 GMUTLU/E+/GETTY IMAGES PLUS
GMUTLU/E+/GETTY IMAGES PLUS
Technology-Related Infection Control Challenges
Understanding how to manage technology in the dental setting requires knowledge and application of infection control guidelines.
This course was published in the August 2018 issue and expires August 31, 2021. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss infection control for patient care items.
- Explain best practices for managing surfaces and equipment.
- Identify guidelines for using surface and equipment barriers.
- List techniques for protecting semicritical devices and technology.
Disease transmission in dentistry has always been a concern with bloodborne pathogens, such as hepatitis B virus (HBV) and hepatitis C virus. The emergence of human immunodeficiency virus (HIV) in the 1980s brought this issue to the forefront. The United States Centers for Disease Control and Prevention (CDC) and the Occupational Safety and Health Administration (OSHA) provide evidence-based rules, recommendations, and guidance related to safety in the provision of patient care.
Oral health professionals must be well versed in OSHA and CDC guidelines when working with technology and related equipment. Two OSHA standards that dental offices must comply with are the OSHA Bloodborne Pathogen Standard and the Hazard Communication Standard.1,2 The OSHA Bloodborne Pathogen Standard mandates protection for all dental team members who may be exposed to blood and other potentially infectious materials.1 Employers are required to provide protection for employees through the use of personal protective equipment (PPE), such as gloves, masks, protective eyewear, and protective garments (lab coats and their laundering); hepatitis B virus (HBV) vaccination; safe work practices, including safety devices (sharps containers, needle recapping devices); and annual training.1
The OSHA Hazard Communication Standard mandates protection from chemical hazards in the workplace. Employers must provide training and PPE for employees handling chemicals, including surface disinfectants, cleaning agents, and dental materials.2 All chemicals must contain a safety data sheet that provides information on handling, including methods for storage and disposal, and first aid instructions in the event of accidental exposure.2
The 2003 CDC Guidelines for Infection Control in Dental Health-Care Settings contain comprehensive guidance related to all aspect of infection control and prevention.3 The CDC published companion documents in 2016 outlining recommendations and basic expectations for safe care.4
PATIENT CARE ITEMS
