 STOCKVISUAL/ISTOCK/GETTY IMAGES PLUS
STOCKVISUAL/ISTOCK/GETTY IMAGES PLUS
Understanding the New Blood Pressure Guidelines
Oral health professionals who are well versed in the new guidelines will be best prepared to handle the implications on patient care.
This course was published in the May 2018 issue and expires May 30, 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Describe the categories in the new blood pressure guidelines.
- Explain the new lower threshold for high blood pressure.
- Discuss the impact of the new guidelines on health, in addition to management strategies and interventions.
Hypertension is a common health condition in the United States and a risk factor for heart disease and stroke.1 The US Centers for Disease Control and Prevention (CDC) 2016 statistics indicate that hypertension affects nearly one-third of US adults—approximately 75 million people.2 One out of every three adults has high blood pressure and only about half of individuals with hypertension have their condition under control.3,4 In 2014, high blood pressure was a primary or contributing cause of death for more than 410,000 Americans, or more than 1,100 deaths each day.1,5
The annual cost of health care services, medications, and missed days of work due to hypertension is estimated at $48.6 billion.5 Women and men are equally likely to develop high blood pressure during their lifetime.6 Black men develop high blood pressure more often than white and Hispanic men.3,6 Medical screening for chronic diseases conducted in the dental setting could save the health care system approximately $42 million to $102 million annually, as many patients visit their oral health professionals more often than their physicians.7
Numerous studies have shown blood pressure levels are positively related to the risk for stroke and coronary heart disease. According to Global Health Observatory data, raised blood pressure can lead to heart failure, peripheral vascular disease, renal impairment, retinal hemorrhage, and visual impairment.8 To allow for earlier intervention with lifestyle changes and nonpharmaceutical approaches, the American College of Cardiology and American Heart Association (ACC/AHA) released new guidelines to lower the definition of high blood pressure in 2017. The new ACC/AHA guidelines (Table 1) were developed with nine other professional organizations and were written by a panel of 21 scientists and health experts who reviewed more than 900 published studies.9
SCREENING IN THE DENTAL SETTING
The National Institutes of Health developed the National High Blood Pressure Education Program (NHBPEP) in 1972—which consists of a network of groups, including federal agencies, professional agencies, state health departments, and community-based programs—to provide education and screening opportunities for the early diagnosis of high blood pressure. The American Dental Hygienists’ Association and American Dental Association have supported blood pressure screening as an important aspect of patient care and have endorsed the NHBPEP’s mission and goals.10
Over the years, screening for various diseases has become more prevalent in the dental setting.11 Numerous studies have validated the significance of chairside medical screening in the dental setting and the willingness of oral health professionals to conduct it.12–17Patients are also open to medical screening in the dental setting.18,19 High blood pressure screening in dental settings is an effective way to detect unknown hypertension.20
Hypertension is asymptomatic and known as the “silent killer.” The only way to determine whether a patient has hypertension is to conduct a blood pressure screening. Blood pressure is measured in millimeters of mercury (mm Hg) using two numbers. The first number is called systolic blood pressure, which represents the pressure in the blood vessels when the heart beats while pumping blood. The second number is called diastolic blood pressure, which indicates the pressure in the blood vessels when the heart is at rest between beats. The gold standard for blood pressure measurement is the auscultatory method (sphygmomanometer and stethoscope), with digital arm and automated equipment as secondary modalities. Digital or electronic automatic blood pressure equipment is used in dental education institutions and commonly used in dental practices for convenience and low cost; however, clinical accuracy may be compromised. As such, if the reading is questionable, the blood pressure should be taken again using the auscultatory method or the patient should be referred to his or her primary care provider.21,22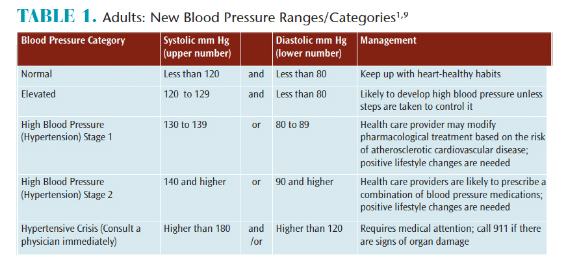
CHILDREN AND ADOLESCENTS
