The Truth About Gluten
Clinicians who are knowledgeable about gluten-mediated reactions will be prepared to treat patients with these types of allergies.
This course was published in the October 2015 issue and expires October 31, 2018. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define gluten and discuss its role in the development of allergic reactions, including celiac disease.
- Discuss strategies for managing gluten-mediated reactions.
- Identify the effects of celiac disease on oral health and the provision of dental treatment.
Today, grocery store shelves are full of gluten-free products—from bagels to frozen pizza. Even the Girl Scouts organization has joined the gluten-free movement with the introduction of the gluten-free cookie Toffee-Tastic in 2015. Gluten-free products are also big business—in 2014 annual sales reached $8.8 billion.1 So what is behind this gluten-free frenzy? Before this question can be answered, defining gluten and understanding what constitutes a gluten allergy is important. Gluten is a protein found in wheat, barley, rye, brewer’s yeast, and malt. It is the “glue” that holds breads, baked goods, and pastas together and provides the chewy texture associated with these foods.2 Wheat is often found in breads, baked goods, soups, pasta, cereals, sauces, salad dressings, and roux, while barley is contained in malt, food coloring, soups, malt vinegar, and beer. Specific types of breads, beers, and cereals contain rye.3 Granola bars, french fries, potato chips, processed lunch meats, candy, flour tortillas, brown rice syrup, meat substitutes, soy sauce, preseasoned meats, cheesecake filling, and eggs served in restaurants (a gluten source is sometimes added to scrambled eggs before cooking, but eggs themselves are gluten-free) may also contain gluten.4
Gluten is composed of glutenin and gliadin. Glutenin is the sticky portion that gives gluten its strength and elasticity. Gliadin is the protein that triggers an immune reaction in individuals with gluten-related allergies.5 A rising number of individuals are reporting gluten-mediated reactions, whether it is an allergy to wheat, sensitivity to products containing gluten, or the autoimmune disorder celiac disease.5
SCI-COMM STUDIOS/SCIENCE PHOTO LIBRARY
Wheat allergy is an immunological reaction to wheat proteins initiated by immunoglobulin E (IgE), an antibody found in the body that plays a significant role in the development of allergies.2 IgE attaches to allergens and initiates the dissemination of substances from mast cells that create inflammation. Once IgE attaches to mast cells, allergic reactions may ensue (Figure 1).6
Wheat allergy is one of the top eight food allergies in the United States.2,7 According to the US Food and Drug Administration (FDA), 0.4% of American adults have a wheat and/or gluten allergy.5 A wheat allergy usually manifests around infancy and is often outgrown by adolescence. Those with wheat allergies may have other food sensitivities such as to eggs or milk. A skin prick or blood test is needed to diagnose a wheat allergy.7 Symptoms include rash, wheezing, lip swelling, abdominal pain, and diarrhea.8 In severe cases, anaphylaxis can occur.2
Nonceliac gluten sensitivity is a gluten reaction in which both allergic and autoimmune mechanisms have been ruled out.9 It is defined by symptoms that appear when gluten is ingested and symptoms disappear with the removal of gluten from the diet.10 Approximately 6% of the US population has nonceliac gluten sensitivity.9,10 Symptoms include diarrhea, constipation, bloating, fatigue, depression, “foggy mind,” and headaches.10 There is no specific diagnostic tool for nonceliac gluten sensitivity; however, a gluten-free diet may be recommended in order to achieve a conclusive diagnosis.9,10
Celiac disease, also known as celiac sprue, is an autoimmune disorder that causes inflammation and damage to the villi of the small intestine when gluten is ingested.2 The undigested gluten causes an immunological response and creation of antibodies. Unfortunately, the antibodies don’t simply attack the gliadin in gluten, they also attack the tissue lining the intestines. This destructive response creates atrophy of the intestinal villi and causes malabsorption of nutrients, leading to nutritional deficiencies.2 The difference between nonceliac gluten sensitivity and celiac disease is that nonceliac gluten sensitivity does not result in an antibody reaction or intestinal damage.