Oral health professionals must understand CDC guidelines when working with technology. Dental instruments are categorized into three levels related to sterilization: critical, semicritical, and noncritical.3 Critical instruments (curets or burs) penetrate soft tissue or contact bone or the bloodstream and, therefore, must be heat sterilized. Semicritical instruments (mouth mirror, amalgam condensers, reusable impression trays) contact mucous membranes but do not penetrate soft tissues; however, they should also be sterilized whenever possible, if heat tolerant. Table 1 outlines these categories. Sterilization refers to a process that kills all living microorganisms, including bacterial spores, by one of three methods: heat, gas, or chemical.5 Noncritical items (X-ray tube heads, blood pressure cuffs, or stethoscopes) only contact the skin and can be disinfected. Disinfection (with a spray or a wipe) is a process that kills many microorganisms, but not all bacterial spores.5
![]() SURFACES AND EQUIPMENT
SURFACES AND EQUIPMENT
 SURFACES AND EQUIPMENT
SURFACES AND EQUIPMENT Clinicians need to understand the instrument reprocessing cycle, as well as how to handle surfaces in the operatory, many of which include technology and related equipment that may not be heat tolerant (sterilizable). There are two types of environmental surfaces in the dental operatory: clinical contact surfaces and housekeeping surfaces. Clinical contact surfaces include items frequently touched during treatment (instruments, devices, equipment, switches, and handles) that require sterilization or disinfection between patients, depending on the level of sterilization (critical, semicritical, or noncritical). Housekeeping surfaces (floors, countertops) are not directly touched during treatment and only require routine cleaning.3
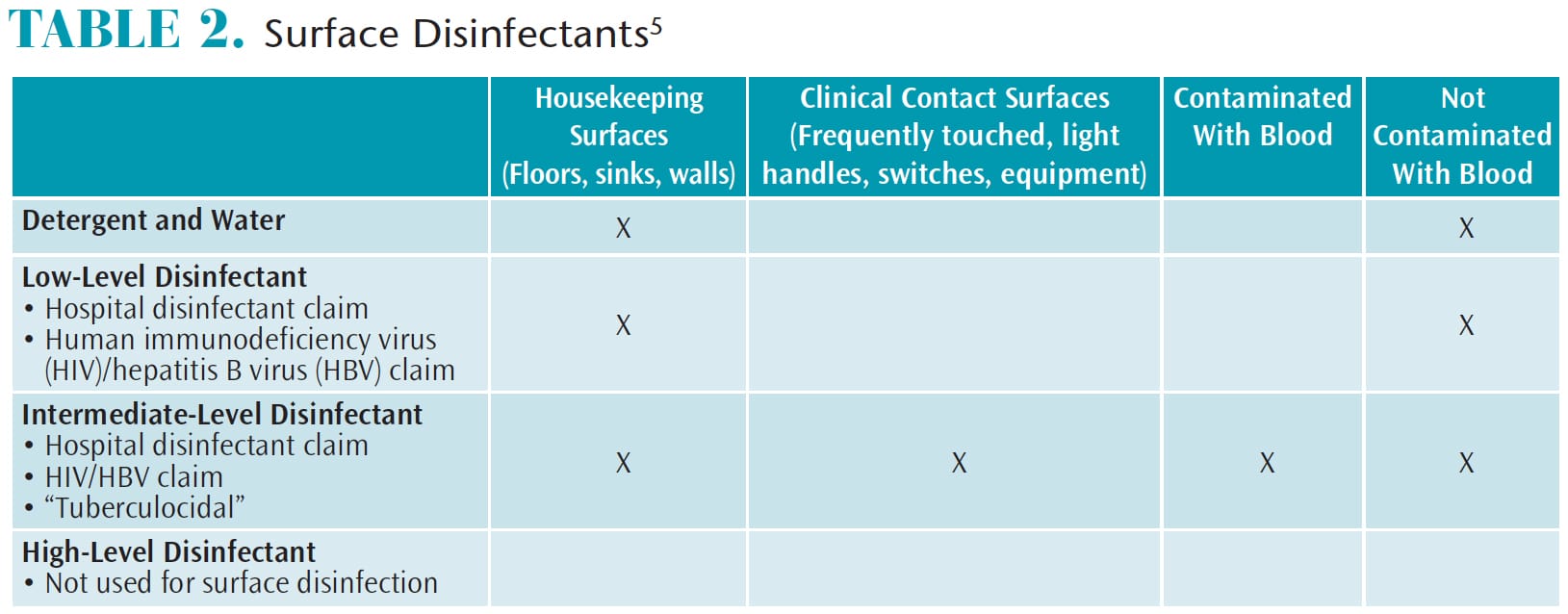
Surface disinfectants are used on both clinical contact and housekeeping surfaces. Many products are available and choosing one requires some research. There are three types of surface disinfectants: low level, intermediate level, and high level (Table 2).3Different types of surfaces in various settings require different levels of disinfection. For example, hospital rooms are different from dental operatories where splash and spatter occur more frequently.
Low-level disinfectants carry a “hospital disinfectant” claim, meaning the product is used on noncritical housekeeping surfaces not contaminated by blood or other bodily fluids.3 Low-level disinfectants are effective against the test organisms Staphylococcus aureus, Salmonella, and Pseudomonas, and are effective against HIV and HBV.3 HBV can last up to 1 month on surfaces.3 Hospitals generally use low-level disinfectants on most surfaces because they are not generating aerosols and spatter.