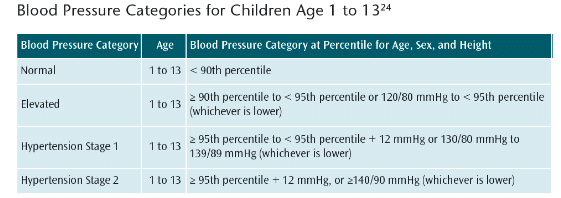
Before 1977, measuring the blood pressure of asymptomatic children or adolescents was uncommon in routine medical visits because there was no link between blood pressure levels in childhood and heightened risk for subsequent adverse cardiovascular events.23 In the mid-1970s, the NHBPEP convened a task force to examine blood pressure data on healthy children in order to determine the normal distribution and define the upper limits of blood pressure according to age.23 As data linking high blood pressure in childhood to an increased risk of cardiovascular events later in life were not available, the task force defined hypertension as the blood pressure level that exceeded the 95th percentile on age-related blood pressure distribution curves. This served as the first clinical practice guideline for childhood hypertension.23 The number of studies conducted on elevated blood pressure in children and adolescents has grown within the past 10 years, thus, the American Academy of Pediatrics released new pediatric hypertension clinical practice guidelines in 2017. Table 2 (page 47) provides guidelines for adolescents.23 The web version of this article includes a table on the children’s guidelines.
RECOMMENDATIONS AND DENTAL CARE
The new guidelines lower the definition of high blood pressure to 130/80 mm Hg for adults. This new definition broadens what defines disease, encompassing people who were previously considered healthy. Approximately 46% of US adults now have hypertension compared with about 32% under the former high blood pressure definition.24 Normal blood pressure is now considered below 120/80 mm Hg and elevated blood pressure is 120 mm Hg to 129 mm Hg systolic with a diastolic pressure below 80 mm Hg. Stage 1 hypertension is between 130 mm Hg and 139 mm Hg, or 89 mm Hg and 89 mm Hg (formerly known as “prehypertension”) and stage 2 hypertension is 140/90 mm Hg or higher (the old definition of high blood pressure). The new guidelines include recommendations for the way health professionals take blood pressure measurements, stressing the importance of using validated devices, allowing patients to rest for 5 minutes before taking their blood pressure, averaging at least two readings over two visits, and highlighting the value of appropriate training for health professionals to reveal “white-coat hypertension.”9,25 White-coat hypertension, also known as white coat syndrome, occurs when patients exhibit blood pressure levels above the normal range in a clinical setting due to anxiety.
Nonpharmacologic interventions to lower blood pressure are strongly supported in the new guidelines. The initiation of pharmacologic therapy for stage 1 hypertension is only if the patient has experienced a cardiovascular event (eg, heart attack, stroke) in the past or is at high risk of one based on age or the presence of a comorbidity (eg, diabetes, kidney disease, atherosclerosis). The recommendation to initiate pharmacologic therapy in patients without risk and at low risk for cardiovascular disease at blood pressure levels ≥ 140/90 mm Hg remains unchanged.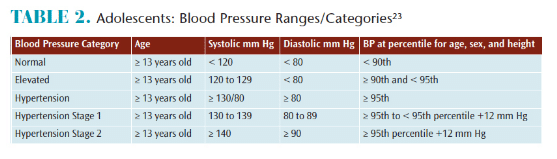
High blood pressure is second only to smoking as a preventable cause of heart attacks and strokes. Cardiovascular disease remains the leading cause of death among Americans.26 If Americans act on the new guidelines and lower their blood pressure by exercising and eating a healthier diet, they could decrease the death rate from heart attacks and stroke. A few concerns with the new guidelines are that a new disease designation can become a mandate for pharmacologic treatment without consideration of the patient’s risk level, and the guideline recommends daily sodium intake of less than 1,500 mg per day, which will be challenging for most people to achieve.26,27 The primary change in pharmacologic therapy is the elimination of beta-blockers from first-line therapy, with primary hypertension and no coexisting conditions that require beta-blocker therapy.26 An individualized approach to treating high blood pressure is recommended.
Oral health professionals need to become familiar with the new guidelines so they can educate patients about the impact on their overall health. Each blood pressure category has management recommendations and can be easily printed as an education/information handout. Patient education regarding both the adult and child/adolescent guidelines is important and oral health professionals should be prepared to provide referrals for further evaluation, if applicable. For patients whose blood pressure is deemed too high, medical clearance should be obtained before administering dental treatment to avoid an emergency situation.
