 FELIX MIZIOZNIKOV / ISTOCK / THINKSTOCK
FELIX MIZIOZNIKOV / ISTOCK / THINKSTOCK
The Impact of National Origin on Caries Risk
Dental hygienists are well positioned to address culturally related risk factors for early childhood caries.
The dental caries rate among school-age children living in industrialized countries ranges from 60% to 90%.1 Dental caries continues to be the most common chronic childhood illness in the United States.2
The American Academy of Pediatric Dentistry defines early childhood caries (ECC) as the presence of dental caries in children age 71 months or younger.3 Nursing bottle decay and baby bottle decay are common terms for ECC.3 Over the past 20 years, research has shown a decline in the incidence and prevalence of ECC in developed countries, such as the US; however, caries remains highly prevalent in minority populations.4,5
Children from low socioeconomic backgrounds are twice as likely to experience dental caries than children from higher socioeconomic backgrounds.6,7 Furthermore, children from low-income families have more serious caries and are less likely to receive dental care than those of higher socioeconomic status.7
Race and ethnicity are risk factors for dental caries development.8 According to recent US government data, untreated caries is twice as common among Hispanic and Black children age 2 to 8 than in white children in the same age group.8 Additional risk factors include migrancy, parental education level, and dietary practices,6 as well as the habits and beliefs of parents/caregivers, especially mothers.2,7,9 Oral health professionals need to be aware of the influence that ethnic and cultural factors exert on oral health—specifically regarding caries prevention and education.
ORIGIN OF FOREIGN-BORN POPULATIONS LIVING IN THE UNITED STATES
Immigrants are individuals who permanently reside in a country different from their country of origin. In 2013, more than 13 million legal immigrants were living in the US.10 But the total number of foreign-born residents is much higher, as the 13 million figure does not include undocumented residents.10 Like immigrants, refugees seek to resettle in another country, but their decisions to relocate are made under duress. They may be unable to return to their home countries because of threats of persecution, violence, or other risks.11
More than 40% of the immigrants who relocated to the US between 2011 and 2013 are from Asia.12 The second largest group came from Mexico and the Caribbean.12 Most refugees who resettled in the US during the same interval are from Myanmar (formerly Burma), Bhutan, and Iraq.13 Recent government data indicate that in 2015, one-third of refugees entering the US were from Near East/Southwest Asia, which includes Iraq, Iran, Bhutan, and Afghanistan.14
CULTURAL INFLUENCES
Familial behaviors related to oral health are often influenced by cultural practices and norms.9 A child’s exposure to cariogenic bacteria can come through direct or indirect contact, and is considered a significant risk factor for ECC.9,15,16 A child may acquire the bacteria through contact with a parent’s/caregiver’s saliva.2,15,17 Behaviors such as testing children’s food before feeding them, as well as sharing food and eating utensils aid in the transfer of cariogenic bacteria from parent/caregiver to child.2,18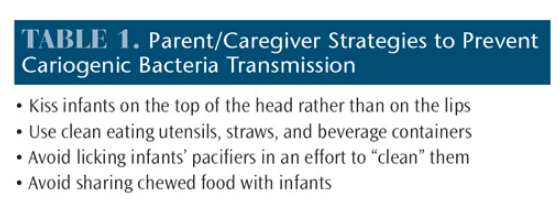
Parents/caregivers may be unaware that tooth decay is an infectious disease, so using simple terminology and sharing basic tips on how bacteria, or “germs” are transmissible can be useful in caries prevention efforts. While helping infants eat by prechewing their food is a common practice in some countries like Myanmar,19,20 it can enable the transmission of cariogenic bacteria. A discussion regarding the prevention of cariogenic bacteria transmission may be better received by parents/caregivers if oral health professionals compare it to other health strategies—such as washing hands to prevent the spread of infection—that are already used at home. Table 1 provides a list of parent/caregiver strategies to reduce the risk of transmission of cariogenic bacteria.