Intermediate-level disinfectants also carry a “hospital disinfectant” claim and include the same characteristics as low-level disinfectants but are also effective against the hearty test organism Mycobacterium tuberculosis. This means it is considered “tuberculocidal” and is effective for use on items or surfaces contaminated with blood or other bodily fluids.3 It is wise to use intermediate-level disinfectants on all surfaces in the dental operatory because aerosols, blood spatter, and other fluids may not be visible. Using one product improves staff compliance and can be cost effective. As long as the label claims tuberculocidal activity, it is considered an intermediate-level disinfectant. High-level disinfectants (glutaraldehyde) are not used on surfaces but are indicated for use on semicritical items that cannot be heat sterilized and must be submerged for 3 hours to 10 hours.3
Surface disinfectants require cleaning or removing blood or other bodily fluids first by a spray and wipe method, or wipe and discard method.3 Next, the surface must be sprayed or wiped again and left wet or damp for the manufacturer’s recommended contact time (varies between 1 minute and 10 minutes). Failure to perform both steps results in surfaces that are not disinfected.
BARRIERS
Barriers made from impervious plastic are alternatives or adjuncts to surface disinfection. Barriers are placed on clean surfaces at the beginning of the day and changed between patients. The surface underneath does not need to be disinfected as long as the barrier was not compromised or visibly soiled.3,4 Barriers are one-time use items recommended for difficult-to-clean items (fixed equipment, light handles, switches, chair controls, radiograph tube head, and exposure buttons), shortening operatory turnaround time.3 A combination of barriers and surface disinfection are often recommended by manufacturers of technology and related equipment.
![]() CHALLENGES
CHALLENGES
 CHALLENGES
CHALLENGES Making sense of infection control guidelines with electronic devices is challenging. Adequate knowledge regarding the safety of each product is critical. Accessing manufacturer instructions for use and their updates for each device is an important step in protecting costly equipment. Striking a balance between proper infection control and protection of the device is key.
Multiple brands of electronic devices are used in dentistry today. The 2003 CDC guidelines recommend consulting manufacturer instructions for use for each device.3 These should provide detailed instructions on the cleaning and maintenance required to safely protect the device and abide by infection control protocols. The US Food and Drug Administration (FDA) also provides suggestions on the labeling and instructions for use of medical devices.6 The FDA asserts that manufacturer instructions should include details on disassembly, cleaning, rinsing, disinfection/sterilization, drying, reassembly of the device, and use of disposable sheathing for other portions of the device. When the user manual is not available, the instructions for use may be found on the manufacturer’s website or by contacting the manufacturer. All users should read and understand the specific device’s sterilization and/or disinfection recommendations, which may be unique to the brand used in the dental office.
SEMICRITICAL DEVICES
Each type of device has its own instructions for use regarding sterilization or disinfection, but oral health professionals should stay abreast of updates to infection control guidelines. Heat sterilization is required for semicritical items whenever possible; however, many devices have a combination of critical and noncritical components that cannot withstand heat sterilization.
Computer mouse and keyboard. Electronic health record management necessitates the frequent use of mice and keyboards, raising the risk that they will become breeding grounds for contamination. Reynolds et al7 found that 80% of infections occurred due to cross-contamination of hand-to-hand contact and other object-to-hand contact. Al-Ghamdi et al8 determined that as many as 91% of office mice and keyboards were contaminated. Hartmann et al9 found 26 contaminated samples from keyboards and mice compared with 18 contaminated samples from other fomites in patient rooms. The keyboard and mouse contain the majority of microorganisms and pose greater risks for cross-contamination.9 They are easily contaminated surfaces and must have barriers placed before and after use, and they must be disinfected between uses.
Care must be taken when disinfecting mice and keyboards to avoid electrical shock and to maintain the electrical components, but disinfectants are effective. Rutala et al10 found that after testing six disinfectants (all containing chlorine, alcohol, or phenol, and quaternary ammonium) “all disinfectants, as well as sterile water control, were effective at removing or inactivating more than 95% of the test bacteria.” Disinfection did not damage the mice or keyboards in this study.10 Using disinfectants per manufacturer instructions for use regarding the correct contact time and avoiding saturating or soaking the delicate electronic components are critical to maintaining equipment while following infection control guidelines.