There are more than 300 symptoms related to celiac disease, including diarrhea, constipation, abdominal distension, abdominal pain, vomiting, and poor growth.11–13 Approximately 3 million Americans or one in 133 are affected by celiac disease.11 Among specific ethnicities, such as Hispanic, Black, and Asian, the average is approximately one in 236 people.11 Sixty percent of children and 41% of adults diagnosed with celiac disease, however, remain asymptomatic.11
While IgA and immunoglobulin G (a type of antibody) serum tests aid in the diagnosis of celiac disease, intestinal biopsies must be performed to confirm a diagnosis.12 In the US, it takes an average of 4 years to reach a clinical diagnosis of celiac disease once symptoms are present.11 Age also impacts disease status, as older adults are at increased risk of developing celiac disease. The early diagnosis of celiac disease helps prevent further systemic complications, but just because a patient once tested negative for celiac disease does not mean he or she will never develop the disease.14 Untreated celiac disease can lead to osteoporosis, infertility, neurological conditions, nutrient deficiencies, and, in some cases, cancer.11
MANAGEMENT OF GLUTEN-MEDIATED REACTIONS
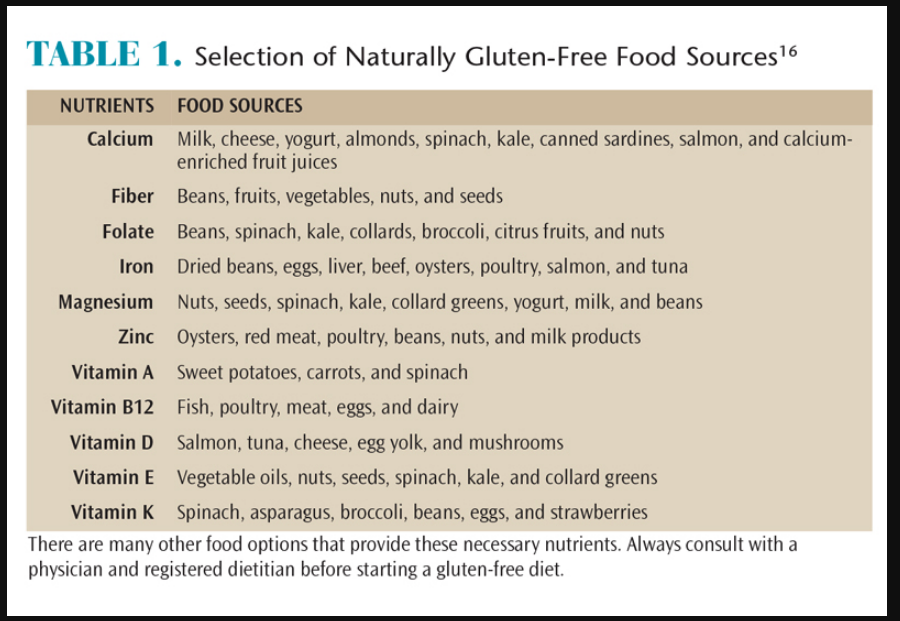
Currently, the only treatment for gluten-mediated reactions is to follow a strict gluten-free diet. In 2014, the FDA introduced new regulations for labeling packaged foods. In order to be considered gluten-free, packaged foods must contain less than 20 ppm of gluten.8,15 More than 2,000 gluten-free food items are now available.11 However, individuals with celiac disease have more to consider than just eliminating gluten from their diets. They must consume increased amounts of iron, calcium, thiamin, riboflavin, niacin, and folate to prevent deficiencies caused by atrophy of the intestinal villi.8 Table 1 lists a variety of fresh gluten-free foods that provide these and other nutrients.16 Patients with gluten-mediated reactions should eat a variety of whole foods such as fruits, vegetables, and lean proteins, as well as gluten-free grains.13 The FDA recommends that everyone, including those on a gluten-free diet, should avoid overly processed foods and keep the intake of refined sugars and saturated fats to a minimum to maintain health.17
*Click to View
Processed gluten-free products, while convenient, are not necessarily healthy options. Research shows that processed gluten-free products have high levels of lipids, sugars, and salt.18 A high consumption of carbohydrates may also lead to weight gain and increased caries risk. Consuming processed gluten-free products may lead to low intake of fiber among those with celiac disease.8 Consuming whole, nutritious, gluten-free foods can provide an adequate intake of fiber, vitamins, and minerals.8
Following a strictly gluten-free diet can be difficult without nutritional knowledge. Registered dietitians play a critical role in the management of gluten-mediated reactions.13 Table 2 provides examples of gluten-free meals.19 Vitamin supplements may be recommended by a physician or registered dietitian if a patient has nutritional deficiencies.