![High Blood Pressure Resources]() PREVENTIVE MEASURES TO REDUCE RISK OF HYPERTENSION
PREVENTIVE MEASURES TO REDUCE RISK OF HYPERTENSION
 PREVENTIVE MEASURES TO REDUCE RISK OF HYPERTENSION
PREVENTIVE MEASURES TO REDUCE RISK OF HYPERTENSIONHigh blood pressure generally develops over many years, and it affects nearly everyone eventually. Fortunately, it can be easily detected and controlled. Other than predisposing factors, such as age, race, and family history, recommended preventive measures are relatively easy to follow. They are as follows:26–28
-
- Maintain a healthy weight. The heavier a patient is, the more blood is needed to supply oxygen and nutrients to tissues. As the volume of blood circulated through the blood vessels increases, so does the pressure on artery walls.
- Eat a heart-healthy diet. The DASH diet (Dietary Approaches to Stop Hypertension) is recommended by the US Department of Agriculture as an ideal eating plans for all Americans. It is rich in fruits, vegetables, whole grains, and low-fat dairy foods, and includes meat, fish, poultry, nuts, and beans. It limits sugar-sweetened foods and beverages, red meat, and added fats.
- Reduce sodium intake. Too much sodium in the diet can cause the body to retain fluid, which increases blood pressure. All Americans are recommended to keep sodium intake less than 2,300 mg. For people with high blood pressure, the recommendation is 1,500 mg or less per day.
- Supplement with potassium. Potassium helps balance the amount of sodium in the cells. If patients don’t have enough potassium in their diets or retain enough potassium, they may accumulate too much sodium in the blood. The adequate intake recommendation for potassium is 4,700 mg per day for adults.
- Increase physical activity. For substantial health benefits, adults should do at least 150 minutes a week of moderate-intensity, or 75 minutes a week of vigorous-intensity aerobic activity, or an equivalence combination of moderate- and vigorous-intensity aerobic activity. Children and adolescents should do 60 minutes or more of physical activity daily.
- Consume alcohol in moderation. Women should consume no more than one drink per day and men should consume no more than two drinks per day. One drink equals 12 oz of beer, 5 oz of wine, or 1.5 oz of 80-proof liquor.
- Reduce stress. High levels of stress can lead to a temporary increase in blood pressure.
- Quit tobacco use. Not only does smoking or chewing tobacco immediately raise blood pressure temporarily, but the chemicals in tobacco can damage the lining of the artery walls. This can cause the arteries to narrow, increasing blood pressure.
CONCLUSION
Oral health professionals play an important role in screening patients for hypertension. They also provide educational resources and recommendations and encourage patients to follow up with their primary health care providers. The new lower threshold is evidence-based with the intention to increase awareness, prevention, treatment and control of blood pressure. Table 3 provides additional resources for patients regarding blood pressure management. All health professionals should share this new information with patients to support early detection and early intervention.
REFERENCES
- United States Centers for Disease Control and Prevention. High Blood Pressure fact Sheet. Available at: cdc.gov/dhdsp/data_statistics/ fact_sheets/fs_bloodpressure.htm. Accessed April 9, 2018.
- Merai R, Siegel C, Rakotz M, et al. CDC Grand Rounds: a public health approach to detect and control hypertension. MMWR Morb Mortal Wkly Rep. 2016;65:1261–1264.
- Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the US: National health and nutrition examination survey, 2011-2012. NCHS Data Brief. 2013;133:1–8.
- Farley TA, Dalal MA, Mostashari F, Frieden TR. Deaths preventable in the US by improvements in the use of clinical preventative services. Am J Prev Med. 2010;38:600–609.
- US Centers for Disease Control and Prevention. Underlying cause of death 1999-2013 on CDC WONDER online database, released 2015. June 16, 2016. Available at: wonder.cdc.gov/ucd-icd10.html. Accessed April 9, 2018.
- National Heart, Lung, and Blood Institute. High Blood Pressure. Available at: nhlbi.nih.gov/health-topics/high-blood-pressure. Accessed April 9, 2018.