Radiography equipment. Plastic barriers should be used, along with a disinfectant containing less than 17% alcohol on portable handheld radiography units.11 A study by Hokett et al12 found contamination of digital radiograph sensors as high as 51% underneath a plastic barrier. Malta et al13 also demonstrated that disinfection of X-ray sensors and components were not common practice in dental offices based on the 78 intraoral and extraoral X-ray systems that tested positive for cocci, Gram-negative bacilli, and fungi after use. Intraoral cameras are used similarly to digital radiography, suggesting they pose the same cross contamination risk. Both digital radiography sensors and intraoral cameras recommend barrier protection and intermediate level disinfectants4 and wiping with isopropyl alcohol and gauze for the intraoral camera lens.14,15
Handpieces. Some cordless prophylaxis handpieces have a removable head, and heat sterilization is recommended after each use. The remaining parts of the unit should be disinfected with an intermediate-level disinfectant. Handpieces connected to the dental unit air and water line (that are not cordless) should be heat sterilized between uses.3
Light, laser, and other devices. Near-infrared transillumination light that uses electromagnetic technology to create images are gaining popularity.16 One product has a plastic guiding sheath that is heat tolerant and autoclavable. The rest of the unit must be disinfected with an intermediate-level disinfectant, and the direct lens can be wiped with isopropyl alcohol on a gauze.16 Another caries detection device uses a low-powered pulsating laser. The pulses of laser light generate photothermal and luminescence responses that produce colors that represent healthy or unhealthy areas of decay and cracks within the tooth. There is a disposable plastic tip and a plastic sleeve that allows the laser to move through the plastic and not affect the quality of the light. The handle may be disinfected with an intermediate disinfectant approved for use on plastics. A computer-aided design/computer-aided manufacturing device that captures images to produce a three-dimensional product known as “same-day crowns” is frequently found in private practices. The mirror sleeve is removable and heat tolerant (autoclavable). The camera body itself should be disinfected by wiping with an intermediate-level disinfectant vs spraying.17 Oral cancer screening handheld devices or scopes illuminate the oral mucosa with a fluorescent light for direct visualization of normal mucosa vs abnormal mucosa to aid in the detection of oral cancer and abnormal lesions. The visual contrast can then be captured as an image. There are single use and disposable lens caps, and the rest of the unit can be disinfected with intermediate-level disinfection.
Cordless endodontic obturation systems combine a downpack heat source with a backfill extruder that heats and cools quickly.18Disposable and autoclavable tips, custom plastic sleeves, and intermediate-level disinfection are recommended. Curing lights require unique barriers specific to the manufacturer’s recommendations to ensure light quality and capability. Any intermediate-level disinfectant is acceptable. Keep in mind that all devices connected to a wall outlet must be unplugged prior to any disinfectant application and none of these devices should ever be directly sprayed with any disinfectant to avoid electrical shock.
BEST PRACTICES
Impervious plastic barriers are effective in the prevention of cross-contamination on devices. The 2003 CDC guidelines emphasize that barriers are effective for difficult-to-clean items, such as electronic devices.3 Barriers alone might not be adequate to prevent cross-contamination and may provide the clinician with a false sense of protection of semicritical items. A study by Choi19 found a perforation rate of 44% to 51% after use of a single plastic barrier (0.04 mm thickness) during intraoral digital sensor use. This warranted further disinfection with an intermediate-level disinfectant. The use of a 0.08 mm thick plastic barrier provided a superior perforation rate, although the thickness irritated soft tissues.19 Thicker barriers make capturing digital images more difficult, may inhibit the device’s effectiveness, and increase discomfort for patients.19 Imaging that depends on clear, direct contact with the tissues or teeth cannot be compromised due to the barrier, so thinner barriers are recommended for these devices. Barriers are recommended for all semicritical devices and the most effective thickness is a low-density polyethylene.19 Choosing the correct barrier with consideration to patient comfort is vital.
CONCLUSION
A combined approach including the use of barriers and intermediate-level disinfection appears to be best practice with regard to technology equipment. As with all good protocols, proper training and compliance with manufacturer instructions for use regarding each product are crucial. The protection and maintenance of expensive equipment are essential for longevity and function; however, health care professionals must keep the asepsis of each type of equipment in mind and follow prudent infection control guidelines. Oral health professionals may want to visit the “frequently asked questions” section on osap.org for additional information. The Organization for Safety, Asepsis, and Prevention supports safe dental visits and provides excellent resources to help oral health professionals adhere to both the CDC guidelines and OSHA regulations.