ORAL MANIFESTATIONS AND DENTAL TREATMENT MODIFICATIONS
The most commonly researched oral manifestations of celiac disease are enamel defects and recurrent aphthous stomatitis.20 Additional oral manifestations include atrophic glossitis, angular cheilitis, petechiae, delayed eruption of teeth, reduced salivary flow, excessive mucous production, oral malodor, dysgeusia, gingivitis, periodontal diseases, oral lichen planus, and oral/esophageal cancer.20,21 Enamel defects accompanying celiac disease include hypomineralization and hypoplasia. These are most often found on incisors and molars of permanent teeth and occur when enamel formation is interrupted.20,21 Enamel defects are present in 51% of individuals with celiac disease.20 The age of the disease’s onset determines if enamel defects are linked to the disease. Restorative treatment can be completed to correct discolored enamel and defects. Despite these enamel defects, children with celiac disease who follow a gluten-free diet are at a lower risk of caries than controls.21
Recurrent aphthous stomatitis, also known as an aphthous ulcer, is a common condition characterized by painful ulcerations of the oral mucosa. It frequently appears in conjunction with celiac disease.22 Etiological factors for aphthous stomatitis include genetic and environmental elements.22 Several methods of treatment for aphthous stomatitis exist, but systematic reviews indicate that no single treatment is superior.23 Pain control and prevention need to be addressed when recurrent aphthous stomatitis is present. Pain control can be provided with over-the-counter pain relievers or topical agents. A daily supplement of vitamin B12 may help to prevent recurrent aphthous stomatitis.24 B12 is a simple and inexpensive preventive agent that is readily available at pharmacies or consumed through diet.

*Click to View
While a gluten-free diet generally consists of fresh fruits and vegetables, low-fat dairy, and lean meats, patients who rely on processed gluten-free products may be consuming more cariogenic foods than normal. Fluoride application should be considered for patients with an increased risk for dental caries. Professional application and home fluoride use are beneficial for reducing caries risk. Fluoride regimens may include twice daily use of 0.05% sodium fluoride mouthrinse and professional application of sodium fluoride varnish every 3 months or daily use of 1.1% sodium fluoride toothpaste with professional application of sodium fluoride varnish every 3 months to 4 months.16
Dental hygienists may be the first health care professional to address gluten-mediated reactions with patients. Patients who present with oral symptoms consistent with celiac disease, such as enamel defects and/or recurrent oral aphthous ulcers, should be asked about other clinical symptoms of the disease including abdominal pain, diarrhea, constipation, weight loss, poor growth, anemia, and extreme fatigue. Inquiring about a family history of celiac disease is also appropriate, as the presence of first or second degree relatives with the disease increases the likelihood of a positive diagnosis.11 Patients who present with symptoms of celiac disease should be referred to a physician for diagnosis and treatment.
Several gluten-free dental products can be purchased for use during dental procedures as well as for home utilization, including prophy paste, toothpaste, and chlorhexidine gluconate mouthrinse. Researching product labels and manufacturer websites can help to identify these products. If orthodontic treatment is needed, the orthodontist needs to review the materials used to ensure they are gluten free. A recent study shows that one type of acrylic used to make retainers contains a plasticized methacrylate polymer, which is a nondietary source of gluten.12 Failure to avoid this plastic may lead to long-term exposure to gluten from the oral appliance. Other plastics found in the dental office may trigger or exacerbate the disease, such as those in dental equipment.12
CONCLUSION
Dental hygienists can play an important role in identifying unrecognized celiac disease and in counseling patients on making healthy dietary choices. While the number of gluten-free food products has grown, consuming a lot of processed foods, regardless of gluten content, does not promote health. Therefore, patients following a gluten-free diet should be counseled to seek out low carbohydrate gluten-free products, and most important, consume more fresh fruits and vegetables, dairy, and lean sources of protein, as these are all naturally gluten-free.
REFERENCES
- Nunes K. Mintel: Gluten free will hit $8.8 billion in sales in 2014. Available at: foodbusinessnews.net/ articles/news_home/Consumer_Trends/2014/11/Min tel_Gluten_free_will_hit_88.aspx?ID=%7B3564EE6F- 582C-4579-8BA8-8D995979CAC3%7D. Accessed September 5, 2015.
- American Celiac Disease Alliance. What is Celiac Disease? Available at: americanceliac.org/celiacdisease. Accessed September 5, 2015.