- Nasseh K, Greenberg B, Vujicic M, Glick M. The effect of chairside chronic disease screenings by oral health professionals on health care costs. Am J Public Health. 2014;104:744–750.
- World Health Organization. Global Health Observatory data. Available at: who.int/gho/ ncd/risk_factors/blood_pressure_prevalence_text/en. Accessed: April 7, 2018.
- American College of Cardiology. New ACC/AHA High Blood Pressure Guidelines Lower Definition of Hypertension. Available at: acc.org/latest-in-cardiology/articles/2017/11/08/11/47/mon-5pm-bp-guideline-aha-2017. Accessed April 9, 2018.
- Hughes C, Thompson AL, Browning WD. Blood pressure screening practices of a group of dental hygienists: A pilot study. J Dent Hyg. 2004;78:1–9.
- Wilkins EM, Wyche CJ, Boyd LD. The Clinical Practice of the Dental Hygienist. 12th ed. Philadelphia: Wolters Kluwer; 2017:13.
- Shimpi N, Schroeder D, Kilsdonk J, et al. Assessment of dental providers’ knowledge, behavior and attitude towards incorporating chairside screening for medical conditions: a pilot study. J Den Oral Care Med. 2016;2:1–7.
- Greenberg BL, Kantor ML, Bednarsh H. American dental hygienists’ attitudes towards chairside medical screening in a dental setting. Int J Dent Hygiene. 2017;15:e61–e68.
- Greenberg BL, Glick M, Frantsve-Hawley J, Kantor ML. Dentists’ attitudes towards chairside screening for medical conditions. J Am Dent Assoc. 2010;141:52–62.
- Santella AJ, Krishnamachari B, Davide SH, et al. Dental hygienists’ knowledge of HIV, attitudes towards people with HIV and willingness to conduct HIV testing. Int J Dent Hygiene. 2013;11:287–292.
- Santella AJ, Davide SH, Cortell M, et al. The role of dental hygienists in conducting rapid HIV testing. J Dent Hyg. 2012;86:265–271.
- Kalladka M, Greenberg BL, Padmashree SM, et al. Screening for coronary heart disease and diabetes risk in a dental setting. Int J Public Health. 2014;59:485–492.
- Creanor S, Millward BA, Demaine A, et al. Patients’ attitudes towards screening for diabetes and other medical conditions in the dental setting. Br Dent J. 2014;216:E2.
- Davide SH, Santella AJ, Furnari, W, et al. Patients’ willingness to participate in rapid HIV testing: A pilot study in three New York City dental hygiene clinic. J Dent Hyg. 2017;91:41–48.
- Engström S, Berne C, Gahnberg L, Svärdsudd K. Efficacy of screening for high blood pressure in dental health care. BMC Public Health. 2011;11:1–7.
- Furgeson D, Mickels-Foster N. Accuracy of digital arm and wrist manometers: Clinical implications for the dental hygienist. J Dent Hyg. 2013;87:309–314.
- Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA. 2003;289:2560–2572.
- Flynn JT, Falkner BE. New clinical practice guideline for the management of high blood pressure in children and adolescents. Hypertension. 2017;70:683–686.
- Bakris G, Sorrentino M. Redefining hypertension—assessing the new blood-pressure guidelines. N Engl J Med. 2018;378:497–499.
- Cobos B, Haskard-Zolnier K, Howard K. White coat hypertension: Improving the patient-health care practitioner relationship. Psychol Res Behav Manag. 2015;8:133–141.
- Cifu AS, Davis, AM. Prevention, detection, evaluation, and management of high blood pressure in adults. JAMA.2017;318:2132–2134.
- Miller ER, Jehn M. New high blood pressure guidelines create new at-risk classification. J Cardiovasc Nurs. 2004;19:367–371.
- Mayo Clinic. High Blood Pressure (Hypertension). Available at: mayoclinic.org/diseases-conditions/high-blood-pressure/symptoms-causes/syc-20373410. Accessed April 7, 2018.
- Flynn JT, Kaelber DC, Baker-Smith CM, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. 2017;140:1–71.
From Dimensions of Dental Hygiene. May 2018;16(5):46-49.

[…] oral health professionals should conduct blood pressure screenings and be well versed in the new blood pressure guidelines. Educating patients about oral health’s bearing on overall health should also be emphasized […]