REFERENCES
- Occupational Safety and Health Administration. Bloodborne Pathogens Standard 29 CFR. 1910.1030. Available at: osha.gov/pls/oshaweb/owadisp.show_document?p_table=standards&p_id=1005 Accessed July 24, 2018.
- Occupational Safety and Health Administration. Hazard Communication Standard 29 CFR 1910.1200. Available at: osha.gov/pls/oshaweb/owadisp.show_document?p_table=standards&p_id=10099. Accessed July 24, 2018.
- Kohn WG1, Collins AS, Cleveland JL, et al. Guidelines for infection control in dental health-care settings—2003. MMWR Recomm Rep. 2003;52(RR-17):1–61.
- United States Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care. Available at: cdc.gov/oralhealth/infectioncontrol/guidelines/index.htm. Accessed July 24, 2018.
- Miller CH, Palenik CJ. Infection Control and Management of Hazardous Materials for the Dental Team. 4th ed. St. Louis: Mosby, Elsevier; 2010.
- United States Food and Drug Administration. Reprocessing Medical Devices in Health Care Settings: Validation Methods and Labeling by the Food and Drug Administration. Available at: fda.gov/downloads/medicaldevices/deviceregulationguidance/guidancedocuments/ucm25 3010.pdf. Accessed July 24, 2018.
- Reynolds KA, Watt PM, Boone SA, Gerba CP. Occurrence of bacteria and biochemical markers on public surfaces. Int J Environ Health Res. 2005;15:225–234
- Al-Ghamdi AK, Abdelmalek MA, Ashshi AM, Faidah H, Shukri H, Jiman-Fatani AA. Bacterial contamination of computer keyboards and mice, elevator buttons and shopping carts. African Journal of Microbiology Research. 2011;5(23):3998–4003.
- Hartmann B, Benson M, Junger A, et al. Computer keyboard and mouse as a reservoir of pathogens in an intensive care unit. J Clin Monit Comput. 2004;18:7–12.
- Rutala WA, White MS, Gergen MF, Weber DJ. Bacterial contamination of keyboards: efficacy and functional impact of disinfection. Infect Control Hosp Epidemiol. 2006;27:372–377.
- NOMAD. Frequently Asked Questions: FAQ Portable X-Ray. Available at: http://aribex.com/support/faq-portable-x-ray/. Accessed July 24, 2018.
- Hokett SD, Honey JR, Francisco R, Baisden MK, Hoen MM. Assessing the effectiveness of direct digital: radiography barrier sheaths and finger cots. J Am Dent Assoc. 2000;131:463–467.
- Malta CP, Damasceno NL, Ribeiro RA, Silva CSF, Devito KL. Microbiological contamination in digital radiography: evaluation at the radiology clinic of an education institution. Acta Odontal Latinoam. 2016;29:239–247.
- Schick by Sirona. Cleaning and Disinfecting Sensors. Available at: schickbysirona.com/items.php?itemid=7669. Accessed July 24, 2018.
- Schick by Sirona. Cleaning and Disinfecting Cameras. Available at: schickbysirona.com/items.php?itemid=8749. Accessed July 24, 2018.
- Dexis. CariVu User Manual and Manufacturer’s Guidelines. Available at: dexis.com/carivu. Accessed July 24, 2018.
- Sirona. Omnicam User Manual. Available at: http://manuals.sirona.com/en/digital-dentistry/cerec-chairside-solutions/cerec-ac-with-cerec-omnicam.html. Accessed July 24, 2018.
- Patterson Dental. System B™ Cordless Obturation System—Cordless Fill Device. Available at: pattersondental.com/Supplies/ItemDetail/071137363. Accessed July 24, 2018.
- Choi JW. Perforation rate of intraoral barriers for direct digital radiography. Dentomaxillofac Radiol. 2015;44:20140245.
From Dimensions of Dental Hygiene. August 2018;16(8):30-33.
