize new oral health work force models and to expand opportunities for the highly educated and experienced dental hygiene workforce.
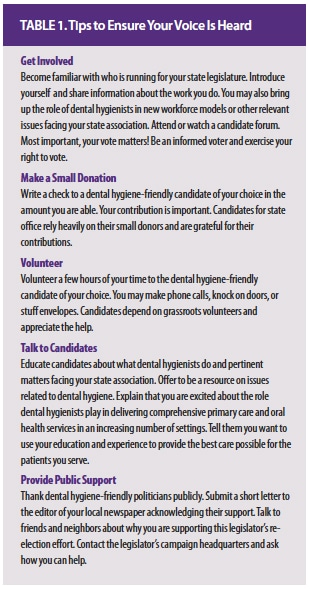
All dental hygienists are needed to join ADHA in moving the profession of dental hygiene forward. With the November election cycle fast approaching, there is no better time to become involved. Table 1 provides helpful tips for dental hygienists who are not yet active in this important work. Dental hygienists have much to offer in improving the oral health and quality of life for many Americans. The ADHA needs the support of all clinicians to ensure that dental hygienists have the opportunity to make a difference in this arena.
REFERENCES
- National Governors Association. The Role of Dental Hygienists in Providing Access to Oral Health Care. Available at: nga.org/cms/home/nga-center-for-best-practices/center-publications/page-health-publications/col2-content/main-content-list/the-role-of-dental-hygienists-in.html. Accessed September 24, 2014.
- Minnesota Department of Health, Minnesota Board of Dentistry. Early Impacts of Dental Therapists in Minnesota. Available at: health.state.mn.us/divs/orhpc/workforce/dt/dtlegisrpt.pdf. Accessed September 24, 2014.
From Perspectives on Dental Hygiene, a supplement to Dimensions of Dental Hygiene. November 2014;12(11):14–16.