- Celiac Disease Foundation. Gluten-Free Diet. Available at: celiac.org/live-glutenfree/ glutenfreediet. Accessed September 5, 2015.
- Celiac Disease Foundation. Sources of Gluten. Available at: celiac.org/live-glutenfree/ glutenfreediet/sources-of-gluten. Accessed September 5, 2015.
- Leonard MM, Vasagar B. US Perspective on gluten-related diseases. Clin Exp Gastroenterol. 2014;7:25–37.
- Asthma and Allergy Foundation of America. IgE’s Role in Allergic Asthma. Available at: aafa.org/display.cfm?id=8&sub=16&cont=54. Accessed September 5, 2015.
- University of Chicago Celiac Disease Center. Allergies and Intolerance. Available at: cureceliacdisease.org/wpcontent/uploads/2011/09/C DCFactSheets9_Allergies.pdf. Accessed September 5, 2015.
- Saturni L, Ferretti G, Bacchetti T. The gluten-free diet: safety and nutritional quality. Nutrients. 2010;2:16–34.
- Tonutti E, Bizzaro N. Diagnosis and classification of celiac disease and gluten sensitivity. Autoimmun Rev. 2014;13:472–476.
- Catassi C, Bai JC, Bonaz B, et al. Non-celiac gluten sensitivity: the new frontier of gluten related disorders. Nutrients. 2013;5:3839–3853.
- The University of Chicago. Celiac Disease Facts and Figures. Available at: uchospitals.edu/ pdf/ uch_ 007937.pdf. Accessed September 5, 2015.
- Memon Z, Baker S, Khan A, Hashmi H, Gelfond D. An Orthodontic Retainer Preventing Remission in Celiac Disease. Clinical Pediatrics. Available at: cpj.sagepub.com/ content/52/11/1034.long. Accessed September 5, 2015.
- Penagini F, Dilillo D, Meneghin F, Mameli C, Fabiano V, Zuccotti GV. Gluten-free diet in children: an approach to a nutritionally adequate and balanced diet. Nutrients. 2013;5:4553–4565.
- Catassi C, Kryszak D, Bhatti B, et al. Natural history of celiac disease autoimmunity in a USA cohort followed since 1974. Ann Med. 2010;42:530–58.
- United States Food and Drug Administration. Foods Labeled Gluten-Free Must Now Meet FDA’s Definition. Available at: fda.gov/Food/NewsEvents/ ConstituentUpdates/ucm407867.htm. Accessed September 5, 2015.
- Darby ML, Walsh MM. Dental Hygiene Theory and Practice. 4th ed. St. Louis: Saunders Elsevier; 2015:427,616-618.
- National Foundation for Celiac Awareness. Celiac Disease: 360. Available at: celiaccentral.org/ newly diagnosed. Accessed September 5, 2015.
- Mariani P, Viti MG, Montuori M, et al. The Gluten-free diet: a nutritional risk factor for adolescents with celiac disease? J Pediatr Gastroenterol Nutr. 1998;27:519–523.
- Children’s Digestive Health and Nutrition Foundation along with the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition. Gluten-free Diet Guide for Families. Available at: gluten-freedietguideweb.pdf. Accessed September 5, 2015.
- Rashid M, Zarkadas M, Anca A, Limbeack H. Oral manifestations of celiac disease: a clinical guide for dentists. J Mich Dent Assoc. 2011;93:42–46.
- de Carvalho FK, de Queiroz AM, Bezerra da Silva RA, et al. Oral aspects in celiac disease children: clinical and dental enamel chemical evaluation. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;119: 636–643.
- Saraceno R, Perugia C, Ventura A, Lore’ B, Chimenti S, Docimo R. Aphthous, coeliac disease and other dental disorders in childhood. G Ital Dermatol Venereol. April 9, 2015. Epub ahead of print.
- Brocklehurst P, Tickle M, Glenny A, et al. Systemic Interventions for Recurrent Aphthous Stomatitis (mouth ulcers). Cochrane Database Syst Rev. 2012;9:CD005411.
- Liu H, Chiu S, Chen K. Effectiveness of vitamin B12 on recurrent aphthous stomatitis in long term care: a systematic review. JBI Database of Systematic Reviews and Implementation Reports. 2013;11(2):281–307.
From Dimensions of Dental Hygiene. October 2015;13(10):53–56.