Children’s oral health statuses are associated with their parents’/caregivers’ oral health literacy.21 Health literacy refers to individuals’ abilities to process and understand health information in order to make sound health decisions.22 Immigrant mothers often have limited formal education compounded by poor communication skills, leading to low oral health status.9 Caregivers’ inadequate oral health knowledge is another contributing factor to ECC.2,9 Limited oral health knowledge has also been associated with adverse oral health behaviors such as failing to clean children’s teeth daily, putting children to bed with a bottle, and allowing children to frequently consume cariogenic foods and beverages.21
To compensate for the hardships previously faced in refugee camps, some foreign-born parents/caregivers may find it difficult to deny their children access to sugary foods and drinks.23 Also, differentiating between healthy and unhealthy options can be challenging for those who are unfamiliar with the language and food packaging of a new country.23 To improve parents/caregivers’ oral health knowledge, the caries process must be explained and the rationale provided for allowing only a bottle containing water in a child’s crib, avoiding prolonged or on-demand breastfeeding, routinely removing plaque biofilm from children’s teeth with a toothbrush and floss (if teeth are touching), and limiting a child’s consumption of sugar-containing beverages, including fruit juices.
The frequent intake of foods and drinks containing fermentable carbohydrates, such as crackers, soft drinks, and fruit juices, can increase a child’s risk for ECC. Eating behaviors established in infants as young as 6 months can impact children’s dietary habits at 12 months and 18 months.2 Healthy eating habits started in infancy may help reduce the risk of ECC.2
In some cultures, primary teeth are considered unimportant. Providing children with sugary drinks in a bottle at bedtime or with pacifiers dipped in honey are common practices.24 One study found that several immigrant populations living in America believed that children who are breastfed do not get caries.19 Additionally, some cultures think that a mother’s diet during pregnancy can cause her child to have “soft teeth.”24
Some ethnic cultures believe the purpose of brushing teeth is to freshen breath—not to prevent oral diseases.24 Foreign-born individuals may be afraid their teeth will be loosened by dental cleanings. Therefore, many immigrant populations avoid preventive dental care, only seeking treatment when there is oral pain. Research indicates that some immigrant older adults believe that the Western approach of treating primary teeth is too aggressive; thus, they may be less trusting of oral health professionals than younger immigrants.24
Prior experiences with unhealthy drinking water in their countries of origin may discourage immigrants from drinking tap water after resettlement.23 Some find the smell and the taste of tap water to be off-putting, as was reported by a mother who was accustomed to drinking fresh water from an underground spring in her homeland.23 Also, some immigrant populations may choose to drink bottled water because it is considered a sign of wealth.23 Furthermore, individuals may not be aware of the oral health benefits gained through community water fluoridation.19,23 As a result, their children may consume less fluoridated tap water, with sugar-containing drinks often provided as alternatives.23
Providing printed pamphlets and brochures to patients in their native languages may help improve oral health outcomes. English- and Spanish-language brochures are available to oral health professionals at no charge from the National Institute of Dental and Craniofacial Research at: nidcr.nih.gov/OralHealth/Topics/ToothDecay.
CONCLUSION
The oral health of children can be influenced by familial cultural practices and beliefs among racial/ethnic populations.9 Dental hygienists are well-positioned to identify children at risk for developing dental caries and to provide disease-prevention education. Providing prevention education to parents/caregivers at the earliest possible opportunity can be an important step in dental caries reduction. Oral health providers’ awareness of the difficulties and challenges faced by foreign-born populations living in the US can aid in their improved understanding of patients’ attitudes. Tailoring questions, responses, and recommendations in a culturally sensitive manner can provide improved oral health outcomes for all patients.
References
-
- Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century—the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003;31(Suppl 1):3–23.
- Nunn ME, Dietrich T, Singh HK, Henshaw MM, Kressin NR. Prevalence of early childhood caries among very young urban Boston children compared with US children. J Publ Health Dent. 2009;69:156–162.
- American Academy of Pediatric Dentistry. Policy on Early Childhood Caries: Classifications, Consequences, and Preventive Strategies. Available at: aapd.org/media/Policies_Guidelines/P_ECCClassifications.pdf. Accessed February 10, 2016.
- Leong PM, Gussy MG, Barrow SL, De Silva-Sanigorski A, Waters E. A systematic review of risk factors during first year of life for early childhood caries. Int J Paediatr Dent. 2013;23:235–250.
- Plutzer K, Spencer AJ. Efficacy of an oral health promotion intervention in the prevention of early childhood caries. Community Dent Oral Epidemiol. 2008;36:335–346.
- Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N. Parental influence and the development of dental caries in children aged 0-6 years: a systematic review of the literature. J Dent. 2012;40:873–885.
- National Institute of Dental and Craniofacial Research. National Call to Action to Promote Oral Health. Available at:?nidcr.nih.gov/DataStatistics/SurgeonGeneral/NationalCalltoAction/nationalcalltoaction.htm. Accessed February 10, 2016.
- Dye BA, Thornton-Evans G, Li X, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011–2012. Available at:?cdc.gov/nchs/data/databriefs/db191.pdf. Accessed February 10, 2016.
- De Castilho ARF, Mialhe FL, De Souza Barbosa T, Puppin-Rontani RM. Influence of family environment on children’s oral health: A systematic review. J Pediatr. 2013;89:116–123.
- Baker B, Rytina N. Estimates of the lawful permanent resident population in the United States: January 2013. Available at: dhs.gov/publication/estimates-lawful-permanent-resident-population-2013. Accessed February 10, 2016.
- Refugee Definition Training Module. Washington, DC: United States Citizenship and Immigration Services; 2013:1–26.
- Monger R, Yankay J. Annual Flow Report. US Lawful Permanent Residents: 2013. Available at:?dhs.gov/sites/default/files/publications/ois_lpr_fr_2013.pdf. Accessed February 10, 2016.
- Martin DC, Yankay JE. Annual Flow Report. August 2014. Refugees and Asylees: 2013. Available at:?dhs.gov/sites/default/files/publications/ois_rfa_fr_2013.pdf. Accessed February 10, 2016.
- American Immigration Council. An Overview of US Refugee Law and Policy. Available at: immigrationpolicy.org/just-facts/refugees-fact-sheet. Accessed February 10, 2016.
- Gussy MG, Waters E, Kilpatrick NM. A qualitative study exploring barriers to a model of shared care for preschool children’s oral health. Brit Dent J. 2006;201:165–170.
- Parisotto TM, Steiner-Oliveira C, Silva CM, Rodrigues LK, Nobre-dos-Santos M. Early childhood caries and mutans streptococci: A systematic review. Oral Health Prev Dent. 2010;8:59–70.
- Chaffee BW, Gansky SA, Weintraub JA, Featherstone JDB, Ramos-Gomez FJ. Maternal oral bacterial levels predict early childhood caries development. J Dent Res. 2014;93:238–244.
- Gussy MG, Waters EG, Walsh O, Kilpatrick NM. Early childhood caries: Current evidence for aetiology and prevention. J Paediatr Child Health. 2006;42:37–43.
- Finnegan DA, Rainchuso L, Jenkins S, Kierce E, Rothman A. Immigrant caregivers of young children: Oral health beliefs, attitudes, and early childhood caries knowledge. J Community Health. September 14, 2015. Epub ahead of print.
- Van Palenstein Helderman WH, Soe W, van’t Hof MA. Risk factors of early childhood caries in a Southeast Asian population. J Dent Res. 2006;85:85–88.
- Bridges SM, Parthasarathy DS, Wong HM, Yiu CKY, Au TK, McGrath CPJ. The relationship between caregiver functional oral health literacy and child oral health status. Patient Educ Couns. 2014;94:411–416.
- US Department of Health and Human Services. Health Literacy Fact Sheet: Health literacy Basics. Available at: health.gov/communication/literacy/ quickguide/factsbasic.htm. Accessed February 10, 2016.
- Nicol P, Al-Hanbali A, King N, Slack-Smith L, Cherian S. Informing a culturally appropriate approach to oral health and dental care for preschool refugee children: A community participatory study. BMC Oral Health. 2014;14:69.
- Butani Y, Weintraub JA, Barker JC. Oral health-related cultural beliefs for four racial/ethnic groups: Assessment of the literature. BMC Oral Health. 2008;8:26.
From Dimensions of Dental Hygiene. March 2016;14(03):28–30.

{kind=link}